
Abstract

Introduction
Staphylococcal meningitis is uncommon in children. The occurrence of brain abscess as a complication is rare, with most cases having an underlying focus of infection. 1
We report two cases of brain abscess in young breastfed infants associated with breast abscesses in their lactating mothers, an association that has not been reported earlier.
Case 1
A 5-month-old boy was admitted with fever and irritability of 2 days’ duration. The mother had noticed that the baby had not attained social smile and head control. He was delivered at term by Caesarean section, with birth weight at 1800 g. Six weeks after delivery, the mother had an abscess on her left breast, which was incised and drained and she was treated with amoxicillin for 1 week. On admission, the boy was conscious and irritable with stable cardiorespiratory status. The anterior fontanelle was tense and there was sutural separation. Head circumference was 44 cm. There was no focal neurologic deficit. Other systems were normal.
A diagnosis of pyogenic meningitis was considered and he was started on cefotaxime and vancomycin. Investigation revealed anaemia and neutrophilic leucocytosis. Cerebrospinal fluid (CSF) study was suggestive of pyogenic meningitis with protein 1720 mg/L, sugar 1.322 mmol/L and cells 50 per cmm. Computed tomography (CT) scan of the brain showed multiple ring enhancing lesions in the right cerebral hemisphere suggestive of abscesses (Figure 1) from which about10 mL of pus was aspirated. Culture of CSF and blood were negative, but pus aspirated from the brain abscess revealed MRSA. There was no evidence of immune deficiency including HIV infection.
Multiple ring enhancing lesions in the right cerebral hemisphere.
Treatment with vancomycin was continued with rifampicin added on, as the child had persistent fever. Three weeks later, the boy developed generalised seizures, which required multiple anticonvulsants.
A nasopharyngeal swab of the mother showed growth of MRSA. She was advised local application of mupirocin. Magnetic resonance imaging (MRI) done after 1 month showed multiple brain abscesses in the right cerebral hemisphere with ventriculitis and non-communicating hydrocephalus.
He continued to have intractable seizures and died 2 months later.
Case 2
A 49-day-old male infant, first-born of non-consanguineous parents, was admitted with multiple focal seizures of 1 day’s duration, initially involving the right upper limb, later becoming generalised. There was no history of fever or other symptoms. The mother had pre-eclampsia and the baby was born vaginally near term with a birth weight of 2130 g. The baby was treated for bronchopneumonia at the age of 2 weeks and was exclusively breastfed. The mother had a left-sided breast abscess, which was drained 1 week prior to the baby’s illness, for which she received oral cloxacillin.
On examination, the baby was drowsy, with stable vital signs and no focal neurological deficits. The anterior fontanelle was bulging.
Investigations revealed polymorphonuclear leucocytosis with a positive C-reactive protein. There was no evidence of immune deficiency including HIV infection. CSF had total white cell count of 60 cells/cmm with 97% lymphocytes, CSF protein was 750 mg/L and sugar was 2.77 mmol/L. Blood sugar was 6.1 mmol/L. Blood and CSF culture were sterile. The boy was started on parenteral cefotaxime and ampicillin. On the 10th day of hospitalisation, he had seizures involving the right upper limb.
A CT scan of the brain revealed multiple hypodense collections with contrast-enhancing walls in the left interhemispheric fissure with mass effect and midline shift and multiple hypodense areas in the left frontal and parietal lobes (Figure 2). A diagnosis of multiple brain abscesses was made and10 mL of pus was aspirated. Culture yielded methicillin sensitive Staphylococcus aureus.
Multiple hypodense collections with contrast enhancing walls in the left interhemispheric fissure with mass effect and midline shift and multiple hypodense areas in the left frontal and parietal lobes.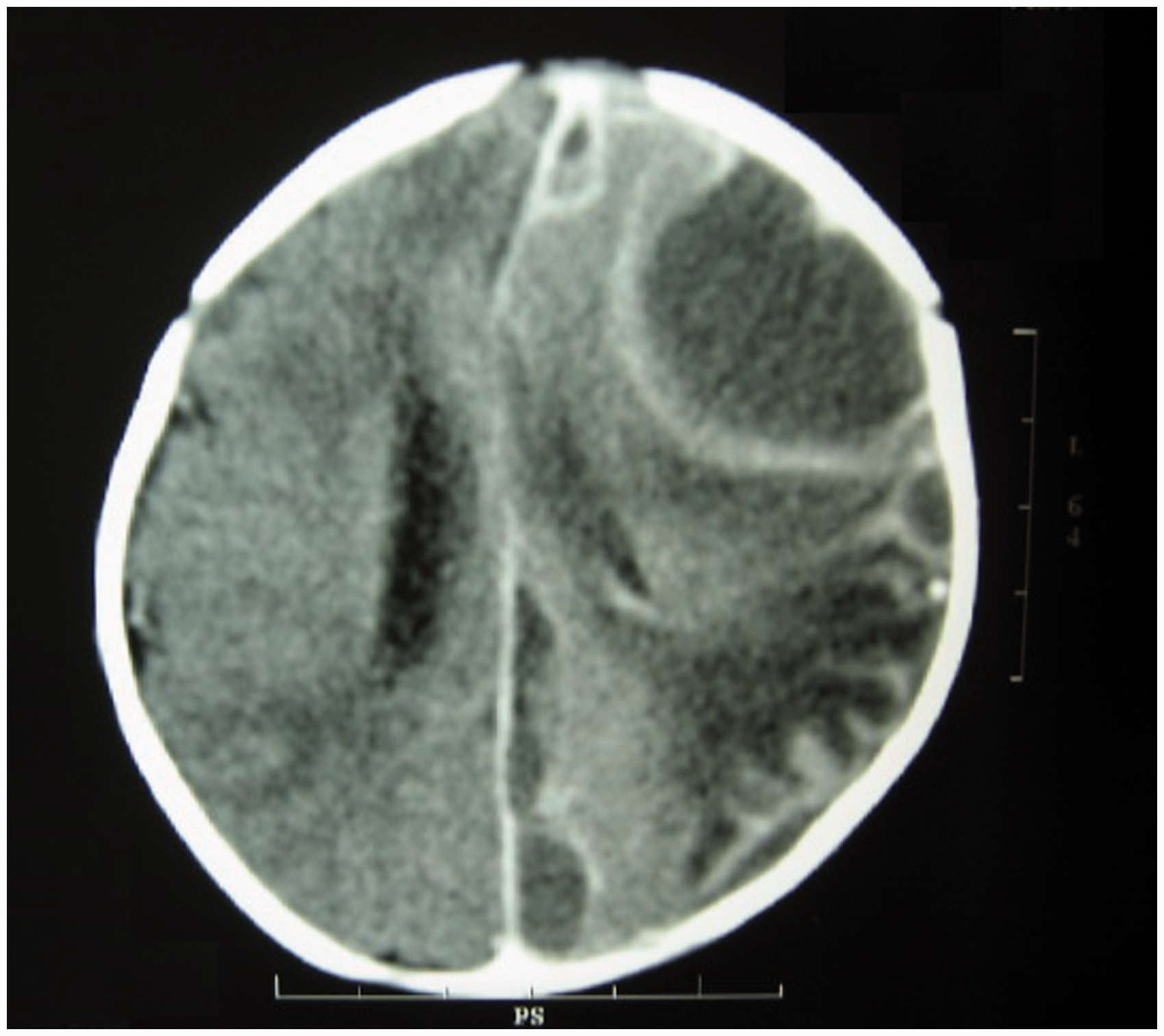
Treatment with vancomycin, ceftriaxone and metronidazole was continued for 2 weeks, after which linezolid was given orally. On follow-up at 3 months, he had normal development and no neurological deficits.
Discussion
Meningitis due to Staphylococcus aureus is uncommon, with an estimated incidence of 0.114 per 100,000 in the general population in the United States. 1 Most of the cases are nosocomial infections, with community acquired staphylococcal meningitis having an incidence as low as 1.3% in a study of 2319 patients with bacterial meningitis during the period 1983–1998 in Brazil. 2 Brain abscess occurring as a complication is very rare.3–5
Over a period of 6 years, three such cases were admitted in the paediatric intensive care unit of our hospital out of 9928 admissions. Two of these breast-fed babies had a history of a maternal breast abscess. Transmission of infection from mother’s breast milk causing neonatal sepsis has been reported.6,7 No case report of brain abscess associated with maternal breast abscess was found after a literature search.
Both mothers had breast abscesses prior to the onset of symptoms in their babies, of whom one had her abscess drained several weeks earlier, an indication of the possibility of persistent nasopharyngeal carriage. Both babies had Staphylococcus aureus grown in culture from pus aspirated from their brain abscesses. MRSA was grown from a nasopharyngeal swab of one of these breastfeeding mothers. Timely treatment of the mother could have prevented the development of breast abscess in this baby. Nasopharyngeal carriage of MRSA can be easily treated with local application of mupirocin. This underlines the importance of a careful search for a source of infection in all cases of Staphylococcal infections in young babies, including a detailed history from their mothers.
Anticipating the possibility of Staphylococcal infection in the baby of a mother with breast abscess would result in early diagnosis and initiation of anti-staphylococcal treatment. Lactating mothers with breast abscesses should be screened for persistent nasopharyngeal carriage and treated appropriately. This is a classic example of a simple and cost-effective intervention that can prevent infant mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.