
Abstract
Summary
Sixty-three patients presenting with subacute intestinal obstruction (SAIO) were studied. Thirty (47.6%) reported recurrent symptoms. Exaggerated bowel sound, visible/palpable bowel loops, distention of abdomen and abdominal lumps were observed in 60.3%, 28.5%, 25.3% and 19.0% patients, respectively. Thirty (47.6%) required emergency laparotomy. Investigations revealed lesions requiring surgery in 14 of 33 patients which were relieved with conservative treatment. The accuracy of ultrasonography, contrast enhanced computed tomography (CECT) scan and diagnostic laparoscopy was 57.1%, 100% and 100%, respectively. Ileum was the most common site of obstruction (79.5%). Adhesions and small intestinal strictures were the two most frequent cause of obstruction seen in 31.8% and 27.2%, respectively. Tuberculous pathology was demonstrated in 23 (52.2%). Previous abdominal surgery was found to be the only predictor of the success of conservative treatment (13/19 versus 7/44). All patients of SAIO, whose symptoms were relieved with conservative treatment, and who do not have history of abdominal surgery, should be subjected to CECTand/or diagnostic laparoscopy in order to discover the underlying cause of the obstruction. When these diagnostic modalities are not available, laparotomy is an effective alternative for this group of patients.
Introduction
Subacute intestinal obstruction (SAIO) implies incomplete, intermittent or recurrent obstruction.1,2 Patients often present with non-specific symptoms and ambiguous abdominal signs and the symptoms may ease spontaneously or after conservative treatment. These confounding features contribute to the delay in the diagnosis and patients may continue to suffer for weeks or months. Although the underlying cause may be identified in some patients subjected to diligent investigations, in cases of unresolved obstruction laparotomy will usually discover the aetiology in the majority. There is a lack of information on the various facets of SAIO such as the clinicopathological profile, role of investigations and management strategies. A PubMed search using ‘subacute intestinal obstruction’ [TI] OR ‘partial intestinal obstruction’ [TI] OR ‘incomplete intestinal obstruction’ [TI] as key words and ‘Human’ and ‘English’ as limits yielded 27 articles (searched on 12 August 2010) and most are case reports of single cases. This study has been undertaken in order to study patients presenting with the features of SAIO to elucidate the patient's profile, role of investigations in diagnosis, predictors for success of conservative treatment, cause of obstruction and underlying pathology.
Methods
All the patients presenting with features of intestinal obstruction to Surgery Unit I in a tertiary care teaching hospital in North India, were evaluated over a period of 16 months for possible inclusion in the study. Patients meeting the following criteria were included: continuation of the passage of flatus/faeces beyond 12 h of the onset of symptoms; a lesser degree of abdominal distension; gas distended bowel loops/multiple air-fluid levels on X-ray abdomen; and the allocation of conservative treatment in first instance. Those presenting with acute obstruction and/or features of strangulation, for which operative treatment was assigned on the first assessment, were excluded from the study. A thorough clinical assessment was performed and the investigation protocol included basic haematology, biochemistry and plain radiographs of abdomen. Conservative treatment for subacute intestinal obstruction was instituted. Those who were relieved of an obstruction, were followed up and subjected to special investigations – ultrasonography (USG), contrast enhanced computed tomography scan (CECT) and diagnostic laparoscopy (DL) – in sequential order according to the clinical necessity and feasibility. Patients in whom the obstruction was not relieved within 48 h of conservative treatment were considered for surgical exploration. Whenever DL demonstrated a lesion, it was tackled under the same anaesthesia either laparoscopically or through laparoscopy assisted laparotomy. All the patients were followed up for a minimum of 6 weeks.
The data was analysed in order to discover: the patient profile; role of investigations in diagnosis; predictors for success of conservative treatment; cause of obstruction; and underlying pathology. Statistical analysis was done using SPSS version 10.0 Statistical Packages for Windows (SPSS, Illinois, USA). Univariate analysis was carried out using the chi square test and Mann Whitney U test for continuous data. Binary logistic regression analysis was employed in order to determine the variables associated with the success of conservative treatment. All P values were considered significant at <0.05 (two-tailed).
Results
The study included 63 patients presenting with clinical features suggestive of SAIO. The mean age of the patients was 31.8 ± 16.6 years. There were 38 males (60.3%) and 25 females (39.6%). The duration of symptoms ranged from 1–365 days (median: 4 days). Thirty patients (47.6%) reported recurrent episodes of the symptoms (range 2–13 episodes; median: three episodes). Abdominal pain was reported by all the patients and it was colicky in nature in 55 (87.3%). Other symptoms reported were: vomiting (n = 51, 80.9%); constipation (n = 28, 44.4%); and distension of abdomen (n = 28, 44.4%). Twenty (31.7%) patients had a history of previous abdominal surgery. The reasons for previous abdominal surgery were available for 17 patients [abdominal trauma (7), intestinal perforation/obstruction (4), appendicectomy (1), gynaecological procedures (2), laparoscopic hernia repair (1) and laparoscopic tubal ligation (2)]. Eight patients (12.6%) had received anti-tubercular treatment (ATT) at other establishments in the past, of whom four received ATT following abdominal surgery [intestinal perforation/obstruction (2), details not available (2)]. Four other patients had been prescribed ATT empirically in view of recurrent abdominal pain. Exaggerated bowel sounds were the most frequent (n = 38, 60.3%) physical finding, followed by: visible/palpable bowel loops (n = 18, 28.5%); distension of abdomen (n = 16, 25.3%); an abdominal lump (n = 12, 19.0%); and tenderness (n = 5, 7.9%). Plain X-rays of the abdomen showed multiple air-fluid levels in 47 patients (74.6%).
Thirty (47.6%) patients underwent emergency laparotomy as they had not responded to conservative management after 48 h, developed features of strangulation or, on investigation during the initial episode, were seen to have lesions requiring surgery. Thirty-three (52.3%) patients were relieved of their obstruction: the time taken for the relief of symptoms following admission ranged from 1–4 days with an average of 2.3 days. Investigations revealed lesions requiring elective surgery in 14 of these patients. The investigative findings in the 14 who underwent surgery were correlated with operative findings. Two of the three specific diagnosis made by USG were confirmed during the operation. USG documented dilated bowel loops with hyper peristalsis in six patients and, on laparotomy, all revealed lesions requiring surgery. In five patients with surgically correctable lesions, USG was noncontributory. The overall accuracy of USG was 8/14 (57.1%). CECT identified the surgical lesion causing obstruction in 9/10 patients and demonstrated dilated bowel loops in one: the overall accuracy was 100%. DL was successful in identifying the obstructing lesion in 5/5 patients, resulting in 100% accuracy.
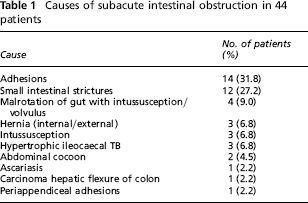
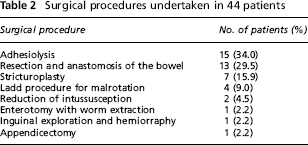
Forty-four (69.8%) patients underwent surgical treatment. The most common site of obstruction was ileum (35 patients; 79.5%). Adhesions, in 14 patients (31.8%), were the most common cause of obstruction, followed by small intestinal strictures in 12 (27.2%; Table 1). The other causes of obstruction were: malrotation of the gut with intussusception/volvulus; hernias (internal/external); intussusception; hypertrophic ileo-caecal tuberculous; abdominal cocoon; ascariasis; carcinoma colon; and periappendiceal adhesions. Adhesiolysis was the most frequently performed operative procedure followed by resection and anastomosis of the bowel and stricturoplasty (Table 2). Tuberculous pathology was demonstrated on a histopathological examination of the resected/biopsied tissue in 23 patients (52.2%) which were seen as: ileal strictures (n = 12); adhesions (n = 7); hypertrophic ileocaecal lesions (n = 3); and cocoon (n = 1).
Causes of subacute intestinal obstruction in 44 patients
Surgical procedures undertaken in 44 patients
Nineteen patients (30.1%) did not require surgical intervention. Of these, there was history of previous abdominal surgery in 13 patients. Four patients also had history previous anti-TB treatment. After a binary logistic regression analysis, previous abdominal surgery was found to be the only predictor for the success of conservative treatment (13/19 versus 7/44; P value = 0.000).
Two patients died on the second and fourth post-operative day, respectively. One patient died from adult respiratory distress syndrome and another succumbed to septicaemic shock. All patients were followed up for a period of 6 weeks to 14 months. A 12-year-old boy had a recurrence of symptoms 4 months after undergoing Ladd's procedure and operative reduction of the ileo-ileal intussusception for malrotation of gut with intussusception. He required re-laparotomy which revealed recurrent intussusception involving Meckel's diverticulum, missed during previous laparotomy, as a lead point. Two patients on ATT developed drug related complications (gastritis and hepatic encephalopathy, respectively) but responded to medical management.
Discussion
The diagnosis of SAIO is usually delayed and several patients continue to suffer from symptoms for weeks and months due to the waxing and waning nature of the disease. This study is unique in that it included only patients presenting with features of SAIO whereas most studies reported in the published literature refer to patients of acute intestinal obstruction or to a particular cause of intestinal obstruction, 3–6 The duration of symptoms ranged from 1 day to 365 days (median 4 days). Thirty (47.6%) of 63 patients had recurrent symptoms, with a median of three episodes per patient with a range from 1–13 episodes. These findings confirm prolonged suffering of these patients caused by non-diagnosis.
A total of 20 patients (31.7%) had a history of previous abdominal surgery. As noted in another study, 7 the majority of patients with small bowel obstruction had undergone previous abdominal surgery. Pain was a presenting complaint. Colicky abdominal pain (87.3%) and vomiting (80.9%) were more frequent than non-passage of faeces/flatus (44.4%) and distension of the abdomen (44.4%). The pain is usually intermittent and colicky in nature in small bowel obstruction. 7 A randomized controlled trial of over 1300 patients with acute abdominal pain in Finland indicated that the presence of previous surgery (relative risk 12.1) and the type of pain (colicky versus constant; relative risk 2.4) were the most predictive features in the diagnosis of acute small bowel obstruction. 8 In our study, the most frequent physical finding was the presence of exaggerated bowel sounds (60.3%). Seven (11.1%) patients had no abnormal physical finding. Distension of the abdomen has been described as one of the four cardinal features of intestinal obstruction and was also reported as the most consistent finding in acute small bowel obstruction. 8 However, in our study, distension was observed in less than half of the patients presenting with SAIO. The partial nature of obstruction and continued passage of flatus/faeces in patients with SAIO is the probable cause of this observation.
SAIO is a frequently used but ill-defined term. Based on the findings of our study, we propose to define its clinical characteristics. SAIO is generally caused by partial or intermittent obstruction of the small intestine or ileocecal region. The patient presents with intestinal colic/colicky central abdominal pain and vomiting. Varying degrees of abdominal distension and obstipation may be present. Increased bowel sounds are the most frequent physical sign. The presence of visible intestinal peristalsis or palpable bowel loops clinches the diagnosis. The symptoms may be relieved spontaneously or following conservative treatment, only to subsequently recur.
Conservative management led to relief of the obstruction in 33 (52.3%) patients and failed in 30 (47.6%). Previous studies have also shown failure rates of 27%–66% for conservative treatment.3,6,9–11 A history of abdominal surgery was found to be a statistically significant predictor of the success of conservative treatment. The time taken for the relief of symptoms following admission ranged from 1–4 days with an average of 2.3 days in these patients. Investigations revealed lesions requiring elective surgery in 14 of the 33 patients who obtained relieved with conservative management. The accuracy of ultrasonography, contrast enhanced CT scan and diagnostic laparoscopy in diagnosing SAIO in these patients was 57.1% (8/14), 100% (10/10) and 100% (5/5), respectively. The findings suggest that patients who are relieved of SAIO should be subjected to systematic investigations if recurrence and prolonged suffering is to be avoided. A CECT scan is an effective and non-invasive diagnostic tool for SAIO but a lack of availability and affordability restrict its use in developing countries. 12 DL is highly effective in diagnosing bowel obstruction and its underlying cause.13,14 It is an invasive investigation but does provide scope for simultaneous therapeutic intervention.
Overall surgical intervention was required in 44 patients (69.8%). In a study of 348 patients of intestinal obstruction, Bhansali et al. 15 also reported 67% patients undergoing surgery for intestinal obstruction. It is interesting to note that 14 of the 20 patients, who were relieved of their symptoms and had not had prior abdominal surgery, ultimately required laparotomy. In our study, the two most common causes of SAIO were adhesions (n = 14, 31.8%) and small intestinal strictures (n = 12, 27.2%). Various studies have demonstrated that adhesion is an important cause of surgically managed small bowel obstruction which seen in 45%–80% of patients.9,11,16–18 TB was the most frequent underlying pathology seen in 23/44 (52.2%) patients operated for SAIO. It is noteworthy that more tubercular lesions manifested as ileal strictures (12/23, 52.2%) than as hypertrophic ileo-caecal TB (3/23, 13.0%) in our series. Two patients who were diagnosed to have malrotation of gut had previously received a full course of ATT for abdominal symptoms elsewhere on an empirical basis. Empirical ATT for abdominal symptoms is still in vogue in this part of the world. All attempts should be made to confirm the diagnosis of TB before prescribing ATT. Laparoscopy is an effective tool for demonstrating typical tuberculous lesions and provides an opportunity to retrieve tissue for histopathological examination.
Conclusion
Our study shows that conservative management is successful in about half of patients presenting with SAIO, particularly in those with a history of abdominal surgery. All those with SAIO, who are relieved of symptoms with conservative treatment and do not have a prior history of abdominal surgery, should be subjected to CECT of the abdomen and/or diagnostic laparoscopy in order to identify the possible cause of an obstruction. In the absence of these diagnostic modalities, especially in under developed countries, laparotomy is the logical next step for this group of patients which can lead to the identification of the underlying cause and, therefore, to corrective surgery.