
Abstract
We describe a possible imported case of osteo-articular coccidioidomycosis in India. Culture of the computed tomography-guided aspirate revealed the growth of Coccidioides spp., which was identified as Coccidioides posadasii by sequencing of the internal transcribed spacer (ITS) region of rDNA. He was successfully treated with amphotericin B followed by itraconazole. All the previous published reports of coccidioidomycosis cases diagnosed in India are also reviewed in order to increase the awareness of this disease in non-endemic areas.
Introduction
Coccidioidomycosis is a geographically restricted disease prevalent in western USA and certain areas of Central and South America. The disease is caused by Coccidioides immitis and C. posadasii, two genetically distinct but morphologically identical species of soil fungus.1,2 In the USA C. immitis is restricted to southern California and C. posadasii to the east and south Sierra Nevada range.1,2 No autochthonous case of coccidioidomycosis has been reported from India. Only five imported cases of coccidioidomycosis have been reported.3–7 Our case is the sixth in the series and was diagnosed late due to a lack of awareness of this disease. We review all reported cases from India.
Case report
A 31-year-old man from Delhi, a software engineer by profession, presented in Safdurjung Hospital, New Delhi, India, in January 2012 with fever, joint pain in the right wrist and ankle, and a small abscess in the vicinity of right elbow. The illness started insidiously 6 months after he had returned to India from Phoenix, Arizona, USA in June 2004. He stayed in Phoenix from March 2004 through May 2004. Initially, he had a high fever, malaise and flu-like symptoms and was admitted to a private hospital in Dehradoon, Uttarakhand, India in November 2004. He was prescribed antibacterials and a partial response was seen.
In August 2005, he complained of low grade fever, pain and swelling of elbow, forearm, wrist and ankle in the right side which did not respond to pain killers. He had also nodular swelling on the chest wall. He consulted a private orthopaedic surgeon in Gurgaon, Haryana (Delhi NCR), India. A laboratory investigation revealed an increased total leukocyte count (12,000 cells/mL); eosinophilia; raised erythrocyte sedimentation rate (85 mm/h); positive Monteux 14 × 15 mm in size; and positive C-reactive protein. Chest imaging was within the normal limits. A posterior–anterior image of the right wrist revealed erosion at the distal right end of the ulna. Similarly, erosive changes were detected in the right talus of his ankle joint and the upper end of his right ulna. The excision biopsy of the chest nodule was reported as being epitheliomatous hyperplasia with satellite neutrophilic abscesses and occasional presence of giant foreign body cells. The culture of the biopsy specimen was negative for bacteria, including Mycobacterium and fungi. A computed tomography (CT)-guided fine needle aspiration (FNA) cytology of the eroded right ulnar head revealed focal granulomatous inflammation. However, as tubercular joint involvement was suspected, he was put on anti-tubercular therapy for 18 months, but his clinical condition failed to improve. In January 2008, the culture from the drained pus from his right ankle was negative for bacteria, including Mycobacterium and fungi. In July 2008, the patient was sent to another orthopaedic surgeon, as there was a further deterioration of his clinical condition. Suspecting atypical or drug resistant Mycobacterium infection, he was put on second line anti-tubercular therapy with a combination of levofloxacin and cycloserine.
In December 2011, he sought advice from the Department of Orthopaedics at Saint Stephan Hospital, Delhi as, by that time, he had lost 80% elbow joint mobility and had difficulty in walking. An examination revealed a painful elbow with an abscess, plus restricted movement of the right wrist and ankle joints with localized swelling and abscess. The CT imaging of his right elbow revealed erosion at the proximal end of the ulna on the upper end of the radius (Figure 1). An FNA sample for the right ulnar head was sent for microbiological investigation and revealed ill-defined lucent areas on the medial aspect of the talus.
The CT imaging of the right elbow demonstrated eroded proximal end of ulna on the upper end of the radius.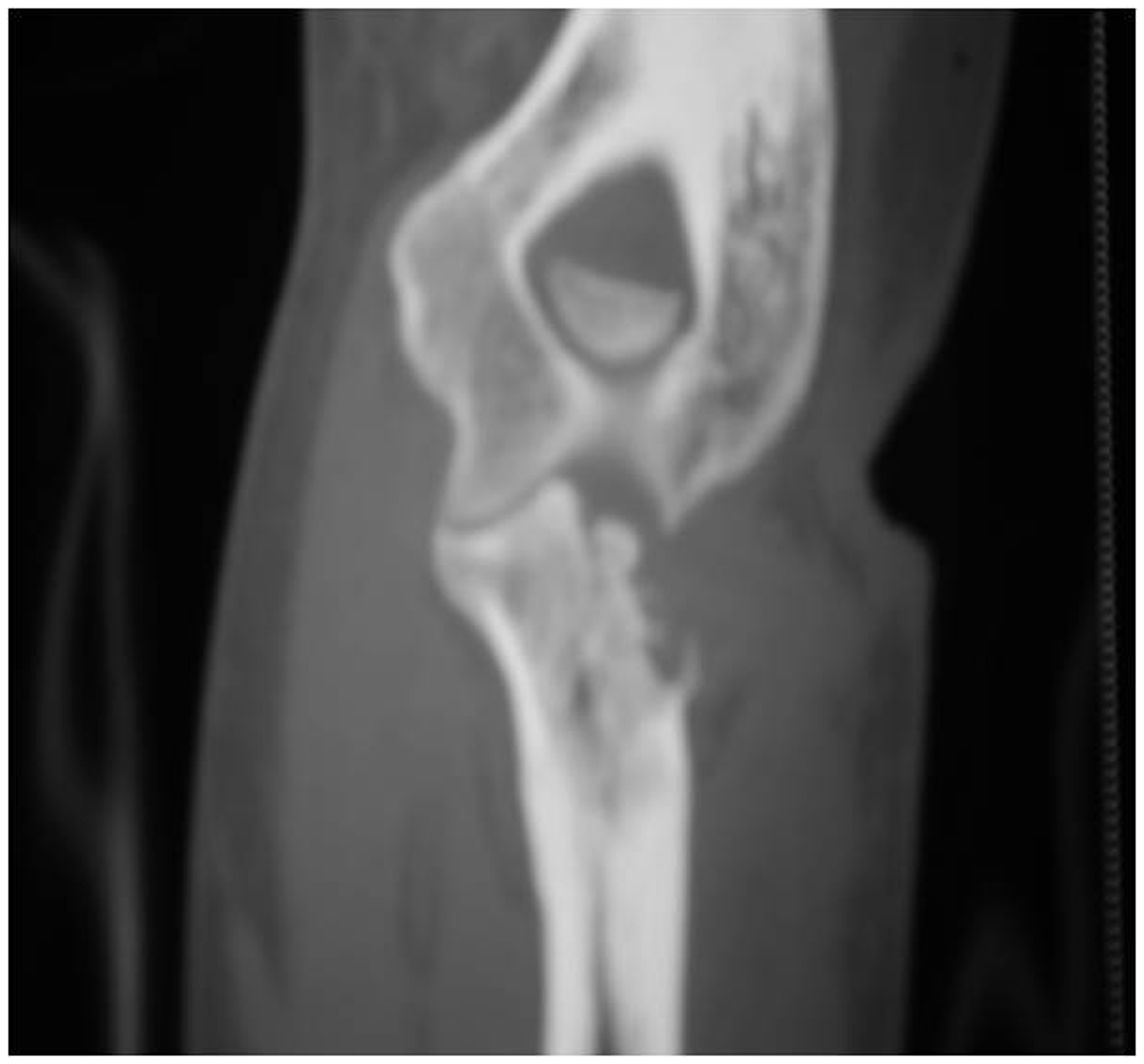
The direct microscopy of periodic acid Schiff stained FNA samples from the right ulnar head revealed spherules with multiple endospores (Figure 2). Greyish off-white fluffy colonies were observed on yeast phosphate agar at 25℃ after 5 days' incubation. Lactophenol cotton blue mount of the growth revealed hyaline hyphae fragmenting into barrel-shaped arthroconidia with alternate disjunctor cells morphologically resembling C. immitis. The isolate was sent to the Postgraduate Institute of Medical Education and Research, Chandigarh, India, for molecular confirmation. Amplification of the entire ITS region (ITS-1, 5.8 S rRNA, ITS-2 of rRNA) was done by polymer chain reaction (PCR). A National Centre for Biotechnology Information (NCBI) Bsic Local Alignment Search (BLAST) of the sequence showed a 99% identity with C. posadasii. A complement fixation test (CFT) for coccidioidomycosis was performed (Focus Diagnostics, CA, USA), and revealed a positive titre of 1:32.
Periodic acid-Schiff stained fine-needle aspirated sample from right ulnar head revealed spherules with multiple endospores (450X).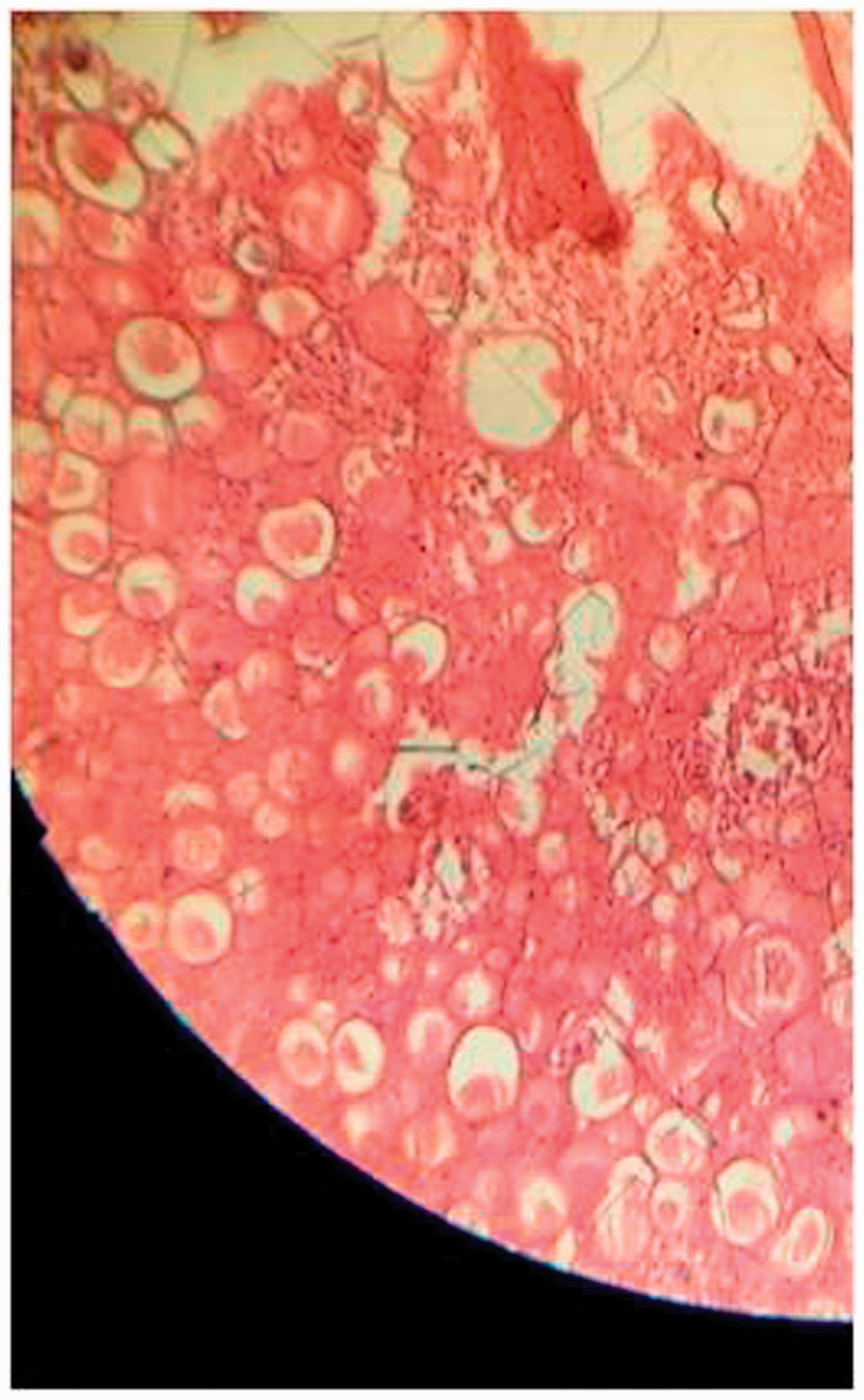
The patient was treated with intravenous amphotericin B deoxycholate (50 mg/day) for 20 days followed by oral itraconazole (400 mg/day). He was successfully treated after 1 year of antifungal therapy.
Discussion
With the ease of global travel, imported cases of coccidioidomycosis have been reported in travellers from Europe, Canada and Asian countries including India.3–7 Our patient, a resident of Delhi, India, had a history of travel to Phoenix (Arizona) and Nevada. He was immunocompetent and possibly acquired the infection during his travels. Unfortunately, his diagnosis was delayed and he was treated with several courses of anti-tubercular therapy. Coccidioidomycosis masquerades clinically and radiologically as TB. Furthermore, the histological lesion of both diseases present as granuloma formation. The similarity of both diseases and the rarity of coccidioidomycosis in India misled earlier doctors. Finally, the observation of spherules (30–40 µm) with endoconidia helped in the diagnosis of coccidioidomycosis.8,9 In this case, the infection progressed to disseminated disease due to the delayed diagnosis, although he was immunocompetent. The disseminated disease in endemic areas is observed in immunocompromised individuals, including patients suffering from malignancy; HIV infection; transplant patients; pregnant women; and those facing heavy exposure such as archaeologists, construction workers and agricultural workers. Certain ethnic groups, that is, patients of Afro-American and Asian origin with blood group B, are at high risk of suffering from disseminated disease. 8
Demographic, clinico-mycological, therapeutic profile of the authentic cases from India.
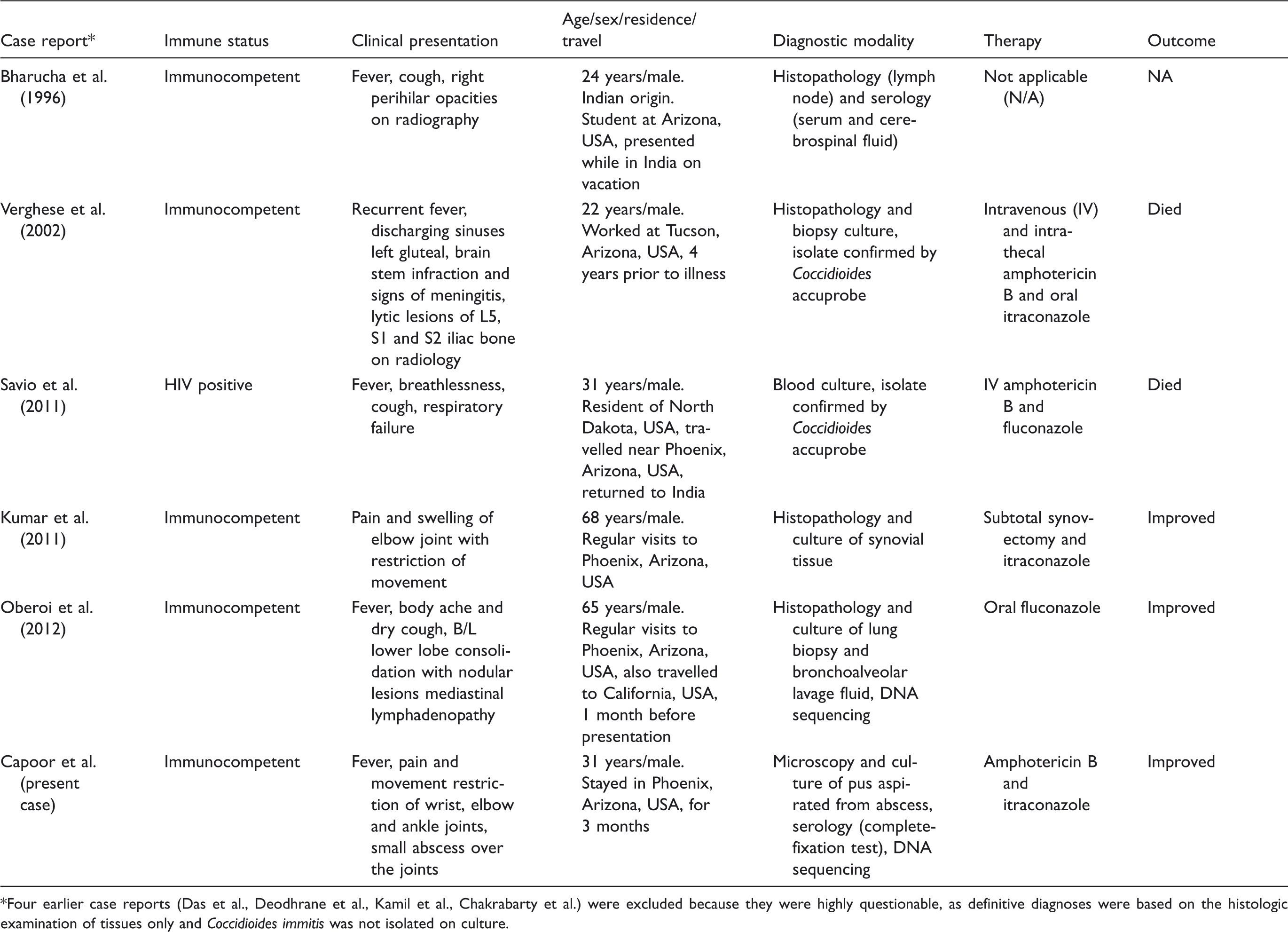
Four earlier case reports (Das et al., Deodhrane et al., Kamil et al., Chakrabarty et al.) were excluded because they were highly questionable, as definitive diagnoses were based on the histologic examination of tissues only and Coccidioides immitis was not isolated on culture.
Conclusion
The present case highlights the fact that the increased frequency of international travel of Indian citizens has resulted in an increase of the number of cases of imported coccidioidomycosis in India. A high index of clinical suspicion by clinicians and microbiologists is therefore required when treating patients who have recently returned from visits to endemic regions.