
Abstract
We present a case of pulmonary cryptococcosis presenting as wandering multiple bilateral shadows and hilar and mediastinal lymph node enlargement in which the fluconazole treatment suppressed the symptoms. This case illustrates the complex nature of immunological responses in the lungs and highlights the need to consider the existence of cryptococcal allergies.
Introduction
The incidence of pulmonary cryptococcosis (PC) has increased in recent years, especially in patients with normal immunity. Radiological findings are varied, non-specific and are influenced by the underlying immune status of the patient. Diagnosis should always be based on the isolation of cryptococcus from a pulmonary specimen or on the detection of cryptococcal antigens, coupled with the appropriate clinical, radiological and histopathology findings. We had observed an immunocompetent patient with wandering multiple bilateral pulmonary shadows for 3 years, exhibiting numerous instances of cough and low fever symptoms and CTs showing enlargement of the hilar lymph nodes. The final diagnosis was cryptococcus pneumonia. After 1 month of luconazole therapy the pulmonary lesions and symptoms had decreased.
Case report
A 31-year-old man had been diagnosed 38 months earlier with multiple bilateral pulmonary shadow lesions, which can subside even without treatment (Figure 1). He denied exposure to pigeons, pets, flowers and dust. However, his father was a fruit peddler. The patient had a history of hypertension but had not received any immunosuppressive therapy. His total lymphocyte count, specifically CD4 and CD8 counts and CD4/CD8 ratio, was normal.
(a) Computed tomography (CT) scan showing a lung prompting multiple pulmonary cavity; (b) CT scan taken 2 years later showed a lung promoting cavity. Although the patient was not given the anti-infection treatment, the lesions had disappeared.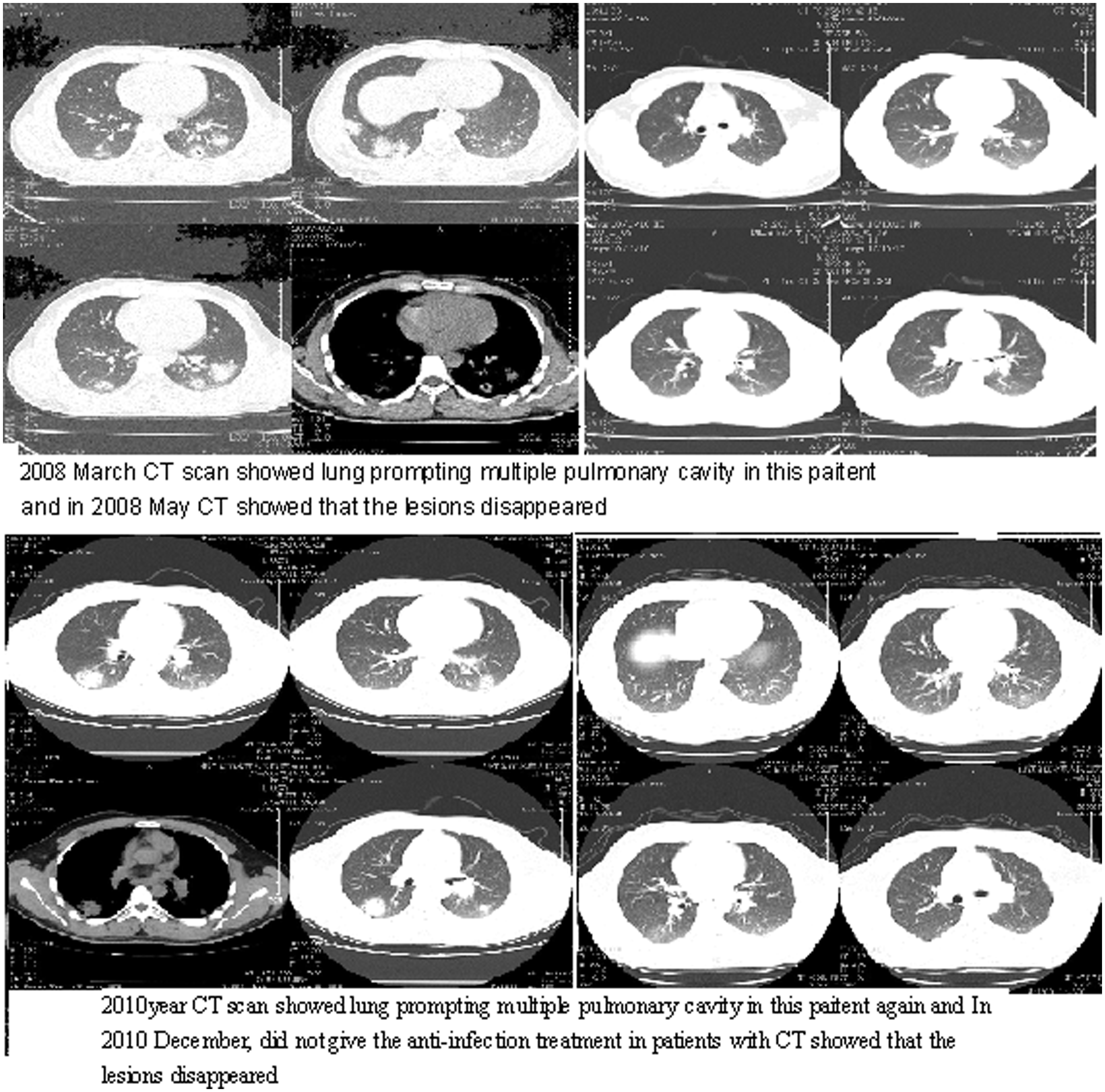
In 2011, the patient reported a fever of 38℃ and 4 weeks of persistent coughing and sputum. A computed tomography (CT) scan showed enlarged pulmonary cystic lesions and hilar and mediastinal lymph node enlargement (Figure 2).
(a) Computed tomography (CT) scan showing multiple pulmonary shadows and hilar and mediastinal lung node enlargement; (b) Grocoti’s methenamine silver staining (+) and haematoxylin-eosin staining (+) (400 x).
An assessment of the patient’s respiratory condition showed: a body temperature of 37.6℃; blood pressure of 130/100 mm Hg; heart rate of 77 beats/min; respiratory rate of 18 breaths/min; and room air oxygen saturation at 100%. He also exhibited non-fluent speech and had no lip cyanosis. His cervical region was soft and trachea in his middle and the jugular vein were not engorged. The superficial lymph node was non-palpable. The bilateral tactile fremitus was normal and the wet and the dry rales were obvious. Results of the neurological, cardiac, abdominal and skin examination were all normal and he displayed no masses or organomegaly.
Basic laboratory studies revealed a white blood cell count of 12.5 × 10e9 cells/L, with a differential of 5.2 × 10e9/L neutrophils, 6.2 × 10e9/L lymphocyte and 0.1 × 10e9/L eosinophils. Chemistry studies revealed normal electrolytes, liver function and thyroid function. C-reactive proteins indicated a mass concentration of 99.10 mg/L. The enzyme immunoassays were negative for HIV. Sputum cultures of normal flora exhibited no fungal growth. Urine, stool and tumour markers and immunoglobulins (Ig), including IgG subclasses, were normal. Abdominal B ultrasound, fatty liver (heterogeneous) image and electrocardiogram (ECG) were also normal.
We therefore considered the possible existence of fungal infection in this patient. A lung biopsy was performed in order to obtain the tissue for Grocoti’s methenamine silver (GMS) staining (+) (Figure 2). The GMS stain was strongly positive and haematoxylin-eosin (+) (Figure 2) and periodic acid Schiff (+) stains displayed the same results. A cerebrospinal fluid India ink smear did not reveal cryptococcosis. Thus, the final diagnosis was primary PC.
The patient was given 400 mg fluconazole daily. A follow-up CT scan a month later revealed the disappearance of the shadows. He then became asymptomatic and experienced no further seizures.
Discussion
Cryptococcosis is a severe fungal infection disease that generally develops in immunosuppressed individuals. PC is generally caused by Cryptococcus neoformans infection. 1 C. neoformans in yeast can be isolated from the natural soil, pigeon dung, fruit, milk and from humans with normal immunity. The organism enters via the respiratory tract and causes a spectrum of illnesses ranging from asymptomatic infection to severe diseases. 2 PC is always expressed as sub-acute or chronic lung mycosis and is self-limited. Symptomatic PC patients can present symptoms of infection, such as fever, cough, chest pain, weight loss and purulent sputum and about 50% are immunocompetent. 3
Laboratory examination of cryptococcus involves: analysis of sputum, pleural fluid and cerebrospinal fluid for ink smear or culture and fixation reactions; white blood cell count for a mild or moderate increase of neutrophil and, in advanced cases, there may be anaemia; X-ray, CT or a lobectomy. Infiltration of any type, nodular or leakage, can occur which is more common in the bilateral middle and lower lung that can be unilateral or confined to one lobe, with large spherical isolated lesions or multiple nodules. There may be a diffuse miliary shadow or patchy infiltrates and about 10% of patients have cavity formation. Enlargement of the hilar lymph nodes are extremely rare. 4
We speculated that, in our patient, other factors might be involved in the cryptococcus pathogenicity in the lung tissue. The pneumonia could have been related to allergic alveolitis but we eventually diagnosed him as suffering from cryptococcus pneumonia.
Treatment of new cryptococcosis depends on the site of infection and on the immune status of the host. PC in immune-normal hosts requires strict observation. For symptomatic cases, treatment with fluconazole (200 mg/day to 400 mg/day) for 3 to 6 months is recommended.
Conclusion
Tests for migratory pneumonia or allergic alveolitis are extremely rare. This case underlines the complex nature of immunological responses in the lung and highlights the importance of considering the possible existence of cryptococcal allergies.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.