
Abstract
Meeting the needs of users requires an understanding of the contexts where they interact with materials. This entry presents an approach for integrating script theory into usability to develop medical materials individuals can use in the settings where they receive or perform healthcare activities. The entry introduces technical communication professionals to script theory and presents mechanisms for using script theory to research patient expectations of and presents usable materials for health and medical contexts.
Keywords
Meeting audience needs requires an understanding of where individuals use items (Garrett, 2010; Norman, 2002). This relationship can be particularly acute in healthcare situations where audiences participate in health, wellness, and medical activities in various environments. As each setting can contain its own unique conditions, how to safely and effectively engage in health and medical activities could vary from location to location. Failure to address such differences when creating medical materials could result in injury or even death. As more individuals rely on personal technologies and self-administered care for wellness, this need for effective usability in healthcare contexts will only increase.
To address such factors, certain scholars have advocated applying usability approaches to healthcare contexts (see Heifferon, 2004; Melonçon, 2016, 2017; St.Amant, 2017a). The objective is to provide individuals with information, designs, and technologies they can readily use based on where they engage in healthcare activities. The challenge involves identifying variables affecting usability in different contexts. The cognitive concepts of scripts and prototypes can help technical communicators accomplish this objective. By providing a framework for identifying variables affecting usability in healthcare situations, scripts and prototypes can help technical communicators meet usability expectations in healthcare contexts.
Usability and Healthcare
Effective healthcare is often a matter of usability (Melonçon, 2016, 2017). If individuals cannot effectively use something to achieve a healthcare objective, then successful care often cannot be provided. Similarly, an inability to use an item correctly in a healthcare context can have adverse results ranging from minor injuries to the death of a patient (Clark & Israelski, 2012; Zhang et al., 2003). In fact, failure to address usability in healthcare has contributed to medical errors becoming a leading cause of death in the United States (Cha, 2016). For these reasons, many healthcare organizations advocate for a usability focus when developing medical products (U.S. Food and Drug Administration, 2016). Certain groups have even created guidelines for integrating usability into the development of healthcare materials, and even regulatory agencies encourage usability in the planning and development of different healthcare products (Callan & Gwynne, 1993; NWX-FDA OC, 2016). Interest in this area has also grown within technical communication where scholars such as Melonçon (2016, 2017) and Batova (2010) note the need to integrate user experience design practices into health communication contexts.
Central factors driving these dynamics are the increase in non-healthcare professionals performing caregiving activities and the location where such activities occur. Over the last decade, the time dedicated to providing patients with dedicated care in contexts like hospitals has decreased (Kalra et al., 2010). Moreover, the amount of time healthcare providers spend interacting with patients remains limited on average (Heath, 2016; Rabin, 2014). Such situations increasingly leave individuals to perform healthcare activities on their own and without the supervision of a trained healthcare professional. This situation means the contexts where such activities occur can be quite broad.
In addition, the number of mass-market technologies for monitoring personal health or treating one’s own medical conditions is growing (Mamtani, 2017; Phaneuf, 2020). These technologies include everything from websites explaining how to identify illnesses to apps that monitor biochemical processes to video tutorials on how to administer treatments. The processes these technologies cover is also expanding to include a range of medical situations and a variety of treatments (Mamtani, 2017; Phaneuf, 2020). As such, the number of non-healthcare professionals engaged in healthcare activities will likely increase over time.
Further complicating this situation is the adoption of electronic health records and information communication technologies for telehealth activities (Agency for Healthcare and Research Quality, 2018; Hecht, 2019). While these systems allow patients to provide information or interact with healthcare workers, they often require patients to input crucial medical data via different interfaces. Yet expectations for what information to collect, how, and the method of collection, can vary across systems and affect results. The contexts where individuals enter such data and interact with systems can affect the kind and quality of data provided. Such contexts can also affect the comprehensibility and usability of the interfaces individuals rely on to provide this input. As artificial intelligence (AI) technologies increasingly review such data and prescribe care, usability factors affecting how patients input information can markedly affect the resulting care received (Artificial Intelligence in Medicine, 2019; Hall, 2016; Page, 2018).
Central to these situations is knowing how patient experiences affect interactions with healthcare technologies (Melonçon, 2016, 2017). Yet individuals are increasingly using such technologies to perform care processes—activities associated with maintaining or restoring the health and wellness of individuals—outside of formal healthcare contexts. The creators of healthcare content therefore need mechanisms for understanding and addressing the contexts where individuals perform healthcare processes or use health-related technologies.
Cognition, Expectations, and Usability
We learn what items are and how to use them based on our experiences (Norman, 2002; Otto & Smith, 2013; Petroski, 1992). Either someone provides us with instruction for using an object, or we mimic the behaviors we observe others performing when they use an item (Berry et al., 2002; Cronk, 1999). The more often we are instructed in or observe the uses of an item, the easier such processes become until they seem almost reflexive. In these ways, our experiences teach us what items are and how they are used. Essentially, our minds use repeated exposure to create a mental model that represents what an object is, what it does, and how it is used. Whenever we encounter an object, we access that model to determine what at item is and does. This is how experience creates usability expectations.
None of us, for example, intuitively knows what a stethoscope is or how it is used to check a heartbeat. Rather, we observed or were provided with explanations of what a stethoscope is and does. The more often we are exposed to such factors, the more our mental model develops until we can see a stethoscope and instantly recognize what it is and how it is used. These factors apply regardless of if one uses a pen to take notes to a sphygmomanometer to check blood pressure. As a result, without experiences to identify what items are and how to use them, they remain unknown and risk being unused or misused.
The design of items is central to this process. The first time I learn what an object is, my mind creates a mental model, or representation, of it. Specifically, my mind notes the features of that item (Aitchison, 1994; St.Amant, 2005). So, the first time I encounter a stethoscope, my mind creates an entry for its features in a mental database of models I use to identify objects. Every time I encounter something identified as a “stethoscope,” I compare it to my mental model for “stethoscope” to see if that object has features in common with that model. Through repeated exposure/experiences, common features become reinforced as central to identifying what that item is. Non-common features, conversely, are omitted from this mental model, for they are not essential to effective identification. In this way, experiences shape expectations of what features something should have for me to recognize it.
We learn the uses of items in a similar way. Either someone instructs us in how to use an object, or we observe how others operate an item to determine its use (Berry et al., 2002; St.Amant, 2018). The more we see similar uses of that item, the more that use becomes established in our mental model for the item. So, our initial observations of using an adhesive bandage (e.g., a Band-Aid™) provide us with an initial mental model for how to use (apply) an adhesive bandage. The more we see this process repeated, the stronger this association becomes for how to use an item.
The associations we have for mental models can also inhibit how we recognize and use objects (Aitchison, 1994; St.Amant, 2005). Imagine your prior experiences taking your blood pressure involved using an analog sphygmomanometer (blood pressure cuff). You then encounter a fully digital one. Would you recognize what it is, or would you think it is something else—say a strange digital watch? Would you overlook it completely? Similarly, if someone told you what that item was (“It’s a digital blood pressure cuff.”), would you know how to use it? Probably not. In this example, you know how to perform a healthcare process, so the knowledge of the care-related activity—what that activity is and how to do it—is not the issue. Rather, you do not know how to identify or use the item available to perform that process. Per the blood pressure example: You know the process for taking blood pressure (restricting then restarting the flow of blood and taking a measurement at key points), but you don’t know how to use the items available to perform this process. In these ways, usability issues can greatly affect actions in healthcare contexts.
Interestingly, the relationship of mental models to usability involve where one learns to identify and use items (St.Amant, 2017b, 2018; Tomkins, 1978, 1987). This is because many objects can be used in different ways, but the context where individuals encounter them determines the related use. In the context of a construction site, one readily recognizes a hammer as a tool for pounding nails and knows the force needed to use a hammer to achieve this objective. In a hospital examining room, one would associate a hammer with testing a patient’s reflexes and related use involving gently tapping a patient’s kneecap to achieve that objective.
Mental Models and Categorizing Contexts
Many cognitive processes involve minimizing the information our brains process at one time (Duhigg, 2012; Eyal, 2014; Ratey, 2002). Essentially, when I see a stethoscope, I don’t view it as its individual parts. Rather, I view those parts as characteristics combined into a single entity for consideration (a stethoscope) (Aitchison, 1994; Ratey, 2002). Moreover, I don’t associate that stethoscope with a wide range of uses, but assume it will be used for certain functions. I also have certain expectations of who will use it and how. All of these factors reflect my prior experiences with stethoscopes (Aitchison, 1994; St.Amant, 2017b).
The combining of factors means all of that information does not exist as a separate items requiring individual processing when I encounter a stethoscope. Rather, my mind has created a mental model, or prototype, that combines these elements into a single unit to consider as one thing (Duhigg, 2012; Ratey, 2002; St.Amant, 2017b). This is why I can instantly identify what a known item is and does upon encountering it. When you recognize an object, you call up all of that associated information at once (one unit) vs. recalling each aspect of design, use, etc., separately (Aitchison, 1994; St.Amant, 2018).
The more information mental models pack into integrated units, the more efficiently individuals can engage in activities, for their minds have the free space to do so. Interacting in a context, however, requires more than recognizing individual objects. Instead, the brain uses a different mental model—known as a script—to package information about behavior in locations (Tomkins, 1978, 1987). Scripts, the mental models humans use to collect information on and perform activities in a location or context, are a key cognitive item affecting usability in context of care. This is because they govern what individuals expect to do, to use, and how when performing activities—such as monitoring or treating one’s health—in a setting.
For technical communicators, there are five script factors affecting audience analysis related to usability and design expectations. These are
The context (or setting) where an activity occurs The activities that take place in a setting in relation to completing a process Who in a location undertakes these activities What individuals use for these tasks How individuals and information enters and exits the context where a process occurs
The better technical communicators understand these factors and how scripts influence audience expectations, the more effective they can research scripts to determine audience expectations of usability in different contexts of care.
Spaces, Scripts, and Scenarios
Scripts are the mental models we use to manage how we behave—and use items—in familiar contexts. They aggregate the details we associate with performing activities in a context (who is there, what is there, what is used, how it is used, how to enter and exit that setting) into a single unit for cognitive processing (Norman, 2002; St.Amant, 2017b, 2018; Tomkins, 1978, 1987). This is why many of us seem to operate on reflex when we perform seemingly complex activities in familiar contexts. Many of us, for example, can enter a location, know where we are, and automatically begin to use certain items to perform certain tasks. It is also why we can easily engage in cognitively challenging activities—such as having a conversation—while easily performing familiar tasks in a known context.
Like prototypes, we form scripts based on repeated experiences we’ve had in certain contexts (St.Amant, 2017b; Tomkins, 1978, 1987). The more I visit a physician’s office, the more accustomed I become to certain elements, individuals, and activities occurring in that location. Through such exposure, I combine factors into a single script for what occurs in that setting (Tomkins, 1978, 1987). Such factors influence usability in terms of what activities I expect to be performed in a location, by whom, with what, and how (St.Amant, 2017b, 2018).
These scripts are why so many of us can automatically move through care-related activities in certain contexts, like hospitals (St.Amant, 2017a). We know our experiences will consist of certain activities in that context (e.g., a hospital) and involve certain objects (e.g., computers for check in, stethoscopes for monitoring heartbeat, etc.) and individuals (e.g., clerk who checks us in, physicians who assesses wellness, etc.). Each object used and every person who interacts with us is an independent prototype we associate with activities in this context (St.Amant, 2017b, 2018). Each of these prototypes is a combination of characteristics (e.g., shape and size for objects, dress for persons) we use to recognize items and identify associated use in that context. Scripts, thus, combine multiple, context-related prototypes into a single unit and minimize the information our brains process when interacting in locations (St.Amant, 2018).
For these reasons, scripts are essential to usability and to successful care across medical and health contexts. We expect healthcare providers to readily recognize and use certain tools, reflexively perform essential processes, quickly identify conditions, and readily provide associated care. This confluence of activities only occurs when the contexts where we receive or administer care match our scripts for care-related activities in a contexts of care, or the setting where care activities occur (St.Amant, 2017a).
These factors mean effective usability in contexts of care involves understanding the scripts individuals use to guide their expectations, activities, and uses of items in a setting (Schank & Abelson, 1977; Tomkins, 1978, 1987). Conversely, when our scripts do not align with a context of care, problems occur (St.Amant, 2017a). In some cases, these problems reflect an inability to recognize or use items in a setting. In others, they involve a failure to use items correctly based on the parameters of a setting. Occasionally, they reveal an inability to know how to provide care or a refusal to accept care based on a perceived lack of credibility associated with an individual or a process. For these reasons, technical communicators need to map such scripts in order to identify what key variables are and determine how individuals recognize them (St.Amant, 2017b, 2018). Technical communicators can then follow these maps to create products that address an individual's usability expectations for contexts of care.
Mapping Scripts and Categorizing Contexts of Care
The first and largest level of organization within scripts are the major activities that occur in a context. These are the acts of the overall script (St.Amant, 2018). The first act of the script (Act 1) for “annual physical,” for example, is likely “checking in at the reception area”—a complex activity that is part of a greater process and that occurs in a particular setting.
Each act consists of different actions, or scenes, that contribute to that overall process within acts (Tomkins, 1978, 1987). For the check-in process, the specific actions occurring could be entering at the reception area, checking in at reception desk, and waiting to be seen. Each activity represents a scene our minds associate with Act 1 of our overall script for “annual physical exam.” The related mental model would look like Figure 1.
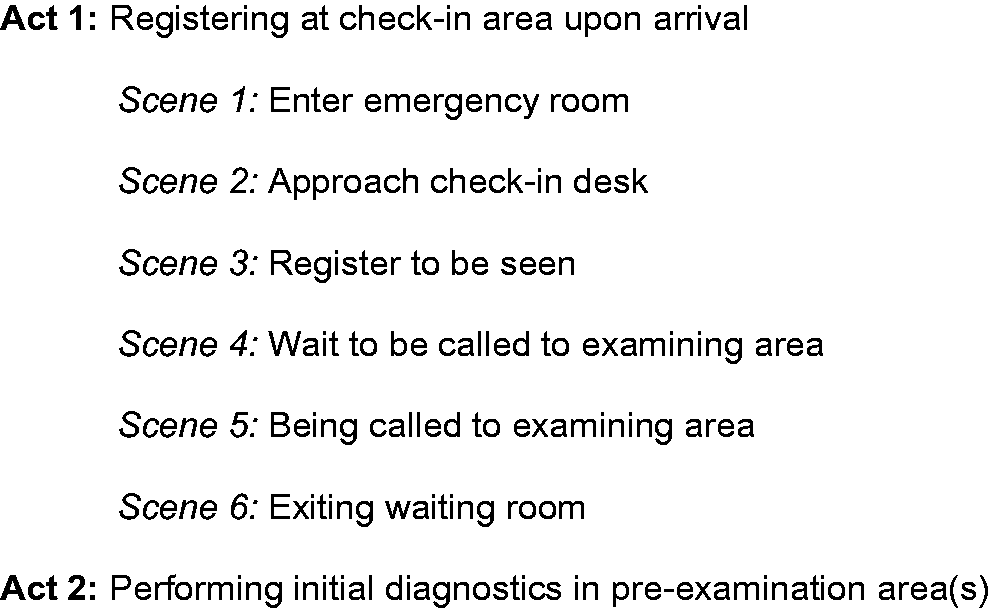
Script for Visiting Emergency Room to Have Condition Assessed.
Each scene is composed of key elements. First, one must enter the scene—a process expected to occur via a particular method of entry into a context. This element is entry conditions and is why we are often surprised when individuals enter a location in unexpected ways (Schank & Abelson, 1977). Upon entry, each process performed involves persons (roles) who perform certain activities using specific things (props) (Tomkins, 1978, 1987).
For the scene of “checking in,” the roles are patient and receptionist, and both are expected to use certain props to complete the check-in activity (St.Amant, 2017b; Tomkins, 1978, 1987). For the patient, the prop might be an insurance card with specific information. For the receptionist, the props would likely be a computer for recording patient data—including insurance card information. Individual might also be expected to dress a certain way that identifies their role in this scene (e.g., receptionist wears a nametag with the hospital’s logo), and the parties might be expected to use certain phrases, or dialogue, to engage in this process (clerk saying “Can I help you?” to indicate the start of the check-in process) (St.Amant, 2017b, 2018). In this sequence of events, individuals expect certain objects and persons to be present, and use prototypes of what these items or persons resemble and what the person should use to guide their behavior in this scene (St.Amant, 2018). The related script map might resemble Figure 2.
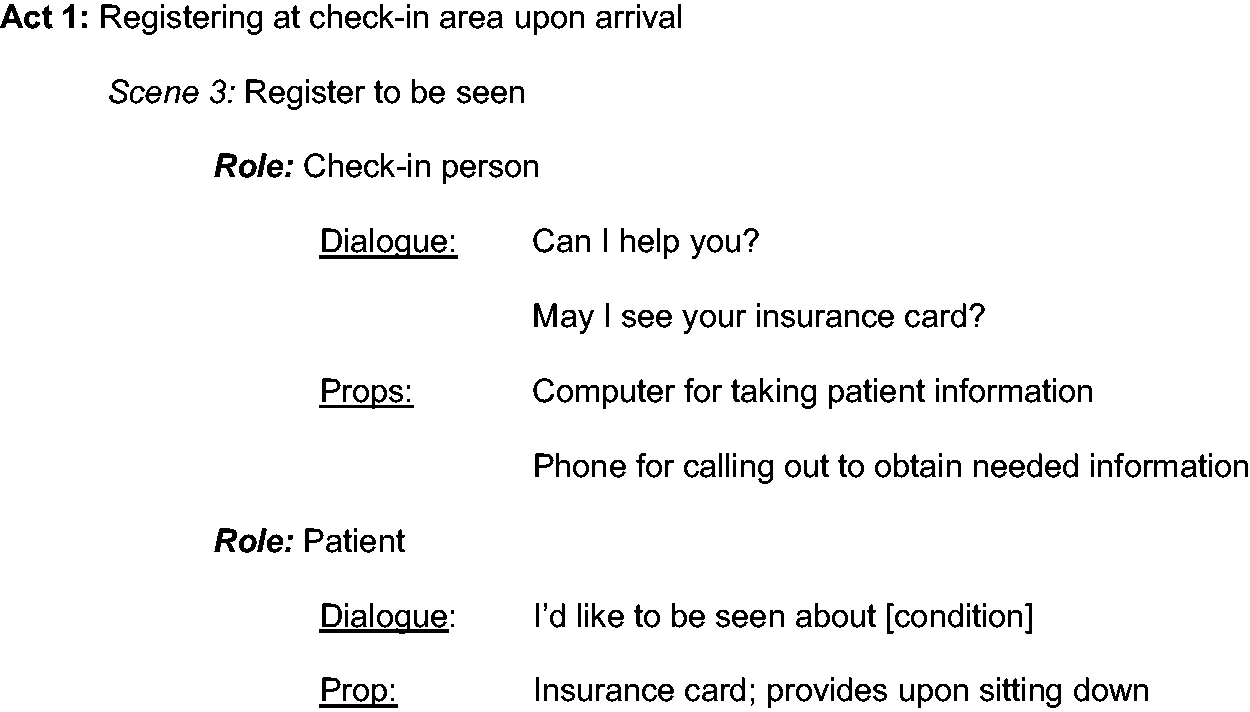
Components of an Act in the Script for Visiting Emergency Room to Have Condition Assessed.
The scenes in the act proceed until all expected activity in that setting is completed and the individual needs to move to a new context, or act, to perform the next series of activities (scenes) in the overall process. At this point, individuals must exit their current context—and the related act—in a certain way in order to move to the next context in the process. Per the physical exam scenario, the patient often needs to remain in the waiting area until called by another individual – often a nurse. The patient then follows that nurse (generally through a doorway near the check-in desk) to the location where the next activities in the overall process occur. The elements associated with how individuals leave one setting and enter another are the exit conditions governing how we expect to move from point to point in a script (Schank & Abelson, 1977). They also explain why, in healthcare contexts, we seem comfortable following a relative stranger to an unknown location without question.
In the next act of our script, the elements and general format repeat themselves. We enter the next context a certain way (entry conditions) and interact with particular individuals (roles). These individuals perform certain activities (scenes) using particular objects (props) and often guide us via particular phrases (dialogue) (St.Amant, 2017b, 2018). Once the activities/scenes for that act are complete, we follow a particular protocol to move to the next context in the script (exit conditions) where these elements appear again and guide our activities in that new space.
These repeated variables, of acts, scenes, roles, props, and dialogue, entry conditions, and exit conditions are central to how we engage in care-related practices and use items to perform healthcare activities in a context. They reflect our prior experiences receiving care in certain settings, and they can be central to usability issues in contexts of care.
Scripts, Disconnects, and Usability Issues in Contexts of Care
While scripts can facilitate our use of items, they can also make us unaware of the usability expectations of others. This situation arises because we often use our own scripts for performing a process to guide how we design materials for others (Eyal, 2014; Lindstrom, 2010; St.Amant, 2017b). In doing so, we assume individuals will be in the same context we usually are when performing a process and will have access to the same items and individuals we consider central to that process. These assumptions can cause usability-related errors in healthcare situations.
Imagine my experiences having blood pressure taken involved going to my physician’s office and sitting passively as my physician (or a nurse) uses a stethoscope and a manual sphygmomanometer to assess my blood pressure, evaluate the results, and suggest a course of care based on these readings (e.g., suggests doing more exercise or prescribes a medication). This script has me playing a passive role, and I depend on other persons (roles) to provide and use the elements (props) involved in the process. In addition, I know how to proceed upon leaving that location in terms of what to do next (e.g., exercise more) or where to go next (e.g., to a pharmacy to obtain a prescription)—the exit conditions for that event.
Let’s imagine your experiences are different. You take your own blood pressure in the kitchen of your home while both watching your small children and preparing dinner. You use an automatic blood pressure cuff you plug into a wall outlet before pressing certain buttons and allowing the cuff to inflate, deflate, and register a reading. You must then determine what your systolic/diastolic readings mean via pamphlets from a local clinic, and your treatment is based on what you find on websites identified during a Google search.
In your script, not only is the setting different, but so are the roles and props involved in the process, entry conditions for bringing information into that location (e.g., pamphlets on assessing blood pressure), and the exit conditions for where to go and what to do after the process is complete. Moreover, your script contains additional roles (children home from school) and props (pans on the stove) that can distract you while performing activities. Likewise, certain environmental factors (e.g., an outlet to access power for the device) are essential entry conditions (bring a needed resource into the environment) as are one’s internet connection for determining a course of care.
Both scenarios encompass the same healthcare process, but each represent different experiences shaping care expectations. Should individuals from the first scenario create instructions for how to monitor blood pressure, they will use their experiences in a physician’s office and design materials for trained healthcare workers to use in a healthcare setting. The content designers will likely also assume the user’s knowledge of the process, including understanding what measurements indicate low, normal, and high blood pressure as well as prospective care for such conditions. Per documentation created for the patient, materials designed for such contexts would likely focus on how to prepare for and what to do so someone else can perform an activity on them vs. do it themselves.
Persons whose experiences correspond to the second scenario (checking one’s blood pressure at home) would likely find instructional documentation designed for healthcare providers ineffective. This second audience instead needs content that reflect their experiences and provide information on how to use a technology to perform the activity themselves. This audience also needs information on how to interpret results and how to respond to these interpretations—including rubrics they can understand and suggestions for researching care options.
Not only can script disconnects lead to different expectations of the kind of content needed, but also the mechanism for delivering the same content. Consider the situation where I need to provide you with instructions on how to use a newly developed technology to check your blood sugar levels. You and I will both use the same technology and perform the same process in the same way. The location in which we undertake this common activity, however, is different. I will use the technology while sitting quietly at my kitchen table at the start of the day or sitting quietly at my desk during my lunch break at work. In this situation, printed documentation—such as a booklet—could serve as an effective method for conveying content I can readily use based on my script expectations for where I perform this process.
You, in contrast, need to perform the related process on crowded commuter train on the way to work. In this situation, you may or may not be able to sit down when using the device, and your ability to open and leaf through a printed text—like a booklet—is limited. The same situation is the case when you attempt to user the monitoring device during your lunch break on a busy construction site where place to sit is limited as is the space available to open and read through a printed booklet. In your script, what you need—and have come to rely on—for content delivery are instructional videos you can watch on your mobile phone as you hold it in one hand and perform the related process with the other. In these cases, it is not the content of the printed manual that renders it unusable in your context of care. Rather, it is the modality used to convey that content that creates script-related usability issues.
These example situations increasingly represent today’s healthcare context where individuals use technologies to perform healthcare activities on themselves or a loved one (Gittel, 2009; Gouge, 2016; Woods, 2019). For these reasons, technical communicator need to become involved in creating health and medical materials to address audience usability expectations and avoid assumptions that could affect usability. Technical communicators can use an understanding of scripts to identify such expectations and develop materials that are usable in relation to audience experiences for a context of care.
Researching Scripts and Mapping Contexts of Use
Understanding scripts is central to creating materials audiences can recognize and use. Doing so involves identifying two factors:
Factor 1: Script Elements—The items individuals associate with performing a process in a context. These include acts, scenes, roles, dialogue, props, entry conditions, and exit conditions (St.Amant, 2017b, 2018). Factor 2: Prototypes for Elements—Recognition of the contexts, persons, and items involved in a process and the prototypes used to identify them. Technical communicators need to determine what a script item “is” and should resemble so individuals recognize it within the context of that script (St.Amant, 2017b, 2018). Interviews can provide insights on individual assumptions, perspectives, and preferences for a context Focus group can help identify usability expectations groups associate with a context (InterQ, 2020; Schwab, 2020)
Identifying these factors requires technical communicators to collect information from the intended audience, and they can use both interviews and focus groups to do so as
Technical communicators can use the resulting data to identify patterns audiences associate with the script for a healthcare activity (St.Amant, 2017a). This information can help technical communicators determine what characteristics groups associate with identifying and using items in that context (St.Amant, 2017b, 2018). Technical communicators can use this knowledge to map out the scripts an audience uses to engage in a healthcare activity. The objective is to create a script map resembling Table 1.
Map of a Script Sequence.

Note. See St.Amant (2017b, 2018).
Questions to Guide Data Collection
Understanding an audience’s script expectations for a context of care requires technical communicators to interact directly with members of the intended audience to collect information on these expectations. Doing so involves collecting script-related information in a particular, systematic way that prompts audiences to access the correct script for a context of care. Such a systematic questioning can help technical communicators identify the core variables affecting usability expectations in the script for a context of care. For this reason, identification of an audience’s script expectations requires technical communicators to ask certain questions in a particular order (St.Amant, 2020). This progression of questioning, however, also requires technical communicators to assess the responses they receive to earlier questions to guide the nature of the subsequent questions they ask in this process. Failure to do so can result in decontextualized information that does not effectively or completely reflect audience expectations of a script for a context of care.
Technical communicators can address these factors via a scaffolded approach to questioning in which the responses to one set of questions lays the foundation for the next set of questions. They key is to slowly and progressively identify the script for the actual context of care an audience associates with a healthcare activity. Technical communicators can then identify the different script-related variables for expected script activities and associated usability in this context. This approach should resemble the sequence of questioning described here.
Question 1: When Do You Do X (Care Activity)?
While location is key to script expectations, time is perhaps more crucial. The time when individuals perform an activity affects who is in a location, what is available, and what is occurring in a space. While subjects will have a distinct prototype of the place for where they perform a care activity, the dynamics of that location likely change during the day.
If technical communicators lead with a location question (e.g., “Where do you check your insulin levels?”), subjects might access an inaccurate prototype of the place (e.g., accessing the prototype for “kitchen” as an idealized or decontextualized space). Subjects might use this idealized alternative mental model when responding to questions on performing a care-related activity. In so doing, they might overlook important elements—individuals or items—that only appear in that space at a certain time. To avoid this problem, technical communicators should have subjects first note when they perform the activity and then ask about location used at that time.
Question 2: Where Do You Perform X (Care Activity) at That Time?
Once the individual is prompted by the time question, technical communicators can ask them to access the mental model for the context where they perform a process. This is the script technical communicators need to map in order to understand an audience’s usability expectations for a context of care.
To make sure subjects access the correct script, the location question should directly connect to the time when the activity occurs in that context. Adding the phrasing “at that time” re-enforces this connection and ensures subjects access the correct script for a context of care.
Question 3: Can You Describe X (Location) to Me? What and Who Is There?
Once subjects identify the setting, technical communicators must determine the features considered essential to identifying that context. Answers can provide insights into the items or persons an audience expects to encounter in that setting and that might play a part in the related process. If possible, technical communicators might also ask subjects to draw a sketch of that context when responding to this question. While sketching, subjects would need to
Label the objects and persons in that context Note where items or individuals are located in that context Identify their location and vantage point in that context during the process
The combined sketches and descriptions can help identify expected dynamics and anticipated items within that context of care.
Question 4: Can You Describe How You Do X (Care Activity) in Y (location) at That Time? What Is the First Thing You Do? The Next? The Next?
The next part of the process involves collecting information on the script dynamics for each action in an overall healthcare process. To achieve this objective, technical communicators should have subjects describe each activity and note the items and individuals involved in each step. Doing so identifies the script elements of scenes (individual actions within a location), roles (persons who perform key activities in a process), and props (items used to perform processes). To collect such data, technical communicators must ask subjects to respond to Questions 4a and 4b (listed next) to isolate script dynamics affecting this process.
Question 4a: What Do You Used to Do Z (Perform Activity in Overall Process)? Can You Describe A (Object Used) for Me? Where Do You Get That Item?/Where Do You Store That Item?
Technical communicators need to identify the prototype expectations for identifying items audiences expect to use when performing each activity in a process. Doing so involves subjects describing such items to identify the features they should have so individuals can recognize and use them during the process. Having subjects provide information on the characteristics used to identify such object prototypes helps with understanding perceptions of how actions should occur. In collecting this information, technical communicators need to ask prototype identification questions of “What is used?” and “Can you describe it?” for each activity in an overall process.
Other factors to address are the entry conditions for each scene—or where the items essential to performing a process come from. Such factors can affect how individuals expect to move within a context to locate and use needed items during a process. Entry conditions can also affect where the individual is positioned and how during different steps in a process. In collecting this data, technical communicators might need to create a rough map or sketch in which they plot where the individual is and what is nearby at different parts of the process.
Question 4b: Is Anyone in Y (Location) When You Are Doing X (Care Activity)? Do They Help With X (Process)? If So, What Do They Do, How, and Using What? If No, What Are They Doing While You Do X (Activity) in Y (Location)?
The individuals in a context of care (roles) could affect or be involved with different parts of or steps in the overall process being performed. Technical communicators need to identify who is there and what they do or how they affect activities associated with care, and these questions help identify such factors.
If an individual is identified as playing a role in a process (e.g., positioning a blood pressure cuff) or performing an activity in the process (e.g., using a blood pressure cuff to take the individual’s blood pressure), technical communicators also need to question that person in order to determine
What activities these individuals perform (roles) in an overall process (act) How they identify and use objects (prototypes for props) in that space Where they obtain these objects (entry conditions) for such activities
In other cases, individuals might be present, but not participate in care-related activities. These individuals, however, could distract others engaged in such processes. Technical communicators need to identify what those persons are doing, determine if such activities are distracting, and create materials to account for this factor (e.g., quick reference items individuals can scan to locate information quickly if distracted mid process).
Question 5: Once You’ve Completed This Process, What Do You Do Next? Can You Describe These Activities to Me?
Just because persons have completed a process does not mean the care related activity is done. Individuals might need to perform additional steps that could include recording readings, updating a physician, or re-considering the activities one should perform. These tasks are part of the overall care process and must be accounted for when creating materials for healthcare activities. For this reason, audience members need to describe next steps (post-healthcare activity) and note if information needs to be recorded or shared (exit condition), if sources should be consulted to plan future activities (props), and how materials (props) are put away once the process is done (exit conditions).
Creating Drafts and Testing Ideas
After collecting script and prototype data, technical communicators should review that information to identify patterns for the following expectations across participants:
Script elements (e.g., acts, scenes, entry conditions, roles, props, exit conditions) audiences associate with the context of care where a healthcare activity occurs Prototype characteristics for the context where the process occurs and the persons and items associated with that process
The objective is to create a checklist of features the audience uses to identify a context of care and perform a health-related activity there.
While experiences in a context of care will differ, technical communicators should identify more general trends for care expectations. Ideally, technical communicators will have the time and funding to map different scripts—and develop different materials—for the various audiences identified through this process. Pragmatically, technical communicators need to determine what factors are common across the greatest number of individuals to produce script and prototype maps for a relatively broad audience. The objective is to create
A design checklist of features audiences used to recognize the context where they perform a care-related process A sample depiction (e.g., a picture) of that context based on criteria in the checklist Design checklists for objects and persons associated with care activities in that context Sample depictions (e.g., pictures) of objects and persons based on those checklists
One cannot assume initial drafts effectively meet user expectations. Rather, they need to be tested with the intended audience.
Testing Draft Depictions
Testing draft depictions (e.g., sample designs) should involve interviews and focus groups to determine how effectively audiences recognize contexts, objects, people, and the care-related processes associated with such factors. Testing these draft depictions involves asking subjects questions as follows:
For depictions of contexts
Question 1: What is this place? Can you identify it? Question 2: What happens there? Question 3: When would you go there? Question 4: What would you expect to happen when you go there for X (care activity)? Question 5: This place is supposed to be an X (location) where you do Y (care activity): Would you modify this depiction to make it more recognizable as an X where you do Y?
The objective of this questioning is to determine if individuals recognize the context, the care activity that occurs there, and if initial depictions match audience expectations for a process.
For persons
Question 1: Who is this? How do you know? Question 2: What does this person do in this context? Question 3: What does this person use to perform this action (noted by individuals)? Can you describe that item? Question 4: What does this person do to perform this action? Can you describe this activity? Question 5: This person is supposed to be an X (kind of individual) who does Y (care activity) with Z (tool used to perform activity). Would you modify this depiction to make it more recognizable as an X who does Y? Would you modify the depiction of Z (object) to make it more recognizable as a Z that is used for Y?
The objective is to determine how subjects recognize the individuals who play a role in the care activity, what they do, and how well draft depictions (and associated design checklists) meet audience expectations.
Technical communicators should also determine if subjects recognize draft objects (in terms of prototype expectations) and the uses of these objects as related to a context of care.
For objects
Question 1: What is this item? How do you know? Question 2: What does this item do? How would you use this item in this context? Can you describe this process? Question 3: Where do you get this item? Where do you place it once the process is done? Question 4: What do you do after you’re done using this item? Do you write anything down or contact anyone to let them know of the results of this activity? If so, what do you write down or who do you contact and why? Question 5: This item is supposed to be an X (object) used to do Y (care activity). Would you modify this depiction to make it more recognizable as an X used to do Y?
Again, the objective is to assess how effectively draft depictions meet user expectations for a healthcare activity. Technical communicators would also need to note what tasks individuals perform once the process is complete (e.g., exit conditions for sharing information).
Technical communicators could use the answers to these testing questions in order determine if the initial design checklists and draft depictions for contexts, persons, and objects could be recognized and used by that audience to perform a healthcare activity. Audience feedback could also be used to modify checklists and create new depictions that better meet audience expectations for a context of care.
Technical communicators would use these questions to test the effectiveness of revised materials with new members of the same audience. Data would be collected and reviewed and modifications made depending on resulting feedback. Technical communicators would then test these newly revised items in a similar fashion to assess efficacy and collect comments. This process of revise and re-test would continue until designs effectively met audience expectations, or time and funding for the process ran out. Ideally, materials (maps, checklists, and depictions) resulting from this process would guide the development of care content and care technologies to create items audiences can readily recognize and effectively use in a context of care.
Testing Initial Models
If time and resources permit, one final stage step should occur before a product or content is released for general use. This step involves creating a physical model of the item based on the final map, checklist, and depictions resulting from iterative testing. Members of the intended audience would use this model in the actual context of care location to perform a task in that setting (e.g., “Use this draft manual for operating a digital blood pressure cuff to check your blood pressure in your kitchen.”). Technical communicators would observe and record what audience members do when performing the process and ask individuals to talk aloud during the process. Specifically, audience members should note
What they are doing Why they are doing it Anything that surprises them or they consider particularly effective—and why Anything that they find confusing or difficult to use or do—and why What suggestions they have to improve the process or enhance the design of the item
Technical communicators could use this feedback to determine if additional revisions are needed before releasing a product for greater public use. They could also use this feedback to revise such models and test them via a similar observational and talk-aloud process.
The objective of this process is to assess usability in the actual context of care, and technical communicators would need to
Bring audience members to the location where they perform the care activity (if done outside of one’s home) Meet individuals where they perform the activity (if in the home or if in another location)
This approach allows for the development of materials that better meet audience expectations for contexts of care.
Final Thoughts
Healthcare contexts are complex, and designing materials for them requires researching where individuals receive care. An understanding the psychology affecting how individuals use items in contexts can facilitate creating products for such environments. Cognitive concepts, such as scripts and prototypes, can be instrumental to these activities. The approach described here helps technical communicators determine factors audiences associate with healthcare practices. Such information can contribute to the development of healthcare materials audiences can use effectively.
Footnotes
Acknowledgments
The author wishes to thank the Eunice C. Williamson Endowment in Technical Communication for its support in the creation of this entry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.