
Abstract
Objective
To evaluate clinically the efficacy and safety in northern India of cefepime monotherapy versus piperacillin-tazobactam in patients of paediatric age group with febrile neutropenia.
Material and Methods
Children aged ≤18 years admitted febrile with chemotherapy-induced neutropenia were randomised into two groups comprising 20 cases in each group viz. CEF (receiving cefepime only) and PIP-TAZO (receiving piperacillin-tazobactam). Based on clinical and laboratory tests, patients were classified into: microbiologically documented infections (MDI); clinically documented infections (CDI); and unexplained fever (UF). They were assessed for clinical signs and symptoms as well as laboratory parameters at the time of enrolment and subsequently on days 3 and 7.
Results
Incidence of MDI, CDI and UF were 22.5%, 47.5% and 30%, respectively. The mean duration of neutropenia (in days) was 5.45 ± 2.1 in the PIP-TAZO group and 5.5 ± 1.5 in the CEF group (P = 0.305). The success rate defined as clearing infection effectively and improvement of neutropenia was comparable (P = 0.705). There was a mortality rate of 20% in the PIP-TAZO group as compared to 10% in the CEF group.
Conclusion
We conclude that cefepime monotherapy and piperacillin-tazobactam are equally efficacious and safe in treating patients with febrile neutropenia. Empirical monotherapy with cefepime would prevent an unnecessary extra economic burden as well as avoiding the serious adverse or toxic effects of multi-drug regimes, especially in low- and middle-income countries.
Introduction
Fever is a common occurrence in cancer patients, particularly among those taking chemotherapy. When infection occurs in a patient with neutropenia, this may prove fatal. Although mortality with therapeutic advances has reduced, infection still remains the major cause of morbidity and mortality. 1 Thus febrile neutropenia remains a serious oncological emergency. Fever is seen in almost half of the patients with solid tumours and in more than two-thirds of those with haematologic malignancy chemotherapy-induced neutropenia. 2 It is critically important for the clinician to diagnose febrile neutropenia quickly and accurately, recognise signs and symptoms of infection in neutropenic patients, and provide appropriate and timely management of this condition.
Evaluation of febrile neutropenia begins with a careful history and physical examination. Empiric antibiotics should be started immediately after sending off basic clinical investigations, which include a full blood count and culture sensitivity of relevant specimens. Initiation, modification and termination of antibiotic therapy are critical. Prompt initiation of empirical antibiotics should not be delayed if cultures and sensitivities are not available. The approach to selecting empirical antimicrobial agents depends upon the nature of the neutropenic host, characteristics of clinical presentation and expected duration of neutropenia. The empirical regimen must be broad, achieve high bactericidal levels, and be as non-toxic and as simple to administer as possible. In the past, a combination therapy of two drugs was advocated which usually included a third or fourth generation cefalosporin or an extended spectrum penicillin (e.g. piperacillin-tazobactam) and an aminoglycoside 3 but recently modified Infectious Disease Society of America (IDSA) guidelines (2010) 4 now recommend the use of empirical antimicrobial (either CEF or PIP-TAZO).
Although standard treatment with multi-drug regimens leads to dramatic decline in mortality rates, they also give us new concerns. Multi-drug resistant micro-organisms have emerged during the last decade, probably due to the indiscriminate use of these broad-spectrum antibiotics. The explanation for this continuing problem with infection is obviously multi-factorial, but the widespread use of antibiotics has frequently resulted in unrealistic over-dependence on their effectiveness in treating disease. Monotherapy may work effectively in a high-resource setting but its efficacy has not been extensively researched in resource-poor circumstances.
Material and Methods
This open-label prospective randomised controlled trial was carried out on 40 patients with febrile neutropenia admitted to Pt. B.D. Sharma PGIMS, Rohtak which is a government-funded tertiary care centre for critically ill children, catering for a heterogeneous population from rural Haryana and surrounding states of northern India. The study was carried out between May 2012 to August 2013.
Inclusion criteria were: patients aged ≤18 years, with a diagnosis of any malignancy, receiving chemotherapy; having an absolute neutrophil count (ANC) ≤500 cells/cu mm or an ANC <1000 that was likely to fall to less than 500 cells/cu mm over the next 48 h, based on the trend shown by previous laboratory counts; having a single oral temperature of ≥38.3℃ or a temperature of ≥38℃ sustained over a period of 1 h in the absence of any other cause of fever; and not receiving any other antimicrobial therapy within 1 week prior to admission to the study.
Exclusion criteria were: the presence of fever attributable to malignancy or transfused blood products or medications; the administration of any systemic antimicrobials within 1 week prior to enrolment; having hypersensitivity to the drugs being evaluated; having evidence of hepatic insufficiency (defined as aminotransferase levels >5× normal values) or renal insufficiency (defined as a creatinine clearance of <30 mL/min); or protocol violations including non-compliance.
Intervention
Informed consent concerning the protocols was sought. A complete history and physical examination was performed and vital observations were charted at 2 h intervals. Full blood counts, liver and renal function tests, and two sets of blood cultures obtained simultaneously from two peripheral veins (including one from each lumen of a central venous catheter, if present) were taken. A chest radiograph was obtained and cultures and sensitivities determined from routine urine samples and from any other sites of suspected infection as clinically indicated. Blood samples were collected again from all patients on days 3 and 7. Complete full blood counts, including the Absolute Neutrophil Count (ANC), were obtained daily. Further bacteriological samples were obtained as necessary until either the organism was eradicated or the initial antibiotic treatment was changed.
Patients were randomly allocated with the help of a computer-generated random number to receive either piperacillin-tazobactam (PIP-TAZO) (100 mg/kg/dose every 8 h) or cefepime (CEF) (50 mg/kg/dose every 8 h). Based on clinical and laboratory tests, patients were classified into the following categories: patients with microbiologically documented infections (MDI); patients with clinically documented infections (CDI); and patients with unexplained fever (UF).
Patients were evaluated for the efficacy of therapy on day 3 to determine whether the initial antibiotics needed to be changed. The response criteria were as follows: success, defined as defervescence (<37℃) within 2 days after starting the assigned empirical therapy; and failure, defined as a body temperature of (>37℃) by the end of the first 2 days, in which case the therapy was changed.
When a positive identification of causative microbe was made, treatment was modified according to its susceptibility. The final evaluation of treatment response was performed at day 7 using the following criteria: success, defined as defervescence (<37℃) that occurred within 2 days after starting the initial therapy and being completely maintained for 7 days with significant improvement of infection-related signs, symptoms and abnormal laboratory values; and failure, defined as therapeutic response other than that described above which included change of antimicrobial therapy after 48 h or a body temperature of >37℃ at the end of 48 h.
All antibiotics were discontinued after patients had been afebrile for 7 days and following the disappearance of signs of infection regardless of neutrophil recovery (ANC > 500/mL). Statistical evaluation was performed using the SPSS 16.0 statistical software. The χ2 test and Mann–Whitney U test were used for comparison. A P value ≤ 0.05 was considered statistically significant.
Results
During the study period 53 patients were screened for randomisation. Thirteen patients were excluded for various reasons; hence 40 patients were randomised after taking informed written consent (Figure 1).
Flow diagram of the study.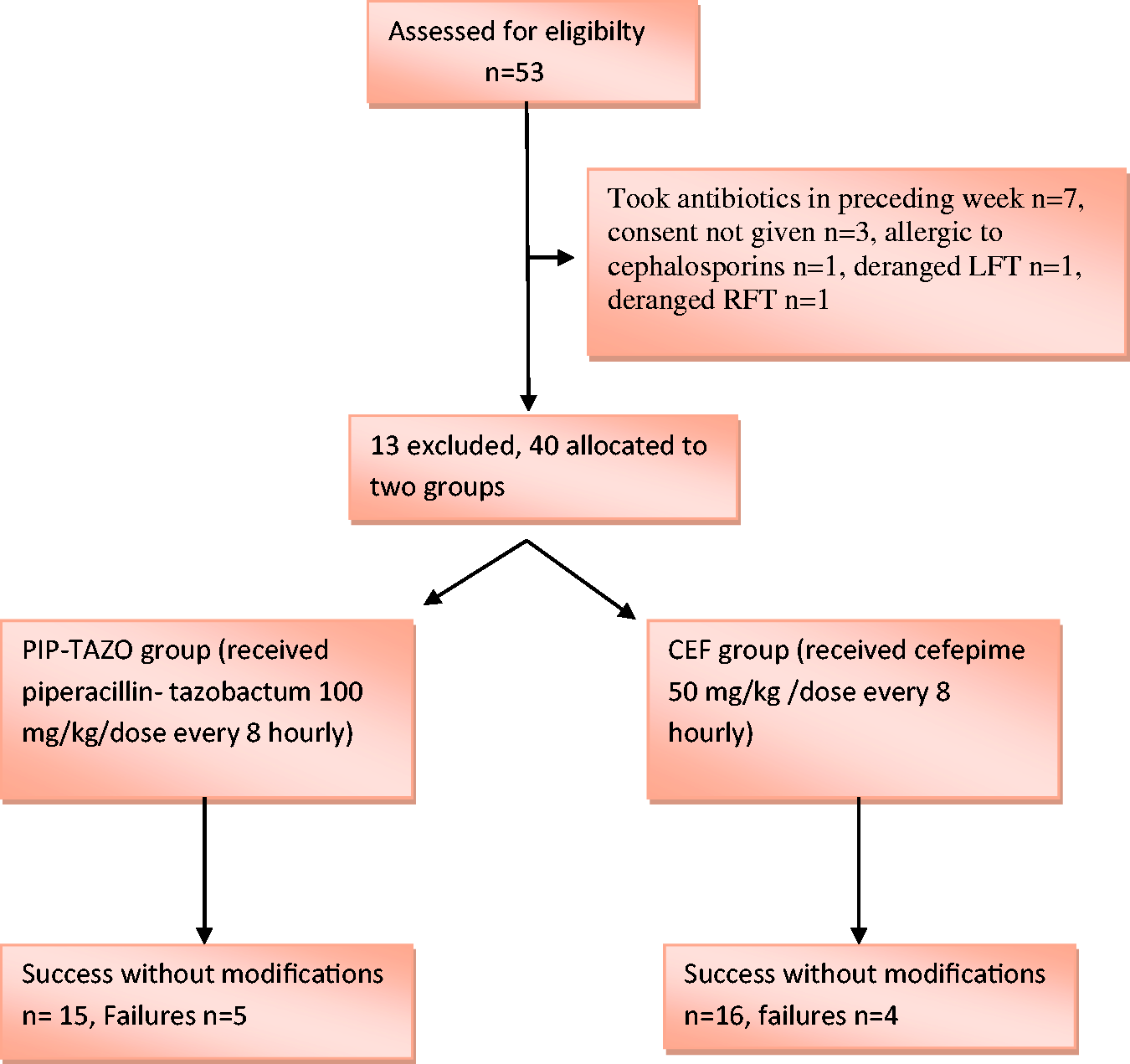
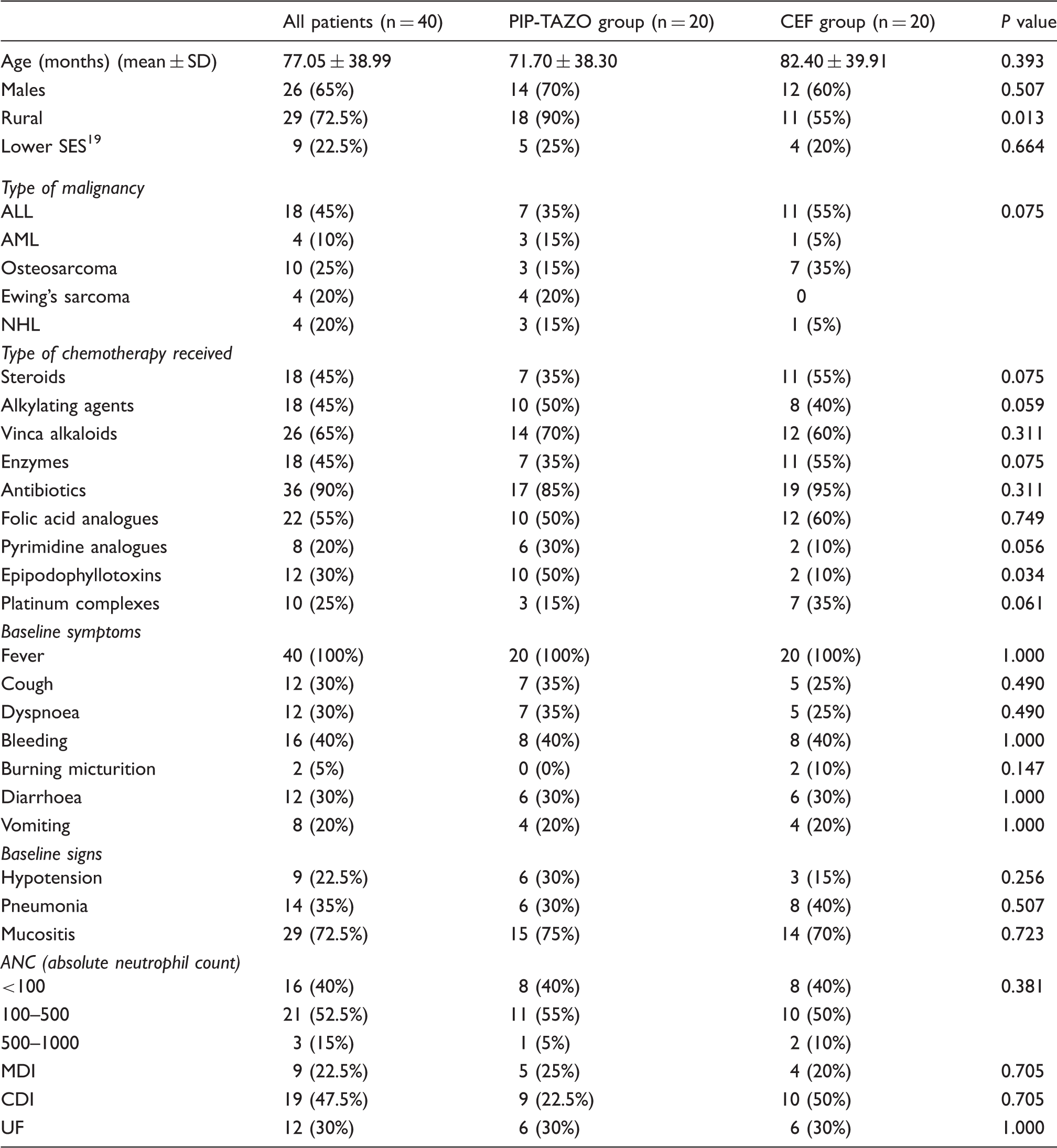
Demographic and baseline clinical and lab parameters (n, %).
Clinical and laboratory parameters on days 3 and 7.

Of note is that some patients received their drugs free through government supplies, but others had to purchase them, depending on current availability. Nonetheless, it was clear that both CEF and PIP-TAZO groups paid less than combination drugs would have cost, and cefepime was substantially cheaper than piperacillin-tazobactam.
Discussion
Patients with febrile neutropenia usually have no obvious infectious aetiology documented. Clinically documented infections occur in only approximately one-third of febrile episodes, with the focus of infection commonly localised to the intestinal tract, lung and skin. Microbiologically documented infection occurs in about 25% of all patients, especially in patients with prolonged or profound neutropenia (ANC < 100 neutrophils/mm).1,5–7
The mean duration of neutropenia and the yield of MDI (by positive blood culture) in our study were similar to other studies 1,8–10 However, most of the bacterial isolates in our study were Gram-negative, whereas predominantly Gram-positive organisms were isolated in other studies. This was probably due to prevalent Gram-negative nosocomial sepsis at our institute and a less frequent usage of indwelling catheters, commonly utilised in high-resource settings.
We found a higher incidence of clinically documented infections (CDI) and lower incidence of unexplained fever, which was not concordant with other studies.8,11,12 The reason for this dissimilarity may be attributed to delayed presentation in our setting, so that at presentation clinical symptoms become evident.1,12
Our overall success rate of treatment was 77.5%. Although most studies8,9,11–14 had a success outcome of 50–60%, a few others15,16 reported a success rate of 80–90%. However, our good results may be related to our small sample size. We nonetheless had a high mortality of 15% which was not consistent with most of the previous studies.8,10,11,16–18 It must be mentioned that in our setting, there are a limited number of intensive care unit beds needed for such critically ill patients. Mortality at our centre with either CEF or PIP-TAZO (15%) was comparable to that of treatment with combined therapy (17%). Moreover, monotherapy is more cost-effective and with probably fewer adverse effects as it avoids the use of aminoglycosides of combined therapy.
No significant adverse effect were noted in any of the study groups, and no patient required antibiotic modification. Minor effects noted were not dissimilar with other studies.
The limitations of our study were its small sample size, our poor yield of microbiologically documented infections, a lower incidence of solid tumours among our patients and our higher mortality rates.
Conclusion and Summary
Our study confirmed the efficacy and safety of monotherapy, recommended by latest IDSA guidelines, 2 of the use of cefepime or piperacillin- tazobactam in the management of febrile neutropenia outside western centres. This means that serious adverse or toxic effects of multi-drug regimens may be avoided and unnecessary costs spared. Furthermore, it is possible that mortality may also be reduced. Importantly, cefepime costs approximately 20% of the price of piperacillin-tazobactam with no poorer effect.
Nonetheless, a larger multi-centre randomised controlled trial may be required before these generalisations can be accepted in this part of the world.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.