
Abstract
An accessory penis is a very rare anomaly. Only five cases have been reported thus far to our knowledge. We present the case of a child aged 2 years and 10 months who had a penis-like structure (containing phallus and glans) attached to the right buttock. Associated anomalies were a non-communicating type of colonic duplication, a paramedian stenosed anal opening, a horse-shoe kidney, posterior urethral valves, scoliosis of the lumbo-sacral spine, polydactyly and equino-varus deformity of the right foot. As far as we can tell, this is the first report of an accessory penis associated with colonic duplication and other congenital anomalies.
Introduction
Human gluteal appendages have been reported very rarely. Only five cases of appendages resembling a penis grossly and histologically have been discovered in the literature. We present the first case of a child with an appendage resembling a penis attached to the buttock, and associated with multiple congenital anomalies involving the gastrointestinal, genitourinary and skeletal systems.
Clinical report
The child presented at the age of 2 years and 10 months with complaints of loose motion and abdominal distension for the last 3 days. On further questioning it was found that the child had similar complaints at the age of 8 months but managed to pass a constipated stool every second or third day normally.
On examination, the most striking feature was a soft tubular structure which looked exactly like a penis, attached to the right buttock. This was non-tender, muscular in consistency, and transversely placed with its base at the lateral aspect of buttock and its apex having a glans directed medially (Figure 1). This structure was present at birth, but never elicited a fluid discharge. The child was born at a health centre by normal vaginal delivery at a birth weight of 2.9 kg. Motor milestones were delayed; the child started walking without support at 2 years with a limp towards the right. Developmental milestones were otherwise normal.
Accessory penis over buttock along with a normal genitalia.
Apart from the accessory penis, normal genitalia were noted. An anal opening was located to the left of the midline and appeared stenosed, explaining the child’s intermittent constipation. Abdominal and chest examination were normal. No organomegaly was found. Tone, power and reflexes (both superficial and deep) of the trunk and limbs were normal. All the cranial nerves were normal with a normal fundus. Nodysmorphic facial features or neurocutaneous stigmata were noted. The skull was normal in size and shape. Gross scoliosis of dorso-lumbar spine was noted with a convexity towards right. The upper limbs were normal, but, the right foot had an equino-varus deformity associated with six toes, the first two being fused. The child was observed walking on the lateral three toes of his right foot, limping towards the right. The left leg was normal.
Investigations revealed a loss of normal lordosis of the lumbar spine and scoliosis of the dorso-lumbar spine with convexity towards the right. Vertebral height, marrow signal intensity and alignment, however, appeared normal. Junctional vertebra were seen at the lumbosacral junction with reduced L5–S1 joint space suggestive of bilateral partial sacralisation. The tubular structure at the buttock consisted of regular penile anatomy with two corpora cavernosum and one corpora spongiosum in between. Ultrasonography (USG) abdomen and intravenous pyelogrpahy (IVP) was suggestive of fused renal ectopia, and the presence of non-communicating duplicated hindgut loops in the right of the abdomen (Figure 2). Dilatation of the posterior urethra near the base of the bladder with faint Y-shaped lucent line was demonstrated suggestive of posterior urethral valves. No vesico-ureteral reflux was observed. There was a low anorectal malformation associated.
Contrast-enhanced abdominal computed tomography showing presence of non-communicating type of colonic duplication.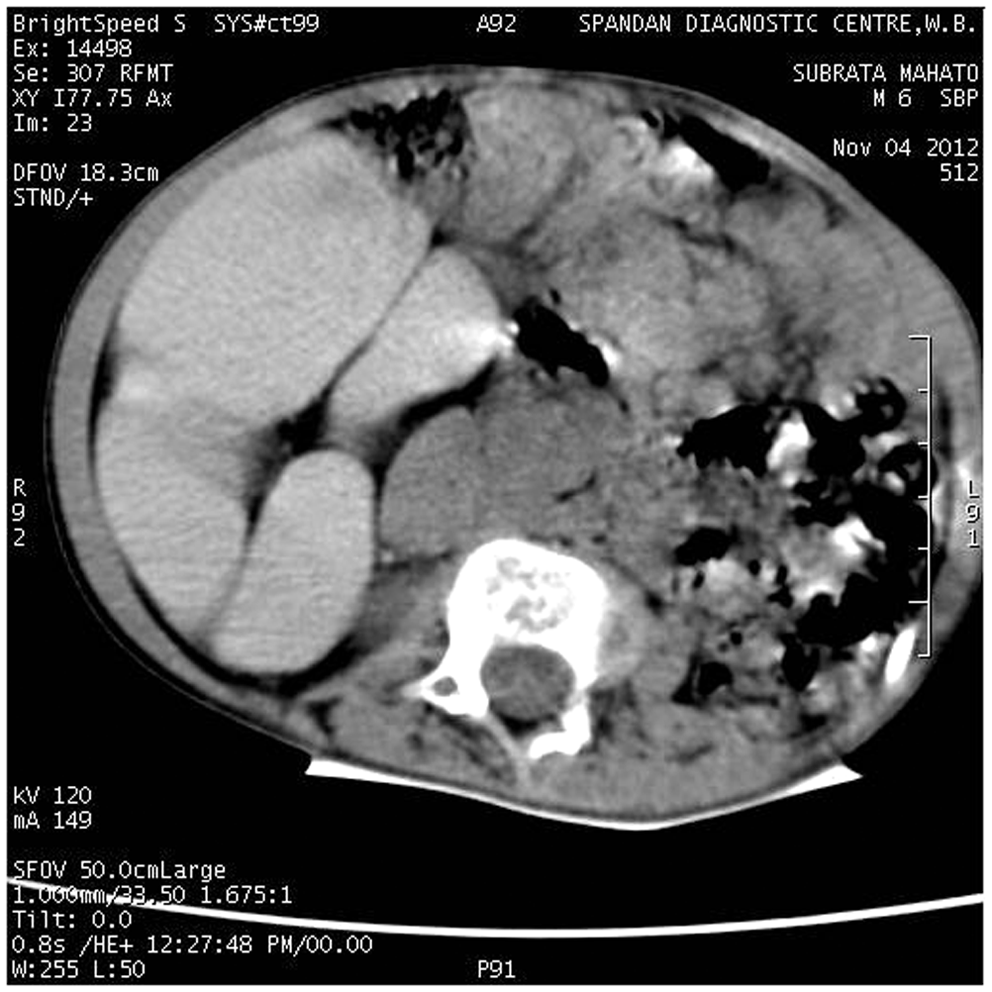
The child underwent an exploratory laparotomy with excision of the non-communicating colonic duplication and dilatation of the stenosed ectopic anus was performed. Unfortunately the parent of the child objected to excision of the accessory penis, and hence no histology of this organ was available.
Discussion
The appearance of ectopic genital tissue is a very rare event. Davies 1 described a case of quadruple peniform structure associated with a dermoid of the perineum. Another case of a sacral appendage resembling a penis but without urethra has been reported in association with sacral fourth and fifth hemivertebrae and only one coccygeal vertebra. 2 Two case reports from India reported the presence of an accessory penis over a mass comprising of a teratoma and/or lipomyelomeningocele associated with spinal anomaly.3,4 Another report described the presence of a thoracolumbar accessory penis which had a lipomatous connection to the epidural space. 5
The correct embryological explanation of this rare deformity is not clear. Historically, most authorities have classified similar malformations as either teratomas or as parts of a fetus in fetu. The lesion described here had many of the features of a well-differentiated teratoma, but the differentiation into a phallus-like structure does not completely fit the definition of teratoma. 6 The possibility of fetus in fetu must also be considered. This term represents the presence of a parasitic twin within its partner. 7 Strict criteria for this entity usually require part or the whole of the vertebral axial skeleton to exist coincidentally.
The morphogenesis of our case is not clear. Spemman 8 was the first to postulate that the influence of a ‘primary organiser’ determined the orderly growth of fetal tissue. Willis 6 takes the view that teratomas arise from foci of multipotential embryonic tissue that, for some unknown reason, have escaped this influence. Other investigators have proposed that mechanical and/or local environmental factors may affect the degree of differentiation. In fact, this theory has been used to explain an accessory scrotum with a rudimentary phallus and accessory limb. 9 The possibility then exists that under the influence of local androgens, these pluripotential cells may mature along the lines of an accessory penis with mature erectile tissue. In summary, although speculations about an aborted attempt at twinning cannot be completely dismissed, this lesion can best be seen as a highly differentiated teratoma in an unusual anatomic location. 5
In our case, the accessory penis was associated with multiple congenital anomalies viz non-communicating type of colonic duplication, paramedian stenosed anal opening, horse-shoe kidney, posterior urethral valves, scoliosis of the lumbosacral spine and polydactyly with equino-varus deformity of the right foot. Colonic duplication itself is a very rare congenital anomaly. 10 Some early aberration in the formation of the primitive hindgut is hypothesised to cause a split or twinning process of the developing embryo, resulting in duplication of the terminal gut. 11 However, the entire congenital anomaly present in this child could not be explained by any of these hypotheses. As per our knowledge and literature search, though association of diaphallus and colonic (or hindgut) duplication has been previously reported, this is the first case reported where accessory penis was associated with colonic duplication and genitourinary and skeletal malformation.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.