
Abstract
Background
Patients with sickle cell disease (SCD) demand special attention during clinical interventions because they are predisposed to acute chest syndrome (ACS), vaso-occlusive crises, intra-vascular haemolysis and immune paresis. Although SCD is endemic in the Caribbean, there has been no report on endoscopic retrograde cholangio-pancreatography (ERCP) outcomes in these patients from this region.
Study
The records of patients with SCD who underwent ERCP between 1 January 2005 and 1 June 2010 were analysed retrospectively. Parameters assessed included patient demographics, procedural details, ERCP-related and SCD-related morbidity. Data were analysed using SPSS version 12.0.
Results
Fifty-four patients with SCD were subjected to ERCP during the study period. There were 37 women and 17 men at a mean age of 28 years (SD +/−12.05). There was 29% (16) overall morbidity, with 10 (18.5%) SCD-related complications and six (11.1%) ERCP-specific complications. More common complications were: pancreatitis (9.3%); cholangitis (1.9%); ACS (9.3%); pneumonia (3.7%); and painful crises (5.6%). There was one death (1.9%) due to multiple organ failure secondary to severe pancreatitis.
Conclusions
This study suggests that the SCD cohort requires special perioperative attention to minimise the inordinately high morbidity, many of which are SCD-related. We propose a perioperative management protocol that may minimise morbidity in these patients.
Introduction
Homozygous sickle cell disease (SCD) is endemic in the West Indies,1–3 affecting one in 300 people in Jamaica. 1 Pigmented gallstones are present in over 80% of adults with SCD 2 and 45% of them will also have choledocholithiasis.3,4
Many of these patients require endoscopic retrograde cholangio-pancreatography (ERCP) to address choledocholithiasis. While there has been extensive documentation of its safety in medical literature,5–9 there are few data on ERCP outcomes in patients with SCD. Anecdotal evidence suggests that these patients have a higher complication rate than the general population but the outcomes in patients with SCD have not been documented in our setting.
This is important to consider since these patients are already predisposed to unique complications including acute chest syndrome (ACS), vaso-occlusive crises, intra-vascular haemolysis and immune paresis. This study was performed to document the complications after ERCP for choledocholithiasis in a cohort of patients with SCD.
Materials and methods
This retrospective study was performed at a teaching hospital in the Caribbean. At this facility, all patients requiring ERCP were admitted to hospital 24 h prior to the procedure. All anticoagulant and antiplatelet medications were discontinued 72 h prior to the procedure. Normal coagulation status was ensured preoperatively.
We routinely administered a prophylactic dose of third generation cephalosporin 1 h prior to ERCP. Hyoscine N-butyl-bromide (Buscopan, 20 mg) was also given intravenously at the commencement of ERCP to minimise duodenal contractions. The procedure was performed in the Radiology Department under fluoroscopic control. Intravenous sedation with midazolam and pethidine was routinely employed.
In an attempt to minimise morbidity, only consultant gastroenterologists with experienced scrub nurses or assistants were allowed to perform ERCP in patients with SCD. Residents and fellows were not allowed to perform ERCP in these patients despite the fact that this was a teaching hospital.
A complete upper gastrointestinal endoscopy was performed routinely. A catheter was advanced past the sphincter of Oddi into the common bile duct (CBD) for contrast injection. The pancreatic duct was selectively cannulated depending on the indications for ERCP and endoscopic / radiologic findings. Sphincterotomy was selectively performed using the wire guide or end injecting sphincterotome. When detected, stones were removed from the CBD with the use of a balloon catheter or wire basket.
Postoperatively, patients were returned to the wards for monitoring and continued supportive care, including supplemental oxygenation, opioid analgesia, chest physiotherapy and intravenous hydration. The patients were observed overnight and discharged the following day once they were able to ambulate, tolerate normal diet and had adequate pain control.
Between 1 January 2005 and 1 June 2010, we examined the operative log to identify all patients with SCD who were subjected to ERCP for choledocholithiasis. Their hospital records were retrieved and the relevant data extracted for analysis. We excluded patients who were transferred from other facilities for this service since their post ERCP hospital records would not be available for analysis. The data collected included patient demographics, procedural details, ERCP-related morbidity (perforation, pancreatitis, haemorrhage and cholangitis) and SCD-specific morbidity (pulmonary complications, painful vaso-occlusive crises, hepatic sequestration, renal failure and neurologic events).
We employed the standardised definitions of ERCP complications proposed by Cotton et al. 10 in order to standardise outcome evaluation. A perforation was defined as a retroperitoneal or bowel wall leak documented by any radiographic technique or at operation.
Post-ERCP pancreatitis was defined as new or worsened abdominal pain that was associated with a rise in serum amylase of at least three times the upper limit of normal (98 IU/L) requiring prolongation of the planned admission. Serum amylase was selectively measured in patients who were clinically suspected of having pancreatitis.
Haemorrhage was considered significant when there was clinical evidence of bleeding, such as melaena or haematemesis, with an associated fall in the haemoglobin concentration by at least 2 gm/dl.
Cholangitis was defined as elevated temperature greater than 38℃ for longer than 24 h that was thought to have a biliary cause without concomitant evidence of acute cholecystitis.
Patients were considered to have the ACS when plain chest radiographs revealed new pulmonary infiltrates consistent with consolidation involving at least one lung segment in the face of one of the following clinical features: onset of pleuritic chest pain; pyrexia (axillary temperature >38.5℃); tachypnoea; bronchospasm; and/or cough. When these findings were present and sputum cultures were positive, the patients were considered to have a lower respiratory tract infection.
In the absence of a standardised definition, a painful vaso-occlusive crisis was considered to be present when a patient with SCD experienced the sudden onset of severe bone or joint pain that was unresponsive to an adequate dose of oral analgesia in the absence of a demonstrable cause for pain.
Hepatic sequestration was defined as the new onset of clinically detectable hepatomegaly with a fall in haemoglobin levels by at least 2 gm/dl. A neurological event was defined as a change in neurological status accompanied by neurological findings. Renal complication was defined as altered biochemical renal parameters pointing to renal insufficiency, haematuria or proteinuria.
The data extracted from the hospital records during the study period were entered into a Microsoft Excel® worksheet. Data were then analysed using SPSS version 12.0. Cross tabulations were made between individual complications using Pearson’s Chi square tests for comparisons.
Results
Over the study period, 590 patients were subjected to ERCP at this institution. Of these, 54 (9.2%) ERCPs were performed in patients with SCD with choledocholithiasis. There was a 1.6:1 preponderance of women, with 37 women and 17 men. The mean age of these patients was 28 years (SD +/−12.05; age range, 13–66 years; median age, 26.5 years; mode, 14).
Outcomes of ERCP in patients with SCD.
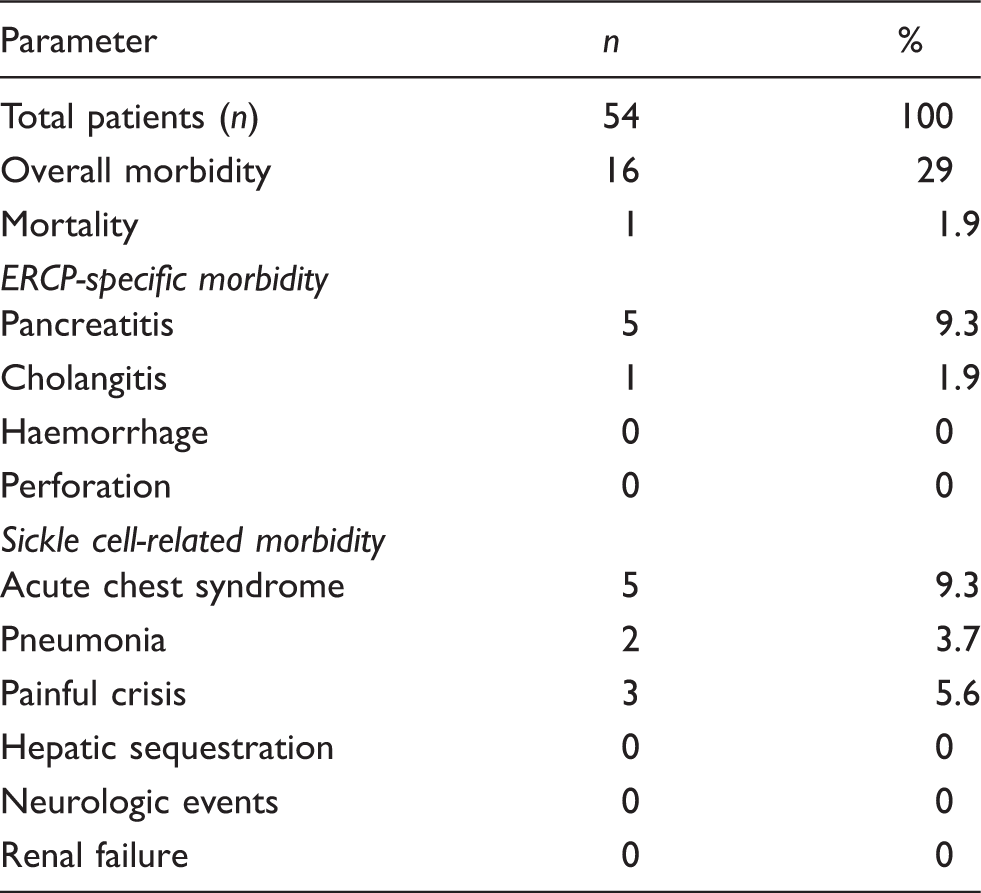
There was successful cannulation and cholangiography in all cases. No biliary stents were required in this cohort of patients. Sphincterotomy was performed in 27 (50%) patients to facilitate biliary instrumentation and/or drainage. In this subgroup, 12 (44.4%) patients developed a complication that included: pancreatitis (n = 4); ACS (n = 4); pneumonia (n = 2); cholangitis (n = 1); and painful crisis (n = 1).
Despite the policy of selective cannulation, the pancreatic duct was inadvertently opacified in 21 (38.9%) cases during contrast injection to access the CBD. In this sub-group, 10 (47.6%) patients developed a complication that included: pancreatitis (n = 4); ACS (n = 3); pneumonia (n = 1); and painful crises (n = 2).
Multiple duct manipulations were required for difficult stone extraction in 18 (33.3%) cases. In this sub-group, 10 (55.5%) developed a complication that included: pancreatitis (n = 4); cholangitis (n = 1); ACS (n = 3); and pneumonia (n = 2). Seven of these patients failed extraction and were subjected to open CBD exploration because laparoscopic stone extraction was not available at the time of this study.
There was one (1.9%) death in this series. This occurred in a 15-year-old boy who had multiple stones within the CBD. After several unsuccessful attempts at stone extraction, he developed a severe pancreatitis (APACHE II score 10) and eventually succumbed to multiple organ failure.
Cross tabulations using Pearson’s Chi square tests were used to detect relationships between each recorded complication and several clinical variables, including age over or below 26.5 years, gender, performance of sphincterotomy, attempts at CBD stone extraction and pancreatic duct opacification. We chose 26.5 years as the cut-off age for comparison because this was the median age in the study cohort.
Difficult stone extraction was the only variable that bore a significant relationship to the occurrence of pancreatitis (P = 0.038) and the ACS (P = 0.038). We noted a trend between an increased incidence of pancreatitis and pancreatic duct opacification, but it did not achieve statistical significance (P = 0.069). Otherwise there was no relationship between pancreatitis / ACS and age <26.5 years (P = 0.640), gender (P = 0.645) or performance of a sphincterotomy (P = 0.351). Neither of the other complications bore any significant relationship to any clinical variables.
Discussion
Previous audits in this institution have documented that ERCP is being performed in the general population with acceptable morbidity and good therapeutic outcomes.11,12 This study now demonstrates that persons with SCD have a higher incidence of complications after ERCP (29%). We do not believe that this is endoscopist-dependent because the morbidity (8%) in the general population at this institution with the same endoscopists was documented to be in the range of 4–10.8%, which is considered acceptable in high volume centres.5–9
When only ERCP-related complications were evaluated, the complication rate reduced to 11.1% but this was still greater than acceptable morbidity rates reported from large volume centres.5–9 In order to reduce ERCP-related morbidity, the individual complications should be analysed.
Acute pancreatitis was the most frequent complication and the incidence (9.3%) was greater than the acceptable range of 3.0–7.2% in high volume centres.5–9 There are several established risk factors for pancreatitis in unselected patients: young age, female gender, difficult CBD cannulation, performance of a sphincterotomy, prior pancreatitis and Sphincter of Oddi dysfunction.13–15 We observed an association between pancreatitis and pancreatic duct opacification. Although this relationship did not bear statistical significance (P = 0.069), we do recognise that the study population is small. A larger sample size may have achieved statistical significance. However, homozygous SCD is an uncommon disease and it may be difficult to accrue a large sample size of these patients who undergo a specialised procedure such as ERCP.
Despite the policy of selective CBD cannulation, there was unintended filling of the pancreatic duct during contrast injection to access the ampulla. Wire-guided cannulation has been proposed as a method to avoid this phenomenon that is seen in the conventional method where contrast injection is used to identify and gain access to the CBD. Three prospective randomized trials compared wire-guided cannulation and conventional contrast injection in 1,000 patients.16–18 They independently demonstrated significant reductions in the incidence of pancreatitis when wire-guided cannulation was utilised. Adoption of the wire-guided cannulation method may be one way to reduce the incidence of pancreatitis in this setting.
Prophylactic pancreatic duct stenting is another intervention to consider. Shi et al. 19 performed a meta-analysis on 1,176 patients across 10 randomised controlled trials comparing the pancreatic duct stenting on post-ERCP pancreatitis. They demonstrated that pancreatic duct stenting significantly reduced the incidence of pancreatitis and reduced the severity in those patients who still developed pancreatitis. Although the indications for prophylactic stenting remain unsettled, it may be an intervention worth investigating in this high-risk cohort with SCD.
Several pharmacologic agents have been shown to decrease the incidence of pancreatitis after ERCP in well-designed meta-analyses. The agents include protease inhibitors (nafamostat-mesilate), 20 rectal NSAIDs (indomethacin and diclofenac) 21 and somatostatin. 22 Use of these agents may also be worthy of consideration in this high-risk group of patients with SCD.
Difficult stone extraction was the only factor that could predict both pancreatitis and the ACS. Difficult extraction, repeated biliary instrumentation and excessive manipulation are already recognised to be established risk factors for pancreatitis13–15 but the relationship with the ACS has not been documented before and is difficult to explain. We theorise that it may occur as a result of diaphragmatic splinting due to the local inflammatory response / increased pain from repeated manipulation of the biliary tree.
It was noteworthy that almost two-thirds of all complications were SCD-related despite meticulous attention to detail in the perioperative period. Pulmonary complications were the commonest form of SCD-related morbidity, with ACS being most common (9.3%). This is one of the most feared complications because it is the leading cause of mortality in SCD, 23 resulting in death in 3% of affected patients.23,24
We did not encounter any reports detailing the incidence of the ACS in patients with SCD who had ERCP. There is a theoretically high risk of ACS from hypoventilation with intravenous sedation and the mandatory gastric insufflation that causes left basal atelectasis. Comparatively, we saw a lower than expected incidence (9.3%) when compared to studies that reported on patients with SCD undergoing other biliary tree operations in which the incidence of ACS was in the range of 20–33%.3,24
When patients in this setting are diagnosed with ACS, the reported mortality was in the range of 16.7–25%.3,24 Again the mortality in our study was lower than expected since there were no deaths in the five patients who developed the ACS. There was one death in our study but this occurred after multiple organ failure from severe post-ERCP pancreatitis (APACHE II Score 10).
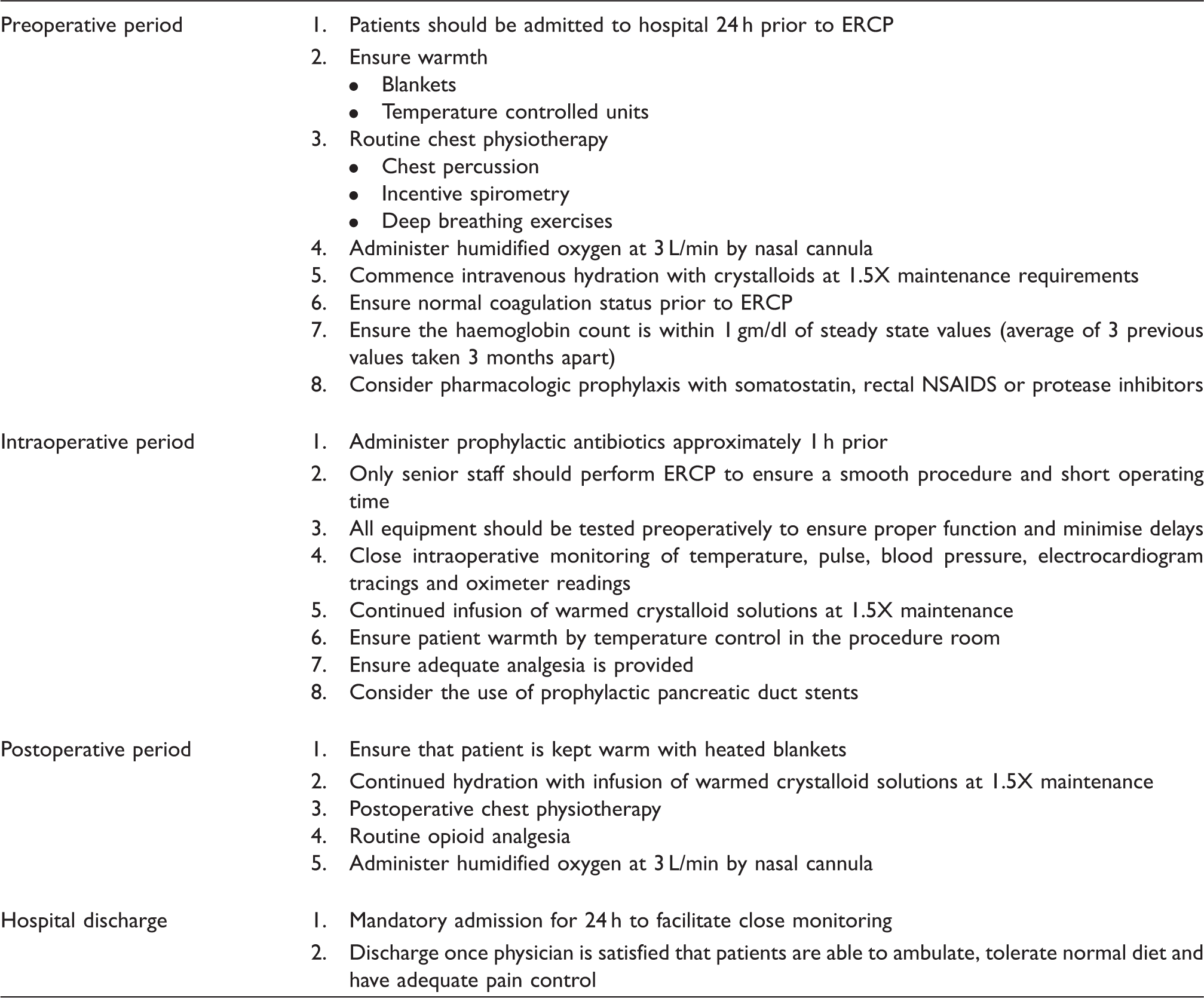
Management protocols for patients with SCD undergoing ERCP.
Conclusions
Patients with SCD require special perioperative attention to minimise the inordinately high morbidity, most of which are SCD-related. Introduction of standardised perioperative management protocols may minimise the morbidity in these patients.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.