
Abstract
Acute arsenicosis, although having a ‘historical’ background, is not common in our times. This report describes a case of acute arsenic poisoning, missed initially due to its gastroenteritis-like presentation, but suspected and confirmed much later, when the patient sought medical help for delayed complications after about 2 months.
Introduction
Arsenic is one of the classic poisons, well known throughout history. 1 Because of its tasteless and odourless properties it became a popular murder weapon. Although, chronic arsenicosis is a public health crisis in Bangladesh and West Bengal (India) owing to ground water contamination, acute arsenic poisoning is uncommon nowadays. The clinical manifestation of acute arsenic toxicity is diverse, involving the digestive, cardiovascular, neurologic, cutaneous and renal systems. If the victim survives the initial phase, peripheral neuropathy and bone marrow suppression develop with skin lesions. 2 This report describes a case of acute arsenic poisoning, missed initially, being confused with simple gastroenteritis.
Case report
A 17-year-old boy, resident of Keshobpur, Jessore, Bangladesh, presented with flaccid quadriplegia lasting approximately 1 month. His initial symptoms, 2 months prior, were acute vomiting and diarrhoea after taking some ‘pitha’ (homemade cakes, a local delicacy), which resulted in his admission to the local primary care hospital. There he was managed with fluid resuscitation only. Subsequently, because of his worsening state, he was transferred to the regional medical college hospital. His gastrointestinal symptoms continued for 2 more days and thereafter resolved, but he subsequently developed generalised swelling and jaundice. He became unconsciousness and had generalised convulsions on several occasions. Initial laboratory investigations showed a hyperbilirubinaemia (176.6 µmol/L), raised alanine aminotransferase (160 U/L) and serum creatinine (159.1 µmol/L), hyponatraemia (126.8 mmol/L), hypokalaemia (2.56 mmol/L), leukopenia (3800/ µL) with a normal differential, and anaemia (Hb 7 g/dL). Abdominal ultrasonography showed mild hepatomegaly with moderate ascites and bilateral small pleural effusions. With these findings, a diagnosis of acute fulminant hepatic failure was made. After 15 days, he regained consciousness, but talked and behaved inappropriately, though this resolved spontaneously after 4 days. On the 20th day, gradual weakness and pain developed in all four limbs, starting from the legs and moving to the arms. As his weakness was worsening, he was transferred once more to Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, 2 months after his initial presentation.
Significant information, delivered by the young man’s parents, was that the ‘pitha’ he ingested was provided by someone who had knowledge of herbal and indigenous medicine, who entertained some rivalry with the family and had later absconded. Thus emerged the possibility of a criminal intoxication.
On admission at BSMMU, careful examination noted Mee’s line (Fig. 1) and some pigmentation on his lower limbs. There was distal muscle wasting with wrist and foot drop (Fig. 2). All the deep reflexes were absent, the plantar reflex being equivocal and all sensory modalities were lost in a glove-and-stocking pattern. An ultrasound abdominal scan was normal. Nerve conduction velocity tests showed mixed sensorimotor demyelination and axonal polyneuropathy.
Mee’s line (arrow). Wrist and foot drop.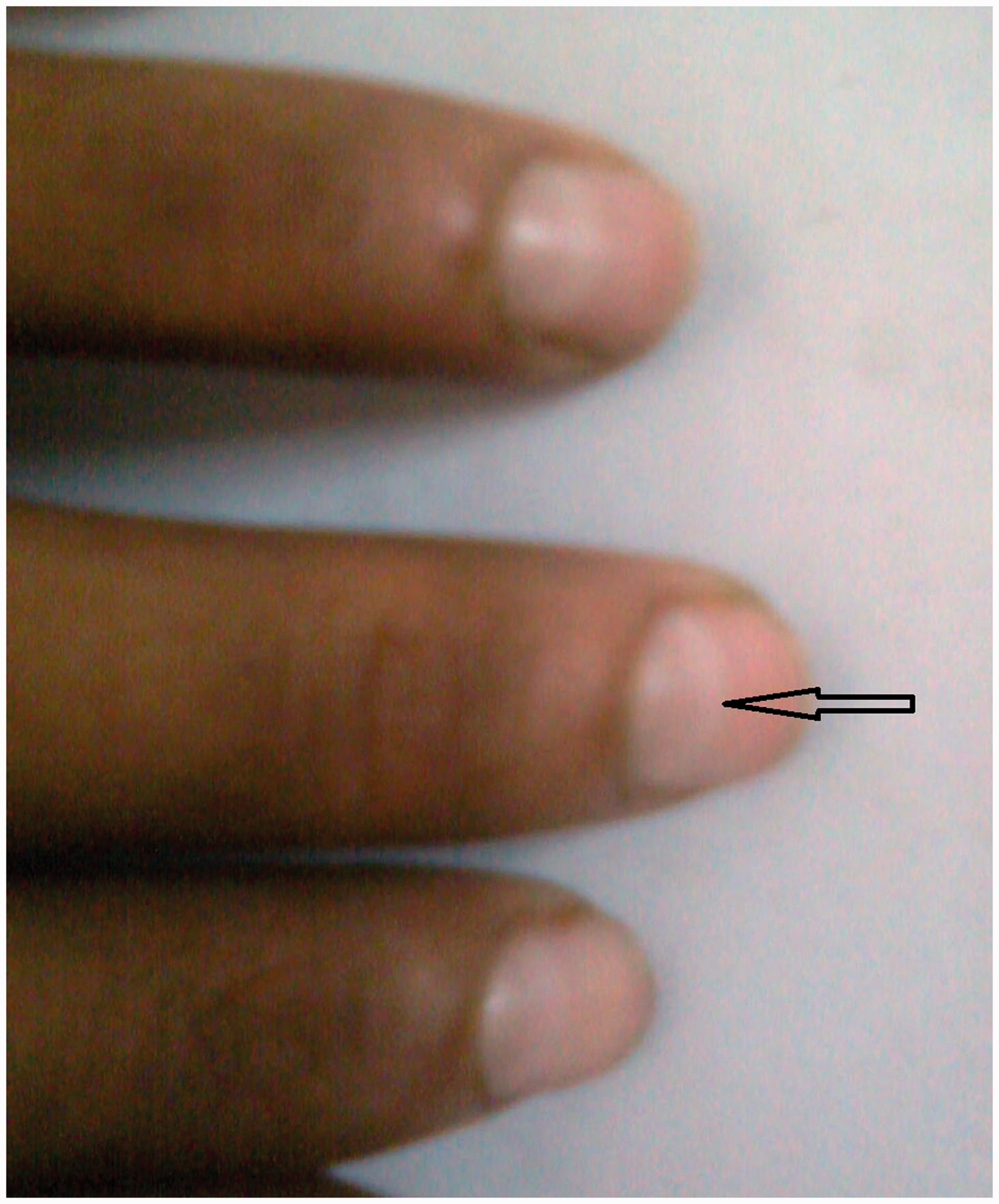

In view of the possibility of attempted homicide, the clinical findings of acute gastroenteritis with acute hepatorenal failure, followed by peripheral neuropathy and the presence of Mee’s line, indicated the likelihood of arsenic poisoning. The arsenic level of a hair sample was indeed found to be 19.3 mg/kg (normal <3 mg/kg). A treatment with dimercaprol (3 mg/kg intramuscularly every 4 h for the first 2 days, 6-hourly at day 3 and 12-hourly for the next 10 days) was commenced. Despite completing the treatment, there was no significant improvement in neurological function. However, at the 3-month follow-up, the Mee’s line had disappeared and he could walk with aid. After 2 years, the wrist and foot drop had resolved (Fig. 3) and daily activities could be performed without help.
Improved wrist drop and patient standing on his own.
Discussion
Acute arsenic intoxication is not common and is less frequent than 50–100 years ago. In addition to natural sources, it is also found in many manufactured products like pesticides, ceramics, enamels, homeopathic and indigenous medicines, as well as preservatives for hides. It is also used in the manufacture of glass and fireworks. 3 Its oxide forms usually exert toxicity by inactivating up to 200 enzymes, involved in cellular energy pathways, DNA synthesis and repair. 2
The classic symptoms after acute poisoning are oral and epigastric burning, followed by nausea, vomiting, tenesmus and profuse rice-watery diarrhoea. 4 The irritant action of arsenic causes bleeding and capillary transudation into the gastrointestinal mucosa. The course of the poisoning is then dictated by the dose ingested. With massive ingestion there is rapid progression to multi-organ failure (renal failure, hepatocellular necrosis, respiratory failure, encephalopathy, acute psychosis and toxic cardiomyopathy).1,2,4 Death is generally caused by circulatory collapse resulting from intense gastroenteritis and from multi-organ failure.3,4 In acute cases, an abdominal radiograph may help in making the diagnosis by revealing radio-opaque material in the gastrointestinal tract. 5
With sublethal doses, the gastrointestinal illness resolves early and injury to other organs resolves eventually. Jaundice and body swelling can be explained by arsenic-induced hepatic and renal failure. Inappropriate behaviour, which normally subsides spontaneously, is due to direct central nervous system dysfunction by the arsenic. 6 Untreated, subacute polyneuropathy develops 7–14 days after exposure. This subacute form of arsenic poisoning may evolve into a severe chronic sensorimotor neuropathy. 1 Autopsy and animal toxicity studies suggest that arsenic may be toxic to the nerve cell body, leading eventually to axonal dysfunction. 7 Mee’s lines (prominent white transverse lines on fingernails and toenails, caused by arsenic deposition in the keratin reach areas) occurs 4–6 weeks after exposure.1,2 Pigmented dermatitis is also a sign of arsenic toxicity. Among variable haematological manifestations, arsenic-induced bone marrow suppression is reversible once the exposure ceases. 2
Determination of total arsenic in the urine is a more representative measure of inorganic arsenic, but it is excreted in the urine within the first 4–5 days after exposure. 1 As our patient presented about 2 months after ingestion, hair arsenic level had to be measured. Hair arsenic level of 1–3 mg/kg signifies acute poisoning, while 0.1–0.5 mg/kg is indicative of chronic poisoning. 2 In a highly exposed population, where the environmental arsenic water concentration is 1090 µg/L, hair arsenic level may be as high as ∼8.5 mg/kg. 8 A hair arsenic level of 19.3 mg/kg in our patient was nonetheless high enough to indicate acute poisoning.
In spite of a late presentation, our patient was treated with dimercaprol on the basis that ingested arsenic is absorbed slowly, 1 and thus effective chelation and prevention of further complication might be achieved.
Conclusion
Although this case presented classically, diagnosis was difficult because of its rarity and the manner of presentation. A high index of suspicion and careful observation may lead physicians to an early diagnosis and appropriate initiation of treatment of arsenic poisoning may prevent the development of long-term complications. This case is reported in the hope that it will alert practising clinicians to consider acute arsenic poisoning, even as a remote possibility, in patients presenting with severe gastroenteritis, particularly if followed by features of peripheral neuropathy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.