
Abstract
Patient safety narratives are a globally mandated format for representing individual patient experiences, and they include peer-reviewed case reports and narrative medicine. The authors show how the humanistic values described by Carolyn Miller in 1979 could enhance or contribute to international health and medical communication in relation to such narratives. They do so by expanding on twenty-first century work by Bowdon and Scott to provide a framework for considering how narrative competence and narrative humility may allow technical communicators to strengthen their practices within technical communication and the rhetorics of health and science by examining an individual problem within its broader, intercultural contexts.
Introduction
The U.S. Food and Drug Administration (U.S. FDA) and other health authorities, like the European Medicines Agency and the Japanese Medicines Agency, seek to better account for individual patients in drug development so they may better understand the effects of medicinal products. Most such efforts center on clinical trials, which are inherently internationally important studies that follow common standards to provide globally applicable data (ICH E6, 2016). Such studies represent a rich, vital source of information on how different national agencies collect health and medical information that can benefit technical communicators working in international health contexts.
Within clinical trials, individual patient safety narratives account for the most dangerous adverse events: deaths, near deaths, and hospitalizations. These narratives, by design, combine information from multiple required tables and lists to better inform risk assessments and regulatory decision-making (ICH E3, 1995; ICH E6, 2016). Patient safety narratives reside at an interesting intersection between individual experiences of medicine and a dehumanizing function of textual automation in study contexts. Of interest for technical communication scholars, patient safety narratives represent standardized practices for conveying information in intercultural medical contexts. Regulatory bodies in many different countries receive and review such narratives in the course of clinical trials and reports of their results.
As clinical studies collect information from individuals in different cultures, study data and the guidelines for writing about them can help illuminate cultural perceptions of medical conditions, processes, and contexts. Thus, patient safety narratives are a possible site for interrogating the nature of regulatory writing, an underexamined intercultural discourse in technical communication. This entry examines how patient safety narratives operate within the context of regulatory documentation in contrast with patient case reports, which appear in the medical literature. Analysis of these forms by technical communicators may create opportunities for intervention in international health and medical settings and situations.
Contextualizing Clinical Trials
Clinical trials assess medicinal products, like drugs or medical devices, in human subjects. The overall objective of clinical trials is to ensure that public health is protected and that needed medicinal products are available to treat and prevent illness. These trials comprise several broad types. For example, Phase 1 clinical trials include small numbers of people and assess pharmacological effects such as how long a product remains in the blood stream. Larger Phase 2 studies identify whether products have the potential to impart benefits and to determine optimal doses for Phase 3 studies. These Phase 3 studies provide supportive evidence that the product works as intended in a larger group of patients.
Before any clinical trial can be conducted, manufacturers apply for permission and must provide adequate substantial supportive data from laboratory and animal studies (Phase 1). Once an optimal dosing regimen is identified at the end of Phase 2, further permission is necessary to progress into Phase 3 studies. After a product is approved for marketing, additional studies may be required. Every stage from the study design to data analysis must be documented. Such documentation itself is regulated and must be reviewed, and the review itself also should be documented.
Furthermore, regulatory agencies have been attempting to include more information about patient experiences in the design, conduct, evaluation, and communication of clinical trials and their results. Table 1 details efforts at the U.S. FDA and provides an overview of goals connected to specific actions. Of note, these processes center on the ability to bring patient voices into study design, conduct, evaluation, and reporting, and also to create greater transparency relating to such activities. It is further worthy of note that these efforts parallel both attempts to maximize patient perspectives in document design as noted by Lisa Melonçon (2017) and Kirk St.Amant (2017) and practices across many cultural contexts (ICH E6, 2016).
Efforts to Include Patient Perspectives at the U.S. Food and Drug Administration Center for Drug Evaluation and Research Under the Prescription Drug User Fee Act.

Note. Reproduced and adapted from U.S. FDA (2018).
One document central to clinical trials is the clinical study report (ICH E3, 1995). The clinical study report details study conduct and results, generally in data-dense displays of tables and figures that present information about patients by group (e.g., all people who received a certain dose of a specific product). Few sections of the clinical study report account for the possible effects of a product on individual people; the most substantive of these is the patient safety narrative, which provides a brief, structured account of each event of note (see Table 2). These narratives are based on data collected during the study as well as specific documentation obtained after the event. As such, they represent an important source of information about how documentation formats have been systematically constructed to function across cultural boundaries.
Patient Safety Narratives for Clinical Study Reports Mandated in International Guidance Documents.
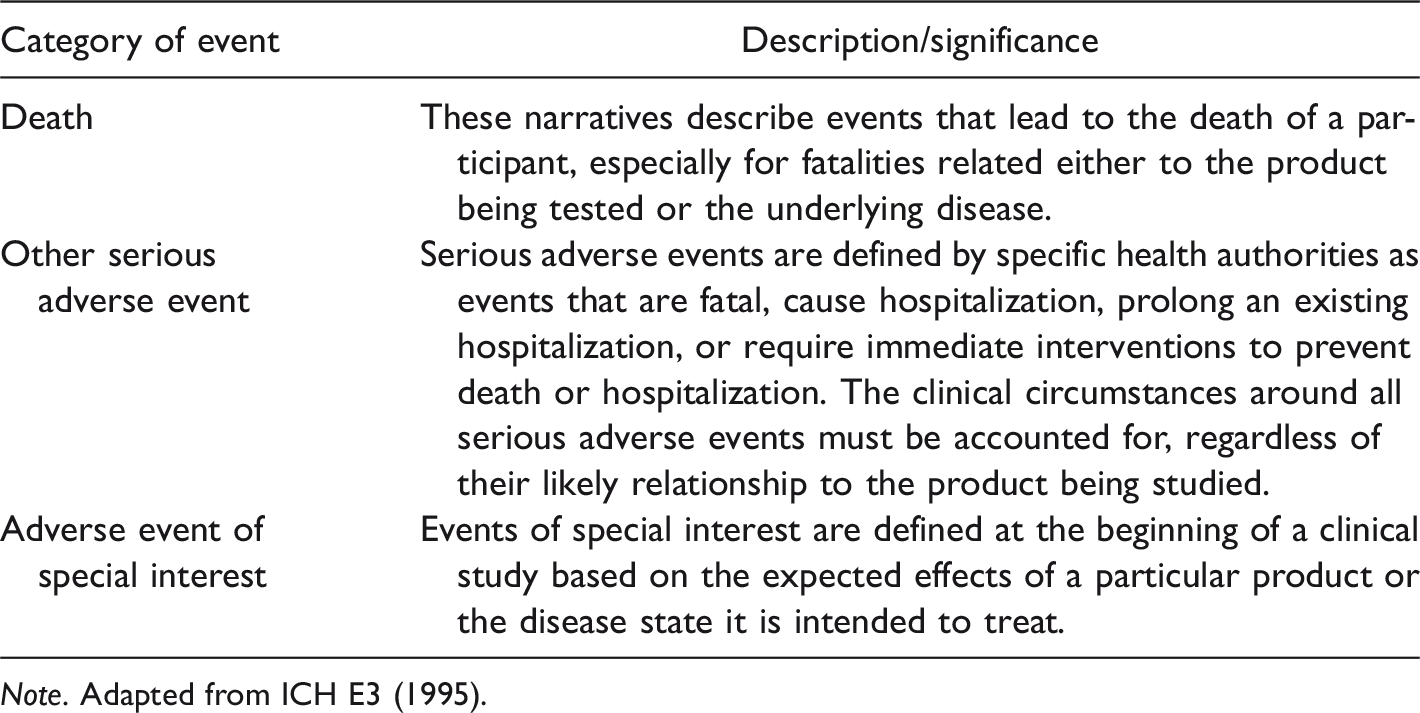
Note. Adapted from ICH E3 (1995).
From the technical communication standpoint, patient safety narratives are interesting because they provide a framework for understanding at least some individual experiences within multinational clinical studies. This information can help guide the creation of patient-centered materials that meet the perceptions and expectations of individuals from a given culture. The more technical communicators understand these narratives, the better they can use them as a resource for creating effective health and medical materials for patients in a given culture.
Connecting to Technical Communication
In medical contexts, understanding and addressing the needs and expectations of patients can be a central challenge to creating usable, effective materials. By bridging normative perspectives and complex information, technical communicators can address conceptual gaps in existing materials to meet patient needs. For example, technical communicators producing infographics about particular products may use information from clinical studies as a basis for their work. Furthermore, technical communicators who study user experiences may offer valuable insights about clinical trial data, enhancing patient decision-making, and communicating trial results. Thus, the efforts described in Table 1 may be of interest to technical communicators as an information source for work such as building patient portals on websites and also a possible site for intervention and interpretation.
Leveraging information from regulatory documentation could enable interventions into intercultural communication challenges noted by Ding (2014) and Sun (2012). Ding cites translational difficulties between languages and cultural expectations in communication about dangerous health outbreaks affecting multiple countries. Sun considers how intercultural content can be adapted to serve users in a specific location. Such practices would also align with patient experience design (PXD) as proposed by Melonçon (2017). Layering intercultural concerns onto PXD provides further opportunities for constructive intervention and could foster usability practices in international health communication contexts, which St.Amant (2017) terms international PXD (I-PXD).
Most regulatory documentation follows globally acceptable documentation guidelines, which represent an important intercultural discourse that technical communicators can use to understand medical information intended to cover local concerns (ICH, 2018; Benau, 2017; Wood & Foote, 2008). A deeper understanding of regulatory documentation as health-related information can enrich technical communicators’ adaptations of complex concepts for general use. Such understanding could contribute to improved PXD practices that (per Melonçon, 2017) mirror patient experiences during the design process and extend into I-PXD contexts (per St.Amant, 2017). The key to making such connections is seeing how technical communicators can use patient narratives and related documentation to realize such aspects of PXD and I-PXD.
Relatively little work in rhetoric or technical communication addresses regulatory documentation. A notable exception is Cuppan and Bernhardt’s (2012) analysis of study report authoring and review. Their entry draws on their critiques of the writing and argument quality in these reports and suggestions for better documentation processes. In a related setting, Graham, Kessler, Kim, Ahn, and Card (2018) observed that efforts to expand patient participation in FDA expert advisory boards ironically often “further marginalize” their opinions (p. 59). These observations highlight the essential function of expert discourses. For example, advisory boards, by design, augment FDA knowledge (Advisory Comitteee, 2018), just as clinical study reports and patient safety narratives serve an expert readership to prevent the approval of dangerous products. Technical communication thus may help patients and other end users understand complex, expert language that addresses broadly intercultural audiences by developing documents that meet specific cultural needs and expectations, per Sun (2012). While few technical communicators will engage in regulatory writing, all technical health-care communication might use a reading knowledge of regulatory materials in its work.
When considering the examples in Table 1, technical communicators may use their existing skills to evaluate patient participation in expert panels, interpret advertising, and assess usability. Intercultural technical communicators can address problems in patient-centered communication and contextualize discussions grounded in a single cultural setting against intercultural discourses or vice versa. Hence, an aim of this entry is to provide information about the context of information collected in regulated intercultural health-care settings for use by technical communicators. Enhancing the ability of technical communicators to understand and situate highly complex and inflected biomedical discourse, like patient safety narratives, against other narrative forms will enable them to better address patient needs in public-facing documents. This entry provides a model for interpreting and using patient narratives as a model for critical engagement with regulatory discourses.
Approaching Patient Narratives
This entry frames patient safety narratives for a technical communication audience. To do so, it follows the types of intellectual values described by Carolyn Miller (1979) in her account of technical communication as a humanistic discipline. One reason for this choice is that the existing framework of regulatory documentation represents such communication as grounded in scientific practices. The current entry then places regulatory documentation in the context of other medical narratives to help technical communicators understand regulatory documentation and identify sites of possible interpretation or intervention. These narrative types should interest scholars whose work addresses the intersections of rhetoric, culture, and language because together these genres reveal that the term narrative itself carries many different meanings, creating a space for technical communication work.
Technical communication can make interventions at multiple sites in communicating information collected in clinical trials of which patient safety narratives are a particularly interesting phenomenon. A core function of technical communication, as defined by groups such as the Society for Technical Communication (stc.org) or tekom (technical-communication.org), is to explain complex information for end users, including the general public. These goals, much like regulatory documentation itself, are international and intercultural because such activities necessarily cross cultural boundaries as they impact external actor and organizational views of the field (St.Amant, 2016). Thus, technical communicators are well positioned to contribute to and benefit from an understanding of regulatory practices. The global character of these practices represents a major area in which technical communicators could enhance or contribute to international health and medical communication.
To participate in such activities, technical communicators need mechanisms for enhancing their understanding. A humanistic approach to such contexts can help achieve this objective. In the next sections of this entry, we examine how technical communicators can use such an approach to achieve this objective. To do so, we pair humanistic conceptions of technical writing (Bowdon & Scott, 2003; Miller, 1979) with medical models of narrative medicine (Charon, 2001; Das Gupta, 2008) that seek to value patient experiences in the clinic. We then present an invention framework of intercultural questions applicable to patient safety narratives and additional regulatory and medical documentation.
Defining Regulatory Patient Safety Narratives
Understanding patient safety narratives entails recognizing their function in enabling (Benau, 2017; DeTora, 2017; Hamilton, 2014; Wood & Foote, 2008) government agencies to justify medical research or product marketing. If a goal of medical regulation is to protect individual lives and public health, patient safety narratives might be understood as describing possible failures in this goal. Regulatory documents follow strict rules of formatting and content placement to facilitate review and decision-making (Benau, 2017; Hamilton, 2014). The end user must locate relevant information quickly, an endeavor that until the late 20th century required negotiation of myriad language and cultural contexts (ICH, 2018; Benau, 2017; Wood & Foote, 2008).
Late 20th century attempts to reduce the regulatory documentation burdens for authors and evaluators may also be seen as enhancing intercultural communication by creating predictable document structures. However, consistent document frameworks also effectively erased many country-specific forms and now face the local challenges Sun (2012) discusses. As regulatory documentation relies on shared formats and worldwide use of the English language, with local language translations needed only for a few key documents (ICH, 2018), many regulatory documents serve multiple intercultural needs.
International agreements for documentation formats were reached during the late 20th century by the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH, 2018). Originally, the ICH represented a collaboration between health authorities and industry sponsors in the United States, Japan, and Europe, with additional observer nations; today these guidelines are used across the world. The ICH E3 Guideline for the Structure and Format of Clinical Study Reports (1995) provides a specific organization for describing the conduct and outcomes of clinical trials, which must also follow the ICH (E6) Good Clinical Practice (2016) guideline (Benau, 2017). Both ICH E6 and E3 mandate the use of consistently formatted patient safety narratives (see Box 1) to describe serious adverse events and other events of special interest, which were briefly defined in Table 2. Patient Safety Narrative Contents (ICH E3, 1995).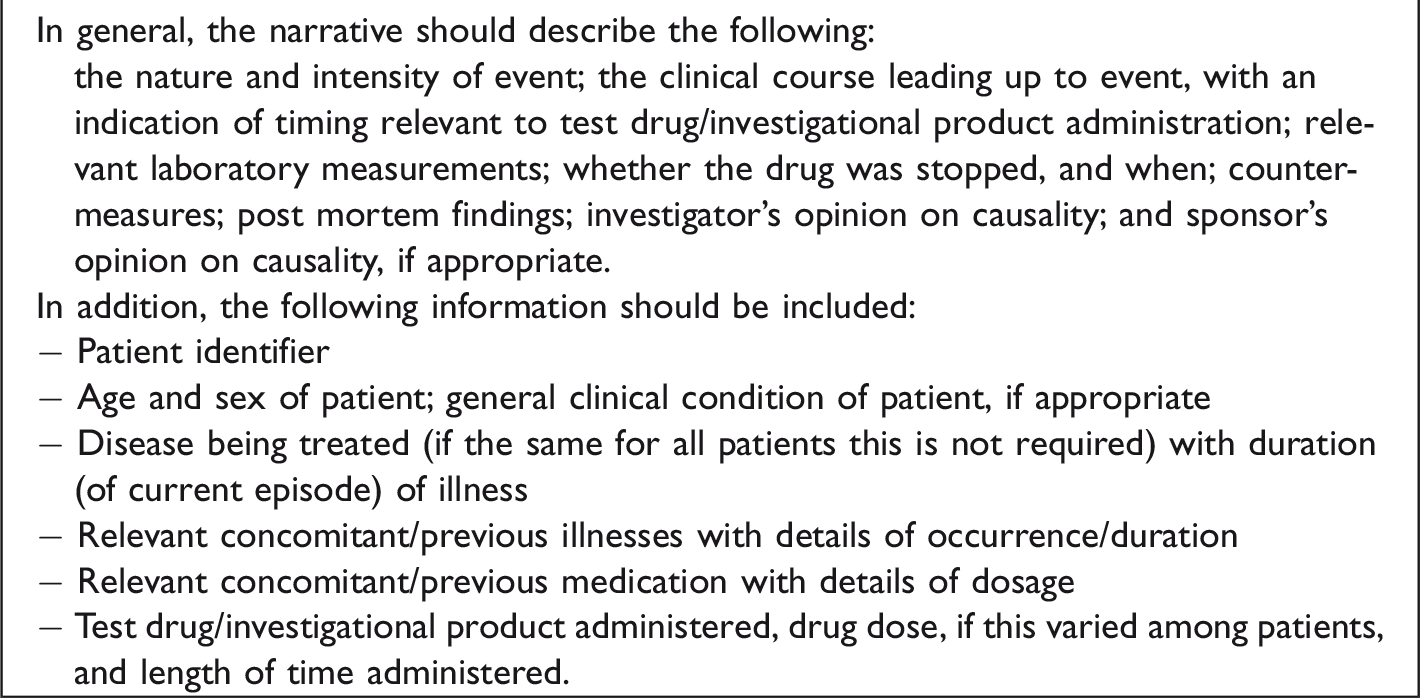
Generally, patient safety narratives are required for events that pose a serious danger for a person enrolled in the trial or that signal inherent problems in the product being investigated. Patient safety narratives must follow ICH guidelines and any needed individual cultural or national requirements that would enable regulators to evaluate safety concerns, risks, and benefits of products under evaluation (ICH E3, 1995; ICH E6, 2016). Ideally, patient safety narratives help regulators clearly identify whether a product should or should not be approved for marketing. Given the common use of documentation across national boundaries, such documents are often prepared to meet all audiences, serving as an inherently intercultural form.
As the content in Table 2 indicates, patient safety narratives describe rare experiences in clinical trials—death, serious illness, and events of specific concern—and provide little to no subjective experience. Hamilton (2014) identifies two categories of patient safety narratives:
Pharmacovigilance narratives provided during the study for health authorities in each country in which a study occurs (thus requiring translation) Final narratives in reports prepared after the study is completed
The information in individual patient safety narratives can stop ongoing studies or prompt health authorities to remove products from the market (Hamilton, 2014; ICH E6, 2016; Moons, 2015). Thus, patient safety narratives can be seen in relation to the efforts to include patient-level experiences noted in Table 1. A key consideration, however, is that patient safety narratives comprise information reported about rather than by the patient (Moons, 2015).
The patient safety narrative structure shown in Box 1 presents information in a proscribed order to ease interpretation, translation, and reading by audiences presumed to be managing multiple languages. Readers must quickly identify whether an intervention is needed to protect patients, which is a crucial decision, especially for products already in wide use. Given the broadly intercultural impact of narrative genre on world health care, it is worthy of further examination and contextualization. In the next section, we offer a technical communication framework for making sense of patient safety narratives against related discourses.
Technical Communication as Humanizing Discourse
Technical communication, as conceived by Miller (1979), emphasizes intellectual and pedagogical grounding in “a communal rationality rather than in contextless logic” (p. 617). Hence, it emphasizes a contrast with specialist documentation guidelines fostered by groups like the ICH, which parallel the work of Elizabeth Tebeaux (2017), who argued that technical communication was grounded in scientific inquiry. A bridging viewpoint might be seen in Charles Bazerman’s (1987) observation that structured scientific discourses leave readers to glean information from disparate texts. Given the importance of structured sources for health-care communication, an appreciation of its target audiences and creators is valuable.
Fortunately, Bowdon and Scott (2003) provide a vital instructional framework for considering rhetorical situations (Table 3). They encourage instructors, students, and practitioners to consider the role and aims of writers, audience needs, and textual genres and functions as necessarily interrelated. Thus, Bowdon and Scott frame human contexts for communication to provide an adaptable means of uncovering communal rationality.
Invention Questions for Technical Communication.
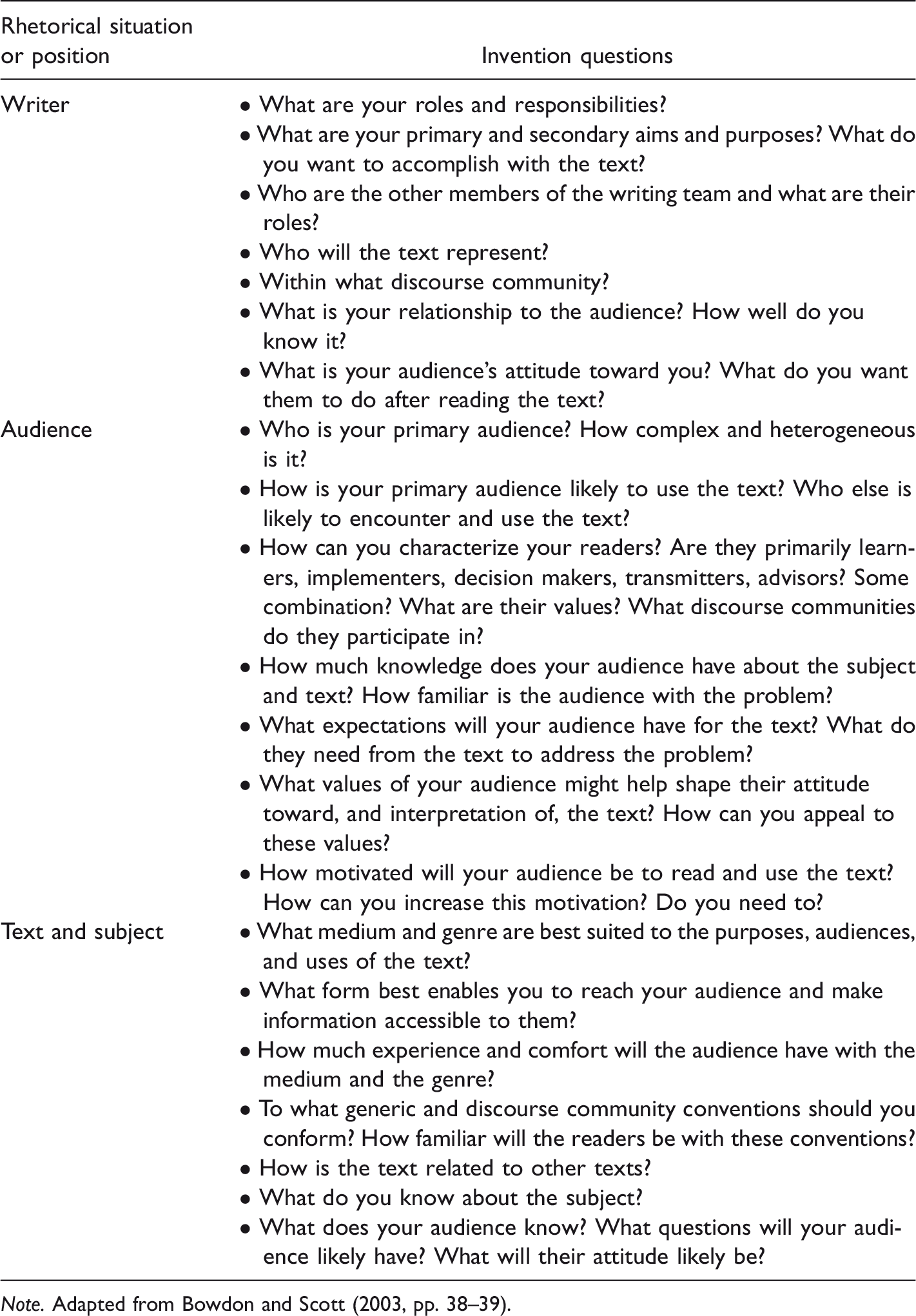
Note. Adapted from Bowdon and Scott (2003, pp. 38–39).
By choosing appropriate invention questions (see Table 3), any rhetorical actor can more effectively engage with textual production and audience needs, regardless of the source discipline. For example, this framework might be applied to FDA efforts to include patient perspectives (see Table 1), study reports, or patient safety narratives. More importantly, Bowdon and Scott identify contextual spheres of production, distribution, and reception of texts (see Box 2). Critical to this work is the necessity to respect the exigencies and goals of the rhetorical situation (Box 2) and to find means of accommodating them by using the framework for the appropriate audience or situation described in Table 3. Invention Questions About Contextual Spheres of Production, Distribution, and Reception. Note. Adapted from Bowdon and Scott (2003, p. 39).
In applying these ideas, technical communicators can more effectively evaluate and enter into user and audience concerns. In practical terms, technical communicators can use the questions in Box 2 to frame situations and then apply the relevant questions in Table 3. By leveraging their insights and expertise to select the most relevant questions, technical communicators will create sites of interpretation suited to a particular needed intervention.
Bowdon and Scott’s framework is an important departure point for analyzing the intercultural rhetorical situations in which regulatory patient safety narratives operate. It can also help define a rational community within which these narratives function. In the context of patient safety narratives, this framework asks users to identify sites at which technical communication interventions might inform uses of the source discourse, such as international biomedicine. Such factors parallel ideas put forth by Melonçon (2017) and St.Amant (2017). However, in such intercultural settings, as well as in health care more generally, additional invention questions might be useful (St.Amant, 2017).
Table 4 provides invention questions designed to aid technical communicators seeking to work in intercultural health-care settings. By applying these invention questions, technical communicators can better interrogate the intercultural impacts of source documentation and their own work (Ding, 2014; Sun, 2012). We use these questions to examine different models of patient narratives in intercultural communication.
Invention Questions for Technical Communication: Intercultural and Health Care.

In addition, we situate the patient safety narrative as a genre by providing information about its origins, exigences, audiences, institutional constraints, and producers. In other words, we provide a framework for technical communicators to explain where the conventions of safety narratives arose, the difficulties of producing them, and the ways that their audiences and writers interact. We show that the synergy of patient safety narratives, additional medical information, and the respective formats of all of these materials form a vital exigency, features of a discursive culture that always necessarily transcends the boundaries of a single nation. The nature of such situations makes them worthy of consideration by technical communicators.
Regulatory Tensions
Patient safety narratives appear in regulatory documents, where individual patients can easily be lost among the logistics of international government regulation and large-scale, multinational research. Individual participants must be anonymized to maintain privacy and prevent bias, further attenuating humanistic engagement. As Ledade, Jain, Darji, and Gupta (2017) explain, “Narrative writing involves multiple activities such as generation of patient profiles, review of data sources—which include individual listings of data by patient—and identification of events for which narratives are required” (p. 58). This content (described in Box 1) derives from multiple regulated sources supported by practices, such as quality control, to prevent error. Such narratives, like the reports in which they appear, must simultaneously meet the needs for each health authority to which they will be submitted. Thus, regulatory patient safety narratives present a globally significant problem of complex information as understood in technical communication (Albers, 2004) and a mix of intercultural requirements.
Metadiscursive work by and for regulatory documentation experts (DeTora, 2017; Wood & Foote, 2008) defines writerly roles for patient safety narratives. Moons (2015) recommends a process for medical writers producing patient safety narratives (Figure 1 shows a simplified version) in any country or language. Of note, this narrative review process occurs before the clinical study report review described by Cuppan and Bernhardt (2012). Audience expectations of patient safety narratives include factual accuracy and conciseness, while institutional expectations include quality control and approval by qualified experts. The complexity of the process Moons describes fostered current moves to automate narratives to aid both production and translation across languages, thus enhancing intercultural and multinational exchange (Quanticate, 2017).

Simplified process for producing patient safety narratives. In the less simplified version, multiple rounds of scientific and medical review are necessary.
Automation and semiautomation of patient safety narratives, however, raises questions about the nature of these texts (Quanticate, 2017). Automation enhances efficiency by limiting production steps and creating consistent, searchable text that can facilitate certain types of regulatory review. Yet these very features move away from true narrative, creating rhetorical situations in which the invention questions we listed earlier no longer operate clearly. In presenting design challenges, automated narratives offer an opportunity for technical communication insights. For example, if increased automation is a response to shifting audience needs, then perhaps more creative solutions might be identified by asking questions such as those in Box 2. Given the worldwide use of patient safety narratives worldwide to foster regulatory decision-making, solutions would require intercultural awareness, which might be addressed by the invention questions in Table 4. Understanding a broader tradition of patient narratives would also assist in this endeavor.
Narrative Contexts for Patient Safety Narratives
A difficulty in analyzing patient safety narratives as rhetorical output is their contradictory relationship to both individual experience and narrative use in medical education and practice. Clinical understandings of narrative often abjure readers to balance literary and artistic interpretations (Ohio State University, 2018) against medical practice (Charon, 2001). In her treatise on the promising vantages literary epistemologies make available to medical practitioners, Charon (2006) shows how narrative serves as an operative term through which generative dispositions in medical contexts are wrought. Her approach “brings powerful narrative skills of radical listening and creativity from the humanities and the arts to address the needs of all who seek and deliver health care” (Columbia University College of Physicians and Surgeons, 2018, np). Charon (2001) promotes “medicine practiced with the narrative competence to recognize, absorb, interpret, and be moved by the stories of illness” told by patients, clinicians, and family members who experience illness, recovery, hope, and healing (p. vii). These concerns easily fulfill Miller’s notion of a communal rationality.
Charon treats humanistic insights as secondary to patient care, offering a practical model of communal rationality by emphasizing human welfare preferentially to considering stories as an end in themselves. Das Gupta’s (2008) critical emendation of narrative competence to encourage narrative humility draws on an intercultural concept: cultural humility. For Das Gupta, an awareness of cultural humility, or the notion that no social science can uncover the full truth about cultural experience, informs narrative competence by encouraging readers, physicians, and others to identify their own limitations. An acknowledgment of personal limitations can also inform the technical communications invention activities we recommend. Acknowledging our own limited understanding promotes a truer picture of technical documentation and its potential intercultural impacts.
Technical communication studies have examined vital connections between storytelling and medical documentation in various patient-focused settings (Angeli, 2019; Munger, 1999, 2000). Such work emphasizes the inherent difficulties in translating verbal communication into medical practice and useful patient information as well as critical limitations of structured documentation in relating authentic experience (Melonçon, 2017). These observations highlight differences between humanistic narrative and regulatory patient safety narratives, offering a model for reading regulatory documentation more generally.
To bridge the differences between regulatory documentation and more normative narrative models of patient experience, technical communicators can employ narrative competence and narrative humility by deepening their understanding and acknowledging the limitations of various intellectual and practical approaches to health information. Technical communicators might use the invention questions in Tables 3 and 4 to promote narrative competence, ensuring that their understanding of regulatory or other medical information would accord with that of its makers and primary audiences (i.e., regulators) before offering adaptive interpretations. Narrative humility, which carries a heavy intercultural component, could then be employed as a reminder that adaptations of complex information for normative uses are never perfect, no matter how confident an adaptor feels about the reception of medical or regulatory content. Such approaches could both better meet the needs of given audiences and contribute value to both the users and creators of technical materials (Melonçon, 2017; St.Amant, 2016).
In terms of the international and intercultural, narrative competence and narrative humility can help technical communicators better consider aspects of context that affect the expectations, needs, and preferences of different audiences. Doing so could help account for cultural aspects that guide the use of materials and guide designs accordingly (Sun, 2012). Such an approach could also help create materials that work effectively across different cultural contexts and facilitate international health and medical discourse (Ding, 2014). Finally, technical communicators can use narrative competence to more accurately map and identify the variables affecting access to and uses of health and medical materials in different national and cultural contexts (St.Amant, 2017). Narrative competence and humility can help technical communicators become more effective contributors—and individuals who add increased value—to international and intercultural health and medical communication practices.
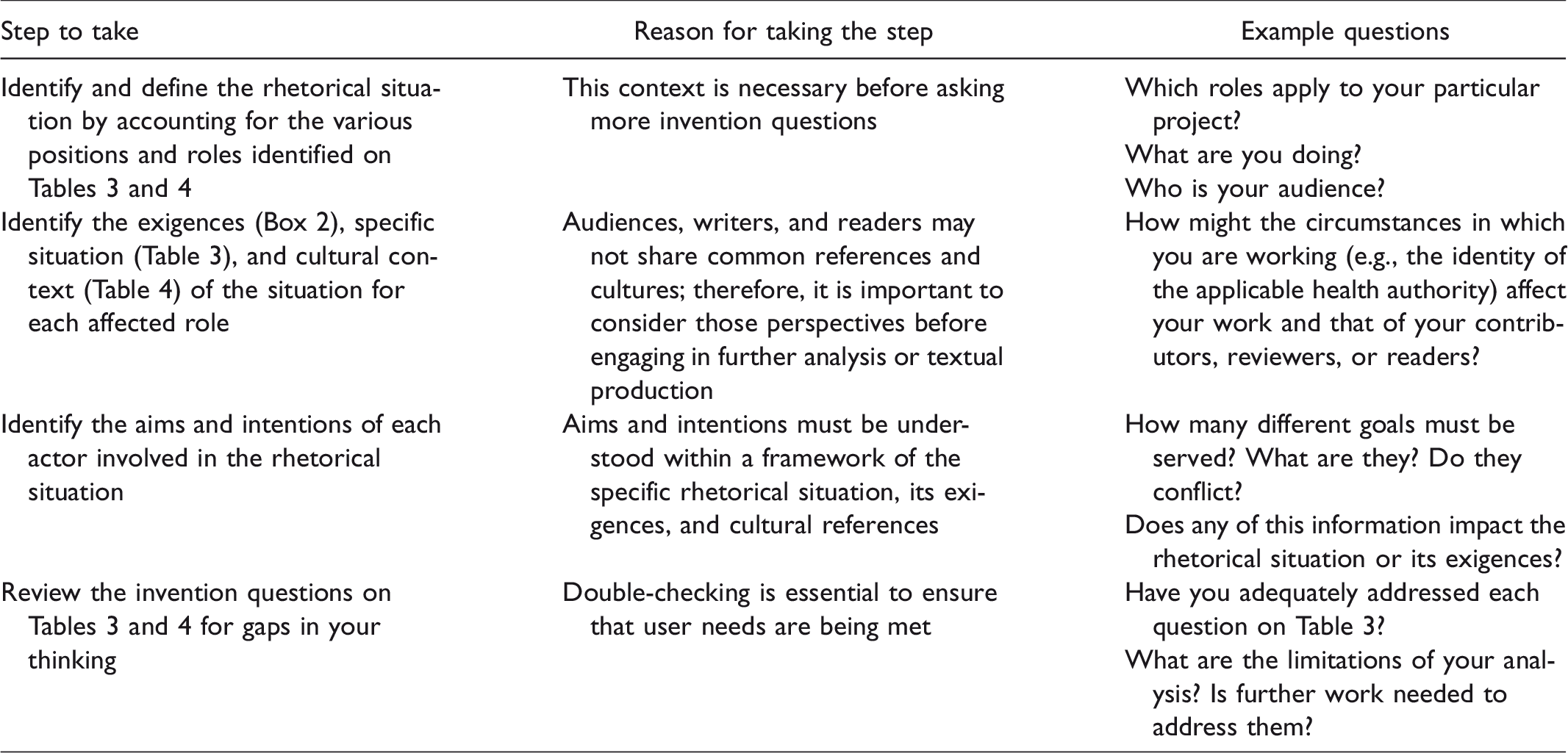
Before closing this discussion, we offer a final, synthetic view of the analysis and invention questions we have presented in Table 5 which illustrates a heuristic for reading patient safety narratives and other intercultural technical documents.
A Sample Heuristic for Applying Analytical Strategies in Technical Communication Practice.
Exigence, Invention, and Intercultural Communication
Narrative formats serve many health-care functions both for individuals and for research, thus having both personal and intercultural impacts. Humanistic readings might identify individual patient safety narratives as increasingly dehumanized automation, rather than a means of protecting other patients or an adjunct to the concerns of narrative medicine. As we have shown, however, applying invention questions can go a long way toward clarifying the intentions and purpose of such documentation. For example, if key audience needs are speedy, consistent narrative production to prevent additional deaths, then automation may take on a greater appearance of communal rationality.
For Miller (1979), implicit invitations to participate in language communities require an awareness of their “concepts, values, traditions, and style” (p. 617). Biomedical language communities are no different. We situated the regulatory patient safety narrative, a globally mandated format for representing individual patient experiences, against associated biomedical discourses such as peer-reviewed case reports and narrative medicine, which uses stories of illness to promote the delivery of effective health care. Each of these discourses crosses national and cultural boundaries. By examining not only an individual problem but also its broader, intercultural context, technical communicators can strengthen our own practices within technical communication and the rhetorics of health and science. Of further significance, we identified a role for technical communication expertise in each of the narrative settings we reviewed.
Technical communicators navigate among disciplinary and methodological boundaries and possess the rhetorical and pragmatic power to consider different types of patient narratives from a unique vantage point. What technical communication may offer related rhetorical situations is a constructive framework for identifying exigency and purpose: This type of inquiry and questioning offers options other than imposing either humanistic concerns or technical requirements preferentially. By reflecting on various rhetorical exigences and incorporating observations into their pedagogies, technical communication experts have an opportunity to influence multiple discourses of health-care narratives both now and in the future. However, as Bowdon and Scott suggest, valuable suggestions require sustained attention and knowledge. It is up to technical communicators to identify the exigences and aims of this work.
Footnotes
Acknowledgments
The authors are grateful to the anonymous reviewers, Kristi Shackelford for copyediting advice and Kirk St.Amant for editorial review and guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.