
Abstract
We studied the practice of malaria prevention and treatment in pregnancy of 394 private medical practitioners in Lagos State, Nigeria using a self-administered pre-tested structured questionnaire.
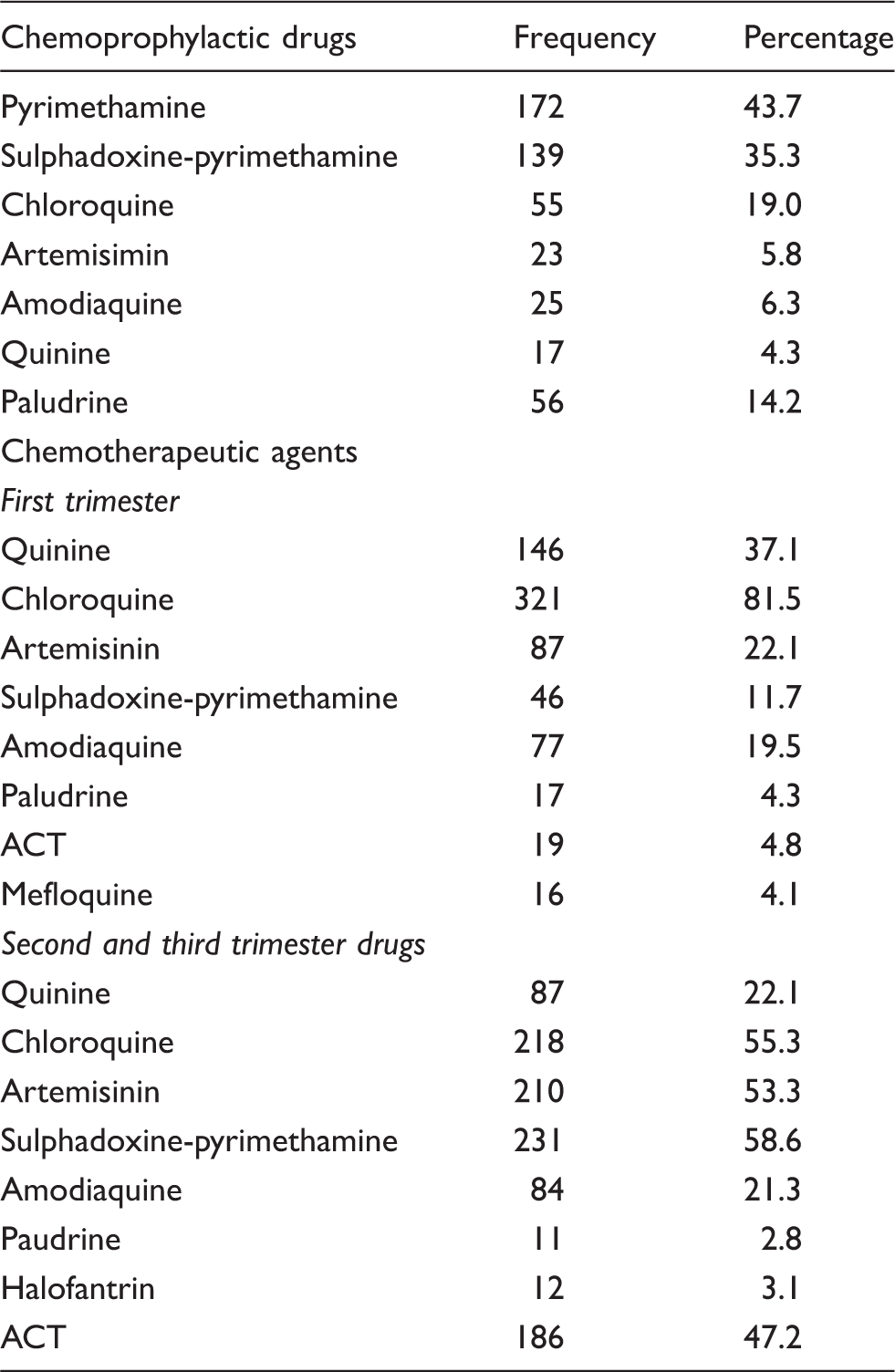
Only 39 (9.9%) respondents had correct knowledge of the World Health Organization (WHO) strategies. Malaria prophylaxis in pregnancy was offered by 336 (85.3%), but only 98 (24.9%) had correct knowledge of recommended chemoprophylaxis. Of these, 68 (17.3%) had correct knowledge of first trimester treatment, while only 41 (10.4%) had knowledge of second and third trimester treatment. Only 64 (16.2%) of respondents routinely recommended use of insecticide-treated bed nets. The most common anti-malarial drug prescribed for chemoprophylaxis was pyrimethamine (43.7%); chloroquine was the most common anti-malarial prescribed for both first trimester treatment (81.5%) and second and third trimester treatment (55.3%). The study showed that private medical practitioners have poor knowledge of malaria prophylaxis and treatment in pregnancy, and the practice of most do not conform to recommended guidelines.
Introduction
Malaria infection is a major public health problem in sub-Saharan Africa where 90% of malaria cases are found and where much morbidity and mortality occur among pregnant women and children. 1
The principal impact of malaria is associated with malaria-related anaemia, which, when severe, increases the risk of maternal mortality. 2 Spontaneous miscarriage, low birth weight, preterm delivery, intrauterine growth retardation, congenital infection and neonatal mortality are linked to malaria in pregnancy.2–4
These adverse effects for both mother and fetus together with data suggesting an increase in multiple drug resistance has made it necessary to look critically at the issue.5–7 The Nigerian Antimalarial Guidelines and Treatment Policy currently recommend a three-pronged approach; viz, intermittent preventive treatment (IPT) of asymptomatic pregnant women with sulphadoxine-pyrimethamine (SP), use of insecticide-treated bed nets (ITNs), and prompt and effective febrile case management of malaria. 8
Despite these well established guidelines, the frustration in countries with high rates of malaria has been the poor uptake and utilization of the recommended interventions. 9 Some of the reasons adduced for this is their lack of proper integration in antenatal care offered in private institutions. Private hospitals play a key role in the delivery of maternal and child health services in Lagos, but unfortunately they appear to have limited access to new information. This may be because most health programmes are targeted at big research and health institutions. 9 In Nigeria, patients are known to prefer private hospitals because of their short waiting time, friendly attitude of the health workers, and privacy and proximity of the facilities to their homes.10,11 Indeed, a recent survey in Abia State, south-eastern Nigeria reported that 79% of antenatal care and delivery occur in private hospitals and clinics. 12
Many studies evaluating reasons for the apparent poor implementation of malaria control strategies in pregnancy have been conducted in this country. However, most of these studies have focused on pregnant women themselves,13–17 rather than healthcare providers. Against this background, this study was conducted to evaluate the practice of malaria prevention and treatment among private medical practitioners (PMPs).
Materials and methods
Study area
The study was carried out in Lagos State, Nigeria, with an estimated population of 17.5–21 million. It has 20 local government areas (LGAs) out of which 16 comprise the statistical area of Metropolitan Lagos. Thirteen of these have population densities over 5000/km2. The state has two teaching hospitals and one of the nation’s three orthopaedic hospitals and a federal medical centre.
In each of the 16 metropolitan LGAs, there are a general hospital and at least three government health centres. There are numerous private hospitals in the State and these are mainly located in the more densely populated parts.
Design
This study is a descriptive cross-sectional survey.
Study population and sampling technique
We selected two high-density and two low-density LGAs by random. The list and addresses of all the private hospitals in each of the chosen LGAs were obtained from official registers. It was assumed that 50% complied with the recommended guidelines. A minimum sample size of at least 400 was projected. a
Data collection
A pre-tested structured questionnaire based on adaptations and literature review on the subject was used. The questionnaire was in three parts: soliciting the characteristics of the respondents; their practice of malaria prophylaxis; and its treatment during pregnancy.
The authors and volunteers who had been carefully briefed about the study visited the selected hospitals until the desired number of respondents for the study was achieved. The purpose of the study was explained to the private practitioners in the hospitals and those who gave their consent were given the questionnaire to study and complete. The self-administered questionnaires were retrieved after a maximum of 1 week. The data were collected over a period of 4 months.
Data processing and analysis
The authors appraised the questionnaires and categorised open-ended questions and answers, deciding whether the responses conformed to the recommended national policy. b
Ethical consideration
Approval for the study was obtained from the Research Ethics Committee of the Lagos State University Teaching Hospital. Only doctors who gave their consent after the purpose of the study had been explained to them participated in the study.
Results
A total of 430 private medical practitioners in two high-density and two low-density LGAs responded, but data were complete in 394 (91.6%) respondents.
The age of these respondents was in the range of 25–64 years with a mean age of 37.98 ± 9.16 years. The respondents had practised medicine for a mean of 10.83 ± 9.31 years (range, 1–34 years). Of the practitioners, 322 (81.7%) were private general practitioners (PGPs), while 72 (18.3%) were specialists in various fields of medicine. The greatest percentage (38.8%) of specialists, were obstetricians and gynaecologists. Other specialists who offered antenatal services were community health physicians (16.7%), internal medicine physicians (16.7%), paediatricians (5.6%), radiologists (9.7%) and surgeons (12.5%).
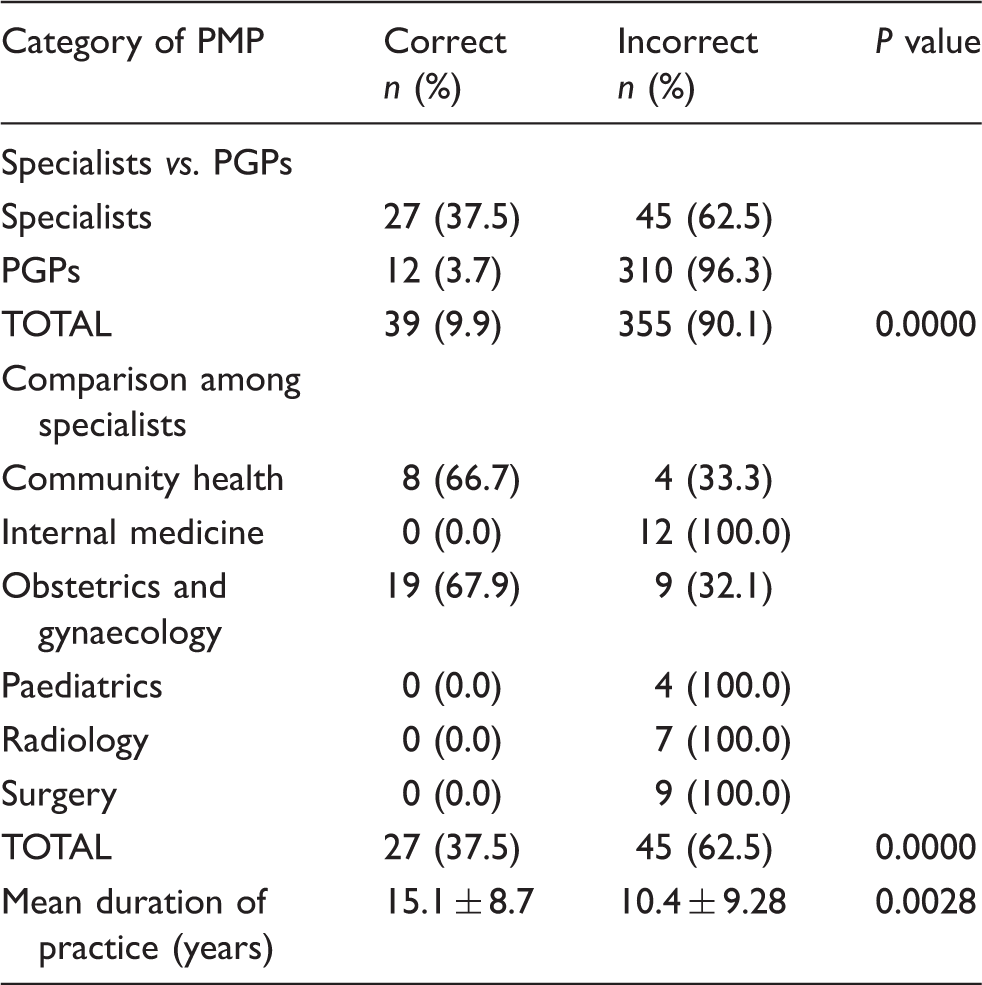
Knowledge of the strategies for malaria control in pregnancy.
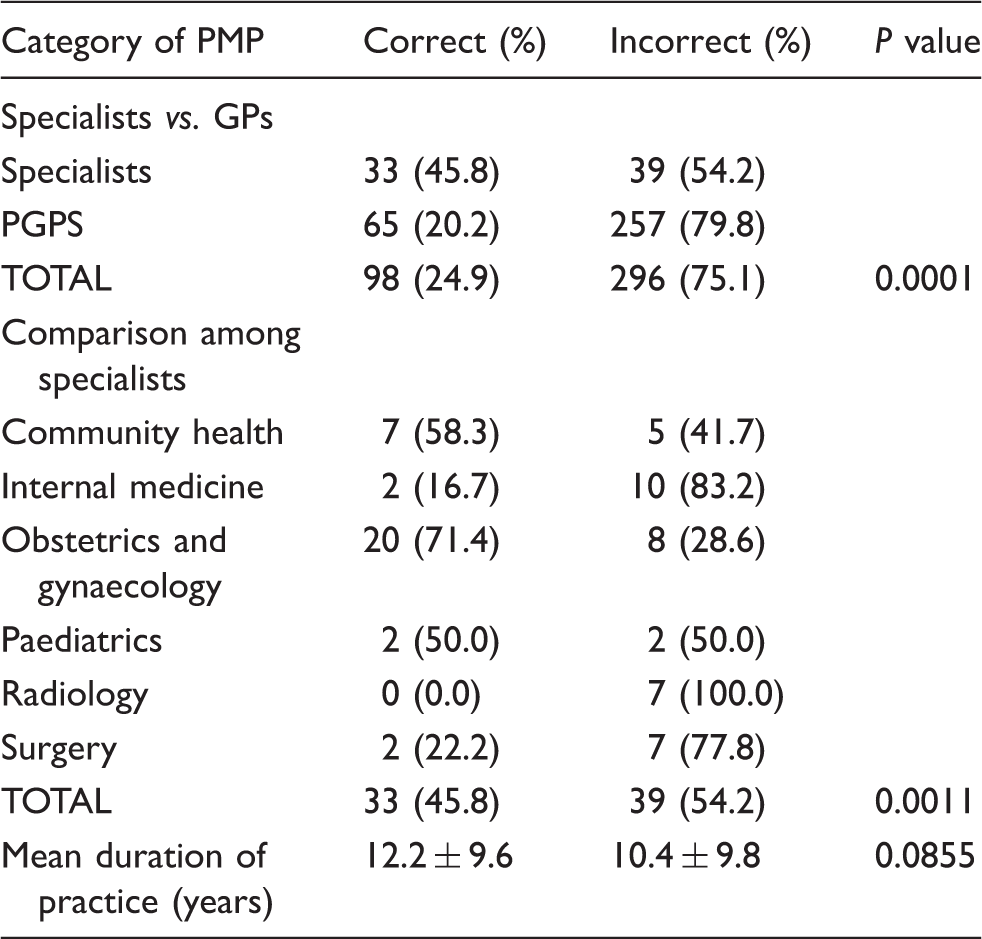
Knowledge of chemoprophylaxis among private medical practitioners.
Knowledge of malaria treatment in pregnancy.

Even less, only 10.4% of all the respondents had correct knowledge of second and third trimester treatment. Nineteen (26.4%) specialists had correct knowledge compared to 22 (6.8%) PGPs (P = 0.0000). Fifty percent of obstetricians and 33.3% of community health specialists had correct knowledge of second and third trimester treatment.
Correct management of second and third trimester malaria was significantly higher in those with longer duration of practice (P = 0.0096).
Malarial chemoprophylactic and chemotherapeutic agents used by private medical practitioners.
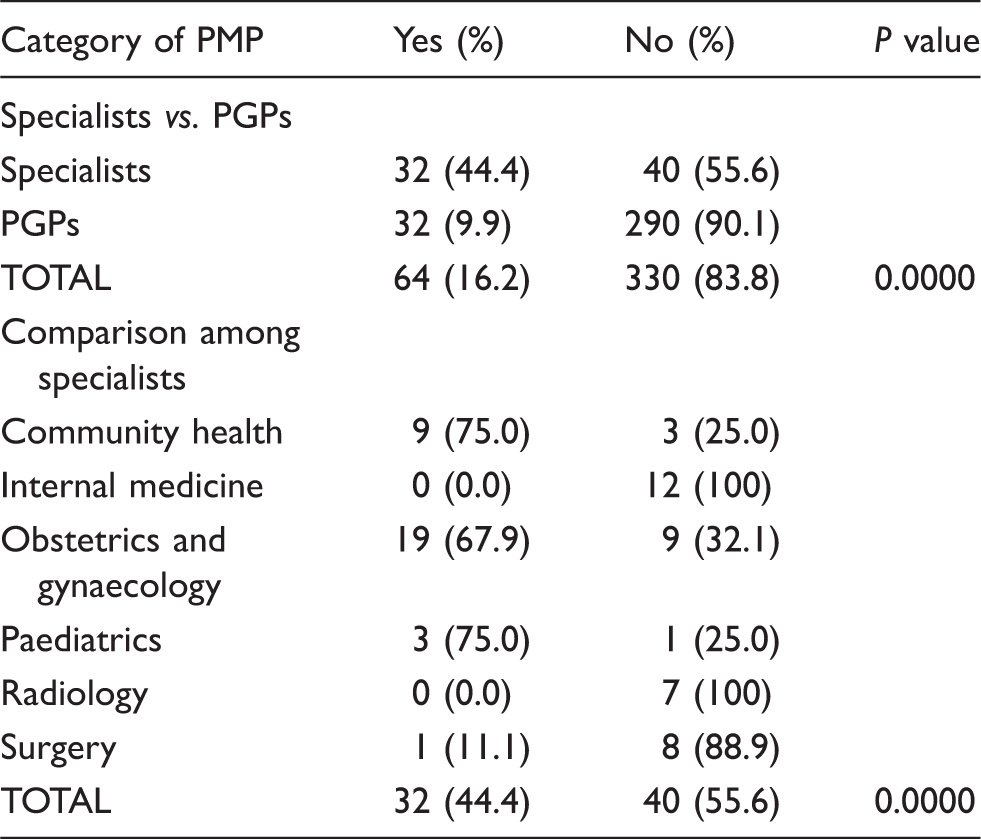
Recommendation of ITN by medical practitioners.
Discussion
Current strategies for malaria control in pregnancy are based on the tripod of IPT, vector control and prompt treatment of acute illness.8,18 The performance of any health system with regards to control of malaria and therefore reduction of malaria-related morbidity and mortality in pregnancy can thus be evaluated by the extent to which it meets these recommended strategies. In most African countries over 70% of pregnant women make multiple antenatal clinic visits and this provides a major opportunity for prevention of malaria. 19
Private medical practitioners have been studied because they occupy a central and strategic position in Nigeria’s healthcare delivery system and are often the first doctors to be visited by patients. Interestingly, apart from general practitioners and obstetricians, many specialists in other fields of medicine who are in private practice also manage women in pregnancy.
This study revealed an embarrassingly poor knowledge of WHO strategies among private medical practitioners. Only 9.9% had correct knowledge of these strategies. Not unexpectedly, more obstetricians and community health specialists, presumably owing to the nature of their training and practice, had better knowledge of these strategies when compared to other cadres of private medical practitioners.
However, the ignorance of WHO strategies for malaria control in pregnancy suggests deficits in professional knowledge for recommended guidelines among a swathe of doctors and may actually be a general reflection of poor knowledge of guidelines among PMPs in the country generally. An earlier study in Lagos to evaluate physicians’ compliance with the WHO recommendation for malaria treatment in the general population showed gross non-compliance 20 and this trend may not be different in other parts of the country and even in other countries in sub-Saharan Africa. A study in Benin Republic showed that the majority of physicians and healthcare workers were unaware of their national policies for the control of malaria. 21
Most of the respondents in this study reported offering malaria chemoprophylaxis to their pregnant patients. However, most of them did not have correct knowledge of the WHO recommendation and this was strikingly evident among PGPs and specialists outside the fields of obstetrics and gynaecology and community health. Even among these, there was still an alarming deficit in practice. This study showed, alarmingly but not surprisingly, that the most common chemotherapeutic agent prescribed in Lagos is still pyrimethamine despite the fact that national guidelines issued in 2005 clearly recommend at least two doses of IPT with SP for prophylaxis. A study in Ilorin, Nigeria also revealed that only three (6%) of 48 private medical practitioners used IPT with SP; the majority (82%) routinely prescribed pyrimethamine. 22 Another study in Nigeria showed that about one-tenth of Nigerian obstetricians surveyed in 2006 did not prescribe malaria chemoprophylactic agents during pregnancy and that the majority of them still relied on pyrimethamine, chloroquine and proguanil. 23 The continued preference for pyrimethamine cannot be justified by its perceived efficacy, safety and cheapness as these elements are met by the SP combination. 24
The National Malaria Control Agency has conducted training in malaria case management in Nigeria. Despite their efforts, it appears that PMPs have not been adequately addressed.
The recommended treatment for pregnant women by the WHO is the use of quinine in the first trimester and the use of artemisinin-based combination therapy (ACT) in the second and third trimesters. 8 This study revealed that this knowledge among PMPs was not in conformity with National Antimalarial Treatment Policy and the WHO Guideline. It is clear from this study that most PMPs, obstetricians inclusive, are deficient in their current practice despite the fact that the guidelines have been made available for almost a decade.
Previous studies in Nigeria and other sub-Saharan countries confirm this trend and have shown that reliance on chloroquine for chemotherapy by private practitioners, their fear of side effects, costs and inadequate knowledge of the recommended chemotherapeutic agents are responsible for low use of quinine and ACTs by private practitioners on their pregnant patients.22,23,25
It is also pertinent to note that the mean duration of practice of private medical practitioners who demonstrated correct knowledge of the WHO strategies as well as that of those who had correct knowledge of second and third trimester treatment were significantly higher than that of those who demonstrated incorrect knowledge. The mean duration of practice of those who demonstrated correct knowledge of prophylaxis as well as that of those who demonstrated correct knowledge of first trimester treatment were also higher than that of those who demonstrated incorrect knowledge although these were not statistically significant. These findings suggest that newly qualified doctors and doctors with few years of practice may have inadequate knowledge of the principles of malaria control in pregnancy and highlights the need to ensure that these principles are well emphasised in the university curricula in Nigeria.
ITNs have been reported to be the most efficacious of all currently feasible interventions for malaria control in Africa and is the only strategy to be used in the first trimester of pregnancy when IPT is not applicable and most drugs are contraindicated. 26 It is therefore surprising that 88.3% of PMPs did not routinely recommend its use for their pregnant patients. Little over two-thirds of obstetricians routinely recommended the use of ITN. The highest figure of 75% was obtained among the community health specialists. A study among healthcare providers in Ibadan, western Nigeria also showed that approximately 50% of doctors do not prescribe the use of ITN for their patients. 27 This non-recommendation of the use of ITNs by many medical practitioners is not unlikely to be a major contributing factor to the low use of ITNs by pregnant women in the country.
In conclusion, private medical practitioners play a key role in the provision of antenatal care services in Lagos, Nigeria but their practice of malaria prevention and treatment in pregnancy falls short of the recommended guidelines and this finding is unlikely to be different in other parts of the country. Private medical practitioners must be encouraged to comply with these guidelines through regular continuing medical education programmes and distribution of educational materials on malaria prevention and treatment in pregnancy. It is also important to emphasise the principles of malaria prevention and treatment in pregnancy in the medical curricula of Nigerian universities.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.