
Abstract
A prospective online study, consisting of 203 participants ages 18 and older who smoked waterpipe (hookah) within the last 30 days, examined how brief messaging about harms of burning charcoal to heat waterpipe tobacco (shisha) influenced knowledge of toxicants released by using charcoal and perceived harms of using charcoal. Participants were randomized to either a control or to an educational arm that reviewed toxicants released by burning charcoal and the health consequences. Participants in the educational relative to the control arm perceived charcoal as more harmful, were more knowledgeable of toxicants released by burning charcoal, and expressed a stronger desire to quit. Effects were sustained a week later. Brief messages about the harms of burning charcoal were effective and may be used to educate the public about the harms of waterpipe tobacco smoking.
Introduction
In the United States waterpipe (hookah) tobacco smoking (WTS) is a public health concern, especially among youth and younger adults. For example, among 19–30-year-olds, past year prevalence of use during 2019 was 9.3% (Schulenberg et al., 2020); in 2019, among 12th graders, 4.0% reported past 30-day WTS (Schulenberg et al., 2020). Waterpipe smokers face health risks including cancer, poorer pulmonary function, and heart disease (Akl et al., 2010; Raad et al., 2011; Waziry et al., 2017) due to toxicants in the smoke (e.g., carcinogenic polycyclic aromatic hydrocarbons (PAHs), volatile aldehydes, and carbon monoxide (CO), Al Rashidi et al., 2008; El-Nachef & Hammond, 2008; Monzer et al., 2008; Primack et al., 2016; Sepetdjian et al., 2008; Shihadeh, 2003).
Many of these toxicants are produced by the combustion of charcoal to heat the waterpipe tobacco (shisha). For example, Monzer and colleagues (Monzer et al., 2008), using a waterpipe smoking machine, found that about 90% of the CO and 75–92% of PAH compounds found in hookah tobacco smoke came from the charcoal. Elsayed and colleagues (2016) reported that raw charcoal used for WTS contained heavy metals such as zinc, iron, cadmium, and lead, some at higher levels than cigarettes. In addition, they identified seven carcinogens (e.g., benzofuran, quinoline, styrene), 39 central nervous system depressants, and 31 respiratory irritants in machine-generated smoke resulting from five different charcoal brands (Elsayed et al., 2016). The extant data show that burning charcoal to heat shisha contributes to smoker toxicant exposure.
Little attention has been devoted to educating the public about the harms of using charcoal to heat shisha. In a recent study, Lipkus and colleagues examined young adult hookah smokers’ knowledge of toxicants produced by charcoal and the perceived harms of charcoal to heat tobacco (Lipkus et al., 2020). Many smokers were unaware that burning charcoal releases carbon monoxide, cancer-causing chemicals, and irritants to the lungs, eyes, and throat. They expressed little worry about inhaling these chemicals and perceived a low risk of developing smoking-related diseases if they continued to smoke shisha heated only with charcoal. These findings point to the need to educate smokers and the public about potential harms of using charcoal to heat waterpipe tobacco.
Conceptually, several models of health behavior change predict that heightened perceptions of risk should increase intentions to modify a maladaptive behavior; intention then predicts behavior change (see Sheeran et al., 2014 for review). Indeed, the literature supports this pattern (Sheeran et al., 2014). While increasing hookah smokers’ knowledge about the risks of using charcoal is a distal and often weaker factor in predicting intentions and especially behaviors (Fishbein & Ajzen, 2010), greater knowledge may increase risk appraisals for WTS (Lipkus et al., 2020). In turn, risk appraisals can dissuade smokers from using waterpipes or motivate the switch to safer alternatives. Thus, educational efforts should highlight content that enhances understanding of a risk more fully; including coverage of risk factors (i.e., use of charcoal), health consequences, and providing strategies to eliminate or reduce adverse consequences (Weinstein, 1999). An example of the latter, and the preferred educational approach, is to inform smokers that no safe charcoal products exist. Alternatively, rather than charcoal, smokers can turn to electrical heaters. However, there is mixed evidence on whether electrical heaters reduce toxicant content, exposing the user to some harmful chemicals found in combusted shisha (Brinkman et al., 2020a, 2020b; El Hourani et al., 2019).
Brief educational messages about the dangers of smoking hookah have been shown to increase perceived harms and desire to quit among young adults; however, these messages have not focused on the specific harms of charcoal (Lipkus et al., 2011; Mays et al., 2016). Accordingly, this prospective, online, randomized controlled study, in which the goal was to increase young adult hookah smokers’ perceptions of harms of hookah use with charcoal, examined whether that goal was achieved. Our educational approach used brief messages that emphasized risk factors (i.e., charcoal and its release of toxicants) and their health consequences, similar to the use of cigarette warning labels (Hammond, 2011).
Intervention arm participants received educational materials about harms of using charcoal in order to assess the effects on the amount and knowledge of toxicants, risk perceptions, and desire to quit WTS. Sustainability of short-term effects was reassessed one week after receipt of educational materials. We predicted that across time individuals who received the educational materials would view charcoal use as more harmful than those in the control arm. This hypothesis was tested using four dimensions of perceived harms: amount of toxicants released, safety of burning charcoal, worry about inhaling toxicants, and perceived risk of getting a smoking-related disease. We also predicted that participants who received educational materials would: 1) have greater knowledge of toxicants released by burning charcoal; 2) report higher perceived risk of tobacco-related diseases if they continued to smoke waterpipe; and 3) express a stronger desire to quit WTS than those in the control group.
Methods
Participants and Procedures
Participants were recruited using TurkPrime (TP, also known as CloudResearch) (Litman et al., 2017), a research platform that supports data collection using the Internet crowdsourcing platform Amazon Mechanical Turk (AMT) (Sheehan & Pittman, 2016). This data collection approach has been used in previous tobacco studies (Mays et al., 2016; Pearson et al., 2016; Shi et al., 2017), although samples are often not representative and findings may not generalize to the larger population (Litman & Robinson, 2020). The survey was first open to all Amazon Mechanical Turk workers who completed at least 100 online tasks, with 90% approval, an indicator that participants often provide more reliable responses. Informed consent was confirmed prior to screening for eligibility. Participants had to report being aged 18 years or older, engaged in WTS during the past 30 days, and had not “quit for good.”
Those who qualified were randomized with equal probability to a control or educational arm. Using the identification numbers TurkPrime provides, all participants were contacted a week later via email to reassess the main measures. Participants were paid $0.05 for completing a screener; eligible participants were paid $3.00 to their AMT account for completing the first part of the study (i.e., Time 1) and $1.50 for follow-up one week later (i.e., Time 2). The study was approved by the IRB at the Duke University Medical Center.
Data quality assurance steps, in addition to having at least 90% data reliability, included prohibiting duplicate responses and using verification to prevent automated completion. While completing the survey, participants were posed a single attention check measure whereby they had to give the answer instructed. The responses of individuals who deviated from the instructions did not differ significantly across the main measures compared to participants who responded as instructed; thus, all sampled data were used in the analyses.
Educational Materials on Harms of Charcoal
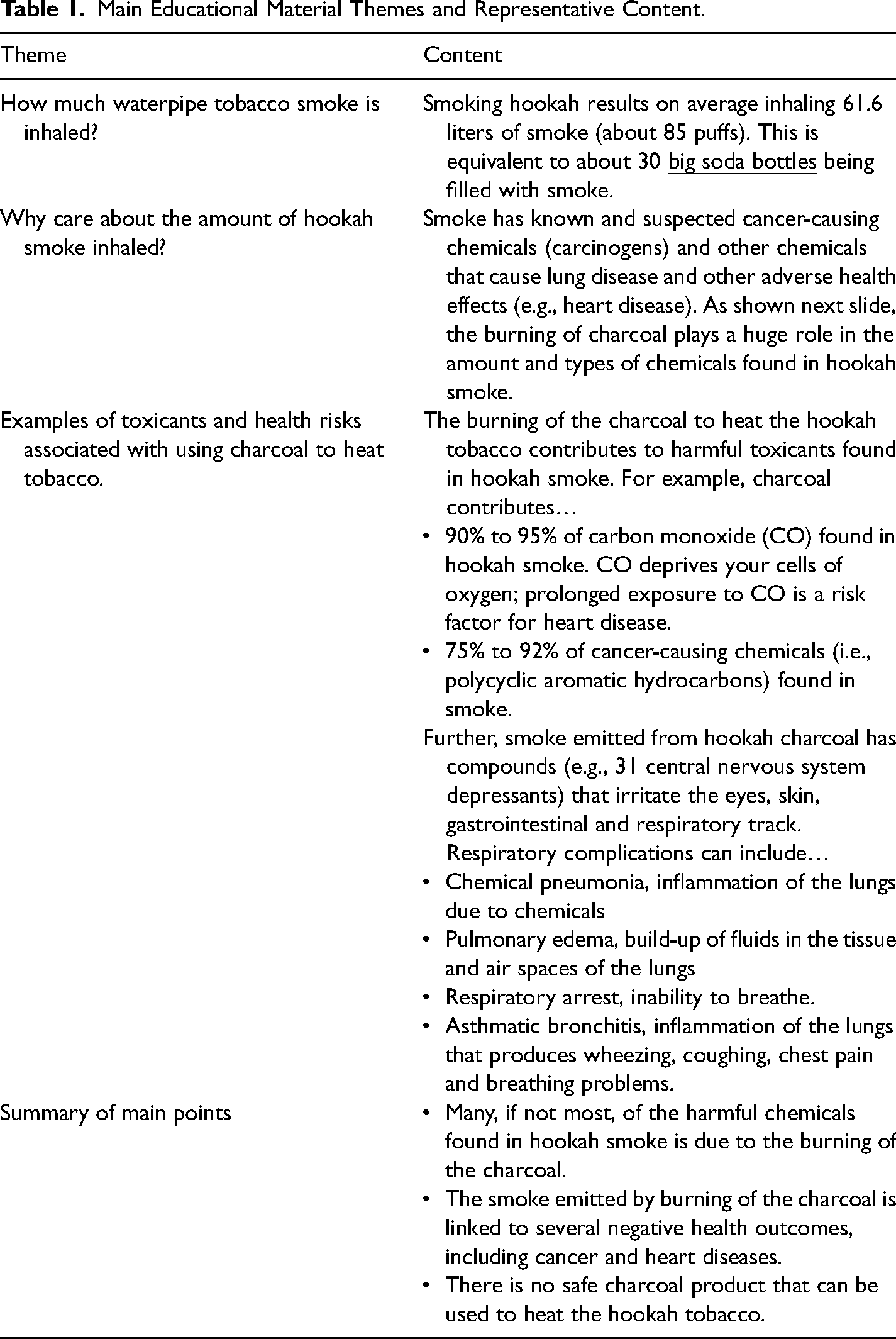
The harms of charcoal were presented via eight static descriptive text and slides entitled, “What you should know about the charcoal used to heat waterpipe (hookah) tobacco.” Participants clicked through the slides at their own pace. The main themes included: 1) how much smoke is released during a WTS session; 2) why knowing how much smoke is released matters; 3) examples of toxicants and their health effects associated with using charcoal to heat tobacco; 4) summary of key points; and 5) references (Table 1). The presentation included images of charcoal. While points 1 and 2 above were not about charcoal, they were necessary to help participants understand that the toxicants from charcoal are transmitted in large quantities through the smoke they inhale.
Main Educational Material Themes and Representative Content.
Control arm participants responded to self-report measures only. Participants in the control arm averaged 8.5 (SD = 4.2) minutes to complete the first survey while participants in the educational arm averaged 12.8 (SD = 5.7) minutes to complete the survey, spending an average of 2.3 (SD = 1.9) minutes reviewing the educational materials. The follow-up survey averaged 6.0 (SD = 5.1) minutes to complete. Participants in the educational arm reported putting a lot of effort into reviewing the educational materials (M = 6.10, SD = 1.21, from 1 = Very little to 7 = A lot).
Measures
Measures completed after randomization included demographics, other tobacco product use and WTS behavior, reactions to the educational materials (for educational arm participants), and main outcomes (i.e., knowledge, perceived risk and worry and desire to quit). The main outcomes were reassessed one week later.
Other Tobacco Product Use
Participants were asked whether they used: cigarettes, electronic cigarettes, large cigars, little cigars/cigarillos, regular pipe, electronic hookah, or none of the above in the previous 30 days.
WTS Smoking Behaviors
Participants were asked: 1) age of initiation of WTS; 2) typical smoking pattern (less than monthly to daily) and location of WTS; 3) whether they owned a waterpipe; 4) products they purchased; and 5) how often they prepared their own waterpipe.
Knowledge of Toxicants in Charcoal
Participants were asked whether burning charcoal to heat waterpipe tobacco released carbon monoxide, cancer-causing chemicals, as well as chemicals that irritate the lungs, eyes, and throat (Lipkus et al., 2020). Response options were “no,” “yes,” and “don‘t know.” A response of “yes” was deemed correct for each item.
To assess if the above questions were evaluating a unidimensional knowledge construct, we conducted an iterated principal factor analysis with promax rotation using a polychoric correlation matrix as input data from baseline. A single factor (MSA = .64) emerged that explained 80% of the variance (eigenvalue = 4.03) with item loadings ranging from .76 to.94. The five items were summed and averaged to create an average total correct knowledge score. Cronbach‘s alphas at baseline and at the one-week follow-up were.76 and.78 in the educational arm, respectively, and.80 and.75 in the control arm, respectively. The one-week test-retest for the five-item scale was.63 in the education arm and.72 in the control arm. The individual item one-week test-retest correlations ranged from.33 (irritates throat) to.60 (irritates eyes), respectively, in the experimental arm and.41 (irritates lungs) to.70 (cancer-causing chemicals), respectively, in the control arm.
Perceived Risk Appraisals
As per Lipkus and colleagues (2020), and employing their measures, four components were used to evaluate perceived risks of charcoal: the amount of harmful chemicals released, perceived safety of charcoal, perceived health risk, and worry about inhaling toxicants.
Perceived Amount of Harmful Chemicals Released
Participants were asked, “How many harmful chemicals are released by burning the charcoal to heat the waterpipe tobacco?” Response anchors were 1 = None to 7 = A great deal. The one-week test-retest was.60 in the educational arm and.56 in the control arm.
Perceived Safety of Charcoal
Participants were asked, “Would you say that the burning of the charcoal to heat the waterpipe tobacco is …” Response anchors were 1 = Very safe to 7 = Very harmful. The one-week test-retest was.71 in the educational arm and.49 in the control arm.
Perceived Health Risks and Worry
Perceived risk was captured by, “How likely is it that you will develop a serious smoking-related disease (e.g., heart disease, cancer) if you continue to smoke waterpipe that is heated only by charcoal?” Response options were: 1 = No chance, 2 = Very unlikely, 3 = Unlikely, 4 = Moderately likely, 5 = Likely, 6 = Very likely, and 7 = Certain to happen. The one-week test-retest was.74 in the educational arm and.71 in the control arm.
Worry about inhaling toxicants was assessed by, “How worried are you about inhaling harmful chemicals from burning of the charcoal when you smoke waterpipe tobacco?” Response options were: 1 = Not at all worried, 2 = Slightly worried, 3 = Somewhat worried, 4 = Very worried, and 5 = Extremely worried. The one-week test-retest was.66 in the educational arm and.62 in the control arm.
To assess if the above questions were assessing a unidimensional risk appraisal construct, baseline data were used to conduct an iterated principal factor analysis with promax rotation. A single factor emerged (MSA = .78) that explained 74% of the variance (eigenvalue = 2.95) with item loadings ranging from.76 to.86. The four items were summed and averaged to create a mean risk appraisal score. Cronbach‘s alphas at baseline and at the one-week follow-up were.83 and.86 in the educational arm, respectively, and.83 and.88 in the control arm, respectively. The one-week test-retest was.80 in the educational arm and.68 in the control arm.
Perceived Absolute Risk
As a global measure, participants were asked, “What do you think is your chance of getting a serious smoking-related disease in your lifetime, such as cancer, lung disease, or heart disease if you did not quit waterpipe tobacco smoking?” Response options were 1 = No chance, 2 = Very unlikely, 3 = Unlikely, 4 = Moderately likely, 5 = Likely, 6 = Very likely, and 7 = Certain to happen. The one-week test-retest was.80 in the educational arm and.68 in the control arm.
Desire to Quit
This was captured by, “How strong is your desire to quit waterpipe tobacco smoking right now?” Response anchors were 1 = Not at all strong to 7 = Very strong. The one-week test-retest was.70 in the educational arm and.36 in the control arm.
Statistical Methods
Descriptive statistics were used to summarize participants’ demographics and WTS behavior. Chi-square or t-tests of these measures were conducted by study arm to confirm baseline balancing via randomization. Knowledge of toxicants in charcoal is presented as frequency and percentage of correct responses (i.e., answer of yes) as well as means scores of correct responses. To test the effects of study arm across time, generalized estimating equations (GEE) were used specifying the binary outcome, correct vs. incorrect knowledge of toxicants in charcoal using SAS 9.4 GENMOD procedure; odds ratios are presented predicting odds of being correct comparing the educational to the control arm. To assess mean differences in individual risk appraisal items and total score, perceived absolute risk, and desire to quit by study arm across time, generalized linear models were run using SAS 9.4 Proc Mixed with compound symmetry as the covariance structure and REML as the estimation method. Means and standard errors are presented for both predicted and observed values; because predicted and observed values were similar, results are interpreted using predicted scores. All arm-by-time by time interactions for predicted scores were followed by tests of simple effects comparing effects between arms at Time 1 and 2 (follow-up).
The main pattern of results due to arm did not vary substantially by demographic or WTS characteristics; thus, we report effects by arm across time without adjustment for these variables. Due to the number of statistical tests performed, an alpha of.01, two-tailed, was deemed statistically significant.
Results
Sample Characteristics
Overall, 435 individuals completed the online screener and survey, of which 203 were eligible and randomized (104 educational arm; 99 to the control arm). Of these, 85 in the educational and 79 in the control arm completed the one-week follow-up (i.e., Time 2). Little‘s test for missingness at random revealed that the demographic and main outcomes data were missing at random. Table 2 presents demographic and WTS characteristics for the entire sample and by study arm. Participants were in their early 30s, with slightly more men than women, mostly white, with roughly equal proportions of some college or college graduates. The samples were comprised mostly of non-students. Most were employed full-time.
Sample Demographics, Waterpipe Tobacco Smoking Characteristics, and Other Tobacco Product Use.
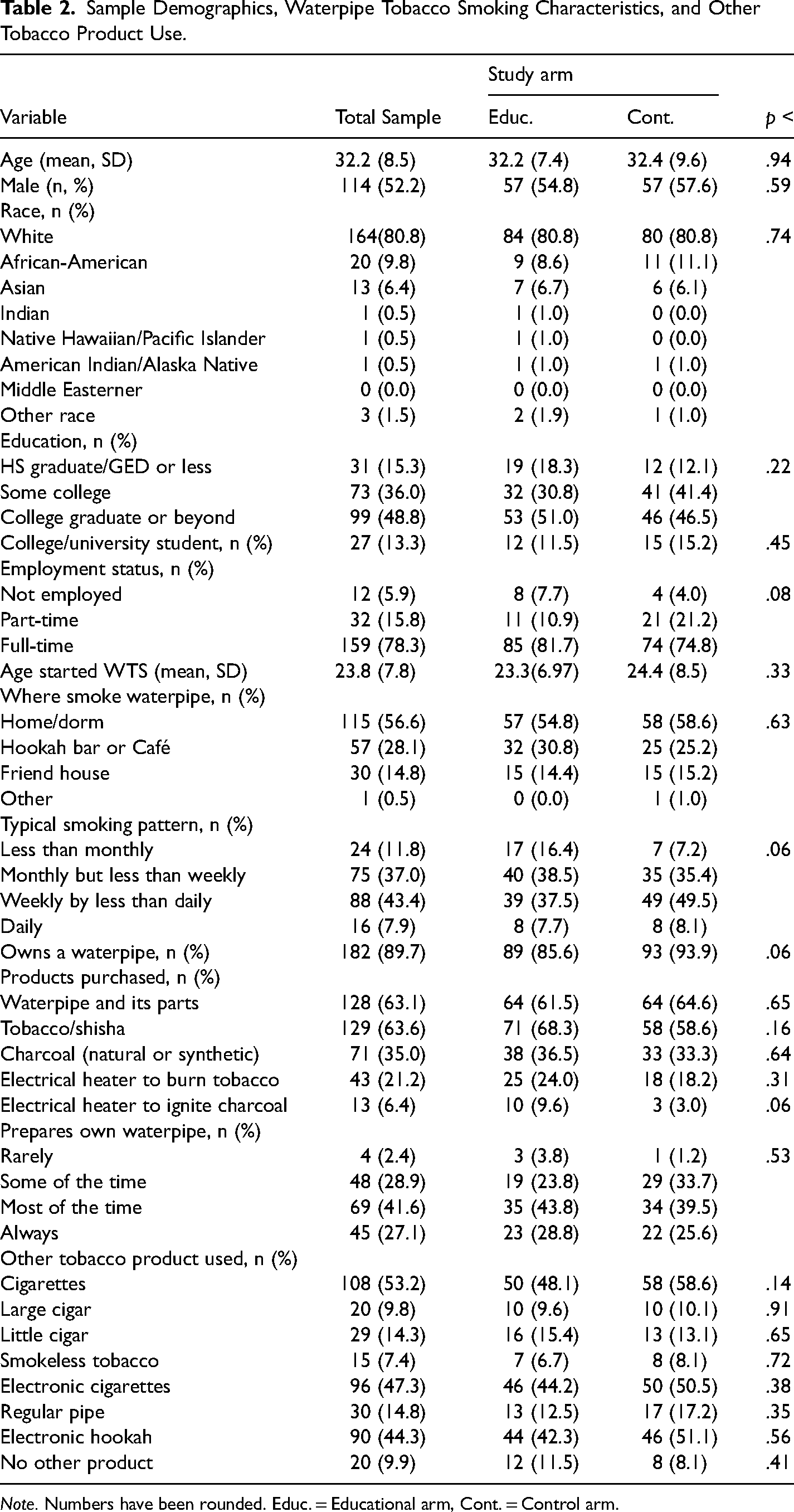
Note. Numbers have been rounded. Educ. = Educational arm, Cont. = Control arm.
In terms of WTS characteristics, the average age of initiating WTS was in the early 20s. The most common place to smoke waterpipe was at home/dorm. Most either smoked waterpipe monthly but less than weekly (37%) or weekly but not daily (43%). Nearly 90% owned a waterpipe. Overall, 21% of participants reported purchasing an electrical heater to burn their waterpipe tobacco—main outcomes did not vary by this variable. A large proportion of participants prepared their own waterpipe at least some of the time to always (85% of the sample). Cigarettes, electronic cigarettes, and electronic hookahs were the most prevalent other tobacco products used.
Knowledge of Toxicants
We predicted educational arm participants would be more likely than control arm participants to report correctly that burning charcoal releases carbon monoxide, cancer-causing chemicals, and throat, lung, and eye irritants. These predictions were supported by a significant main effect of arm for all outcomes (See Table 3). Across time, except for CO, which had an arm-by-time interaction, participants in the educational arm correctly identified more toxicants released than participants in the control arm. For example, participants in the education arm were 8.57 times more likely to state that smoking waterpipe tobacco releases cancer-causing chemicals compared to participants in the control arm across time (95% CI = 4.34–16.91). For CO, whereas the percentage of participants in the educational arm who correctly acknowledged this chemical is released did not differ across time, the percentage of participants in the control arm with a correct response increased significantly across time (42% to 86%. p < .0001).
Correct Knowledge of Chemicals Released by Burning of Charcoal by Time and Study arm.

Note. Numbers represent how many and the percent of participants who answered correctly. The odds ratio represents the odds of being correct comparing the educational versus the control arm. The three p-values from top to bottom represent the main effect for arm across time, main effect for time and the arm-by-time interaction. Numbers with different subscripts differ at p < .05 for tests of simple effects decomposing significant interactions. Values of p < .01 and smaller were considered statistically significant. Time 1 = time of assessment, Time 2 = 1-week follow-up. Educ. = Educational arm, Cont. = Control arm.
Total mean knowledge varied as a function of arm, time and an arm by time interaction (bottom of Table 3). The nature of this interaction was such that mean correct knowledge was significantly higher in the educational than the control arm across time with no significant difference in mean scores across time in the educational arm. However, in the control arm, mean correct knowledge was significantly higher at Time 2 than at Time 1.
Perceived Harm
Four outcomes were used to assess perceived harms from charcoal: perceived safety of burning charcoal, amount of toxicants released, perceived risk of getting a smoking-related disease if the person continued to smoke using charcoal only, and worry about inhaling toxicants related to burning charcoal. We expected participants in the educational arm would report greater perceived harms across items than participants in the control arm (see Table 4).
Perceptions of Waterpipe Tobacco Smoking Harms and Desire to Quit by Time and Study Arm.

Note. Mean (SE) presented for all outcomes. Higher means represent greater perceived risk or desire to quit. The three p-values from top to bottom represent the main effect for arm across time, main effect for time, and the arm-by-time interaction. Predicted means with different lettered subscripts differ at p < .05 for tests of simple effects decomposing significant interactions. Time 1 = time of assessment, Time 2 = 1-week follow-up. Educ. = Educational arm, Cont. = Control arm.
Predictions were supported for all outcomes with significant main effects of arm, indicating that participants in the experimental arm reported higher perceptions of harm across time than participants in the control arm. These main effects were qualified by arm-by-time interactions for two outcomes: perceived safety of burning the charcoal to heat the tobacco and the perceived number of harmful chemicals released by burning the charcoal to heat the tobacco. Tests of simple effects revealed that among participants in the experimental arm, the predicted means for these two outcomes remained stable and higher than the means in the control arm across time; however, among participants in the control arm, the predicted means for the two outcomes increased significantly at Time 2 relative to Time 1.
Total mean risk appraisals varied as a function of arm, time, and an arm-by-time interaction (row five, Table 4). The nature of this interaction was such that mean risk appraisals were significantly higher in the educational arm than in the control arm across time, with no significant difference in mean scores across time in the educational arm. However, in the control arm, average risk appraisal was significantly higher at Time 2 than at Time 1; yet the mean in the control arm at Time 2 was lower than the mean scores in the educational arm across both time points.
Perceived Risk of Continuing to Smoke
We expected that reviewing the educational materials about charcoal would generalize to a perceived higher personal risk of developing smoking-related diseases should one continue to smoke waterpipe. As predicted, participants in the educational arm reported higher perceived risk for smoking-related disease than participants in the control arm across time (see Table 4).
Desire to Quit
We predicted and found that desire to quit WTS would be stronger among participants who viewed the educational materials versus those who did not (see Table 4). This main effect of arm was qualified by main effect of time and arm-by-time interaction. Tests of simple effects revealed that while the mean desire to quit did not change significantly between time points among participants in the educational arm, in the control arm participants’ desire to quit increased from Time 1 to Time 2.
Discussion
Toxicants released by burning charcoal to heat waterpipe tobacco are plausible causes for the negative health outcomes associated with WTS (Akl et al., 2010). Studies using smoking machines and actual smokers reveal that WTS using charcoal releases several toxicants (Brinkman et al., 2020a; Monzer et al., 2008). While only a few studies have explored the magnitude and types of toxicants released by burning charcoal, the extant literature supports informing individuals of the harms of charcoal used to the tobacco. To the best of our knowledge, no interventions exist containing detailed information about the harms of charcoal and assessed their effects on perceived harms, knowledge of toxicants, and desire to quit. To the authors’ knowledge, this study is the first to report these effects.
Compared to participants who did not view the educational materials, those who did judged charcoal as more harmful overall based on several dimensions, including viewing charcoal as less safe, releasing more rather than fewer harmful chemicals, increasing worry about inhaling toxicants, perceiving oneself at greater risk for WTS-related diseases contingent on using charcoal exclusively, and having greater knowledge of toxicants released. Further, participants in the educational compared to the control arm expressed greater perceived personal risk if they continued to engage in WTS; thus, the intervention influenced one global measure of perceived harm.
Despite promising effects, findings point to potential limitations of brief educational messaging. For example, the mean for worry about inhaling toxicants was around the midpoint of the 7-point scale. If emotional reactions are key drivers to behavior change, and more so than cognitions, then our messages may not be potent enough to reduce WTS or change heating source use. Perhaps a more effective way to evoke thoughts about harm is to post health warnings about charcoal on waterpipe equipment and product ads (Islam et al., 2016). Further, a consistent result across measures was that participants in the control arm reported greater knowledge and higher total average risk appraisals at follow-up while participants in the educational arm reported no or small declines—producing arm-by-time interactions. The reasons for this pattern are unclear. Study involvement may have influenced participants to think more about their WTS and seek information about the harms of heating sources, especially among those in the control arm. Another possibility is that randomization did not work completely, such that participants in the control arm started with poorer knowledge and lower perceptions of harm than participants in the educational arm, producing a potential regression toward the mean effect. Despite these observations, with exception of knowledge of CO being released, mean scores on most measures remained highly stable in the educational arm and significantly higher than in the control arm across time. Future designs should assess baseline levels of knowledge and perceived harms and then randomize participants to study arms.
Our findings provide insights to improve the public‘s understanding of WTS health risks in several ways. First, based on these promising preliminary findings, public health messages could incorporate more information regarding the harms of using charcoal to heat waterpipe tobacco and ultimately examine messaging effects on waterpipe use behaviors. While waterpipe smokers acknowledge that WTS is harmful to some degree, many may not realize that a major source of toxicants stems from burning charcoal; data on this perception of WTS are almost nonexistent. It is likely that smokers attribute most toxicants originating from chemicals in the tobacco contrary to available evidence (Elsayed et al., 2016; Monzer et al., 2008). For example, Monzer and colleagues using a waterpipe smoking machine found that about 90% of the CO and 75–92% of PAH compounds found in waterpipe tobacco smoke came from the charcoal (Monzer et al., 2008). Second, from a policy perspective, a major mission of health agencies, such as the Food and Drug Administration, is to create and disseminate educational materials to the public to assist in making informed decisions about tobacco use. The content of our materials can be used for this purpose alone or integrated with other educational materials on WTS. Third, and more broadly, the content presented may be used as part of an intervention effort for WTS as a harm reduction strategy (e.g., reduced frequency of use, use of lower harm waterpipe materials/tobacco products) and/or to encourage quitting more generally. A harm reduction strategy may be well received among smokers who do not or cannot quit WTS. Use of the current materials will require further testing to determine if messaging on the harms of charcoal translates into behavior change, but our results represent preliminary support for their utility.
Study limitations
There are several methodological limitations, beginning with caveats regarding using AMT samples. Findings based on AMT workers are not well-suited for descriptive research aimed at making broader claims about the US population because these samples are often not representative of the population (e.g., people are younger, more educated, etc., Goodman et al., 2013; Litman & Robinson, 2020) and are limited to those who have access to phones, computers, and an AMT account. Consequently, it is unclear if our findings generalize to a representative population sample of waterpipe tobacco smokers and among those who do not respond to online surveys for payment. However, samples based on AMT workers provide useful insights pertaining to correlational and experimental studies that mirror effects found in other more (representative) samples (e.g., see the Fit-for-Purpose Framework, Litman & Robinson, 2020). For example, in the tobacco control arena, Jeong and colleagues conducted phone interviews using probability samples and online surveys with AMT samples that had embedded experiments (Jeong et al., 2019). They found that many of the experimental results and associations were similar in both samples (see also Kraemer et al., 2017). Another concern is that data based on AMT samples are biased and unreliable. AMT workers maximize their income—with low payment in many cases—by completing online studies quickly; as a result, workers may not attend fully or expend effort on survey tasks. In-depth explorations have revealed that biases and poorer quality data stem, in part, from bots and participants from other countries (e.g., due to language barriers) taking surveys meant for US participants (Hauser et al., 2021). When country of origin is controlled for (e.g., by screening and/or verification of IP addresses) as well as when data quality control strategies are used (e.g., attention checks), data from AMT workers can be highly reliable (Goodman et al., 2013; Hauser et al., 2019, 2021; Kennedy et al., 2020). We implemented some of those quality control strategies but, given the potential limitations of using AMT samples, validity and generalizability of findings need to be tempered until results are replicated in other samples.
Other limitations pertain to content and model of dissemination. Our content was delivered via static text and images, which are less captivating than videos and/or more highly engaging public service announcements. What matters is that the content described may transfer readily to more engaging social and other media outlets. To this end, we included brief general content (e.g., amount of smoke) not specific to charcoal use. A credible argument can be said that doing so confounds effects due to the general versus charcoal-specific information. While not completely resolving this issue, our questions were conditional on asking about charcoal. Third, the follow-up assessment was very short, limiting re-testing of the messaging effects on our outcomes and importantly on WTS and use of charcoal. Longer follow-up periods should be implemented. Fourth, participants were exposed only once to the educational intervention. Testing the effects of repeated exposures holds the key to producing more profound and lasting effects; this strategy should be pursued.
Conclusion
Overall, this study is novel and represents a first step in testing messaging effects, albeit in a non-representative sample, on the use of charcoal as a heating source for WTS. This is an area that needs more research testing messaging effects. The educational content increased knowledge of toxicants and perceptions of harm, and increased the desire to quit. Future research should attempt to replicate and extend findings using representative samples of adult waterpipe smokers, and test the effects of repeating messaging that can be integrated into interactive and engaging media and/or on waterpipe tobacco products and ads on WTS heating source use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the Duke University School of Nursing.