
Abstract
Rheumatic manifestations may be prevalent in more than 30% of patients with infective endocarditis (IE), often predating this diagnosis by several months. A case series of five patients recorded at a tertiary care Rheumatology and Clinical Immunology unit over a period of 1 year emphasises that varied presentations of endocarditis may mimic uncommon rheumatic diseases.
Introduction
Infective endocarditis (IE) refers to infection of native or prosthetic heart valves and the endocardium. IE often occurs in patients with underlying structural cardiac abnormalities predisposing to turbulent flow; however it can also occur in structurally normal hearts. 1 Rheumatic manifestations such as myalgia, arthralgia, arthritis and back pain are prevalent in nearly 40% of patients with IE at presentation, 2 antedating the diagnosis by weeks to months.2,3 Patients with rheumatic diseases often require immunosuppressive medication; hence it becomes all the more relevant to be aware that IE may mimic rheumatic diseases, more so in tropical countries where infectious diseases are more prevalent. We share our experience of patients of IE presenting with classical syndromes of various rheumatic diseases.
Methods
The medical records of patients over 1 year (from 1 February 2013 to 31 January 2014) from a tertiary care referral centre in North India, presenting to the Department of Clinical Immunology and Rheumatology, were reviewed. Patients diagnosed with IE based on modified Duke’s criteria 4 were included. The commonest risk factors for infective endocarditis (IE) in our setting are rheumatic heart disease, congenital heart disease and mitral valve prolapse. After establishing the diagnosis of IE in our patients, we looked at the presence of these risk factors, namely rheumatic fever, features of pre-existing cardiac disease such as exertional shortness of breath, orthopnoea, paroxysmal nocturnal dyspnoea, syncope, cyanotic spells, pedal oedema or right upper quadrant pain. We also checked for a history of intravascular intervention, surgery or intravenous drug use that might have predisposed to the development of endocarditis. A summary of each of these patients is presented, a relevant review of the literature, followed by a discussion.
Results
Of 1089 patients, five (0.46%) presenting to our department had a diagnosis of IE concluded, and are summarized below. During the study period, there were 86 other cases of IE admitted to our institution, mainly in the Cardiology Department. The most common presentation of our patients with IE was pyrexia of prolonged duration (>6 weeks), followed by embolic episodes leading to neurological manifestations. The cases described were suspected to have a rheumatologic disorder and were hence referred to us.
Case 1: IE mimicking seronegative rheumatoid arthritis (RA)
A 63-year-old woman presented with flare-up of seronegative polyarthritis affecting small and large joints of upper and lower limbs for 3 years, for the past 3 months. She had active arthritis involving shoulders, right elbow, right wrist, knees and ankles. Her Disease Activity Score for Rheumatoid Arthritis (DAS28) was 6.48, suggesting active disease. Acute phase reactants were elevated: the erythrocyte sedimentation rate (ESR) 75 mm/h, and serum C-reactive protein (CRP) 14.2 mg/dL. A full blood count revealed a microcytic hypochromic anaemia, with a drop in haemoglobin (Hb) from 12 to 7.3 g/dL over 1 month; upper and lower gastrointestinal tract endoscopy were normal. The white cell count (WCC) was 12,900/mm3 and platelet count (Plt) 143,000/mm3. A hand radiograph showed only erosions and decreased joint space in both first carpometacarpal joints (owing to coexistent osteoarthritis). Over the next 3 months, her joint symptoms were unresponsive to steroids, methotrexate and leflunomide in combination. She was admitted with vomiting, malaena and pancytopenia (Hb 6 g/dL, WCC 2140/mm3, Plt 66,000/mm3), likely drug induced. Two blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA). An echocardiography showed a 15 × 14 mm vegetation attached to the septal leaflet of the tricuspid valve with moderate tricuspid regurgitation. After establishing the diagnosis of IE, retrospective evaluation did not reveal any cardiovascular risk factors. She was treated with appropriate antibiotics, and her joint pains dramatically improved. Her pancytopenia also improved after stopping methotrexate and leflunomide. Nonetheless her bacteraemia persisted even after 6 weeks of injectable teicoplanin followed by oral linezolid. She subsequently developed backache; magnetic resonance imaging (MRI) of the dorsal spine revealed spondylodiscitis with subligamentous spread, which worsened clinically and radiologically despite antibiotics. She was thus referred for neurosurgical management.
Case 2: IE mimicking anti-neutrophil cytoplasmic antibody (ANCA)-associated small vessel vasculitis (AASV)
A 34-year-old man presented with fever for 8 months, 6 kg weight loss, abdominal pain for 5 months (initially in the right hypochondrium, later in the left hypochondrium, not related to meals or associated with malaena or haematochezia) and recurrent syncope with headaches for the past 2 months. He had a Marfanoid habitus, with a positive wrist-and-thumb sign, and an arm span greater than his height. Investigations revealed a thrombosed aneurysm in the jejunal segment of his superior mesenteric artery; urinalysis showed haematuria, granular casts and proteinuria with a protein:creatinine ratio of 1.1 on a 24 h timed urine collection (ultrasound scan showed no urinary stones). ESR was 85 mm/h, CRP 4.14 mg/dL. Anti-proteinase-3 (PR3) antibody was positive (>300 au/mL). Granulomatosis with polyangitis (GPA) was the clinical diagnosis, although he did not fulfil classification criteria. 5 His aneurysm could be explained by underlying Marfan’s syndrome. Echocardiography was normal. Renal biopsy could not be done owing to financial constraints. He was thus empirically treated with intravenous cyclophosphamide as per the European Vasculitis Study Group (EUVAS) regimen 6 with steroids in tapering doses, and azathioprine added for maintenance. He improved symptomatically, although haematuria persisted.
While still taking low dose oral steroid and azathioprine, he presented 1 year later with 6 kg weight loss over 6 months, and abdominal pain in the right hypochondrium with intermittent fever for the past month. Examination revealed petechiae in the palpebral conjunctivae. The CRP was elevated (12.3 mg/dL), hence a relapse of AASV was considered. By this time, though, anti-PR3 titres had become undetectable; however haematuria still persisted. Two blood cultures grew methicillin-sensitive Staphylococcus aureus (MSSA); echocardiography showed a large mobile vegetation in the posterior mitral leaflet with mitral stenosis and mitral regurgitation. He had no history of prior cardiovascular risk factors. With injectable cloxacillin over a period of 6 weeks, his fever subsided. He developed a mycotic radial artery aneurysm 3 weeks subsequently. Two weeks after stopping his course of antibiotics, his fever recurred; though blood cultures were sterile, repeat echocardiography showed persistent vegetations as before. He was thus referred for cardiovascular surgical management.
Case 3: IE mimicking pulmonary-renal syndrome
A 25-year-old woman presented with spontaneous abortion 2 months previously, followed by fever for the same duration (up to 39.4°C), with exertional shortness of breath and mucopurulent expectoration (the latter subsiding after a few days). She was found to be profoundly anaemic (Hb 3.5 g/dL) though there had been no excessive bleeding following her abortion, neither menorrhagia nor gastrointestinal blood loss and had been transfused 4 units of packed red cells till her Hb rose to 8 g/dL. During the first month of her illness, for a period of 15 days, she had had swelling of the face, hands and feet which later subsided, but there was neither oliguria, abdominal swelling nor abdominal pain. For the whole past 2 months, she had complained of increased, diffuse, non-scarring hair loss, not associated with a scalp rash. In the previous 15 days, she had painful tongue ulcers, lasting a few days before spontaneously resolving. She had no rash, photosensitivity, cheek or palatal ulcers, photosensitivity, Raynaud’s symptoms or arthralgia. She never had a foul-smelling vaginal discharge. She had been treated with colistin and metronidazole; owing to persistent fever and shortness of breath, she was referred to our hospital.
Examination revealed a tachycardia (110/min), moderate pallor and diffuse alopecia; blood pressure was 130/80 mmHg. Chest auscultation revealed bilateral rhonchi. The ESR was 90 mm/h and CRP 5.68 mg/dL. Peripheral blood picture showed neutrophilic leucocytosis (WCC 11,900/mm3, neutrophils 88%), Hb 8 g/dL, normocytic hypochromic, Plt 255,000/mm3. The Coombs test was negative. Urine examination showed proteinuria and haematuria. Serum creatinine was 61.9 µM, serum albumin 39 g/L. Chest radiographs showed heterogeneous shadows in both lower lung fields (Figure 1). The pulmonary-renal syndrome, secondary to systemic lupus erythematosus (SLE) was considered, in view of alopecia, tongue ulcers and active urinary sediments. The drop in Hb level, necessitating blood transfusion, was attributed to pulmonary haemorrhage.
Chest X-ray showing heterogeneous lung shadows in both fields.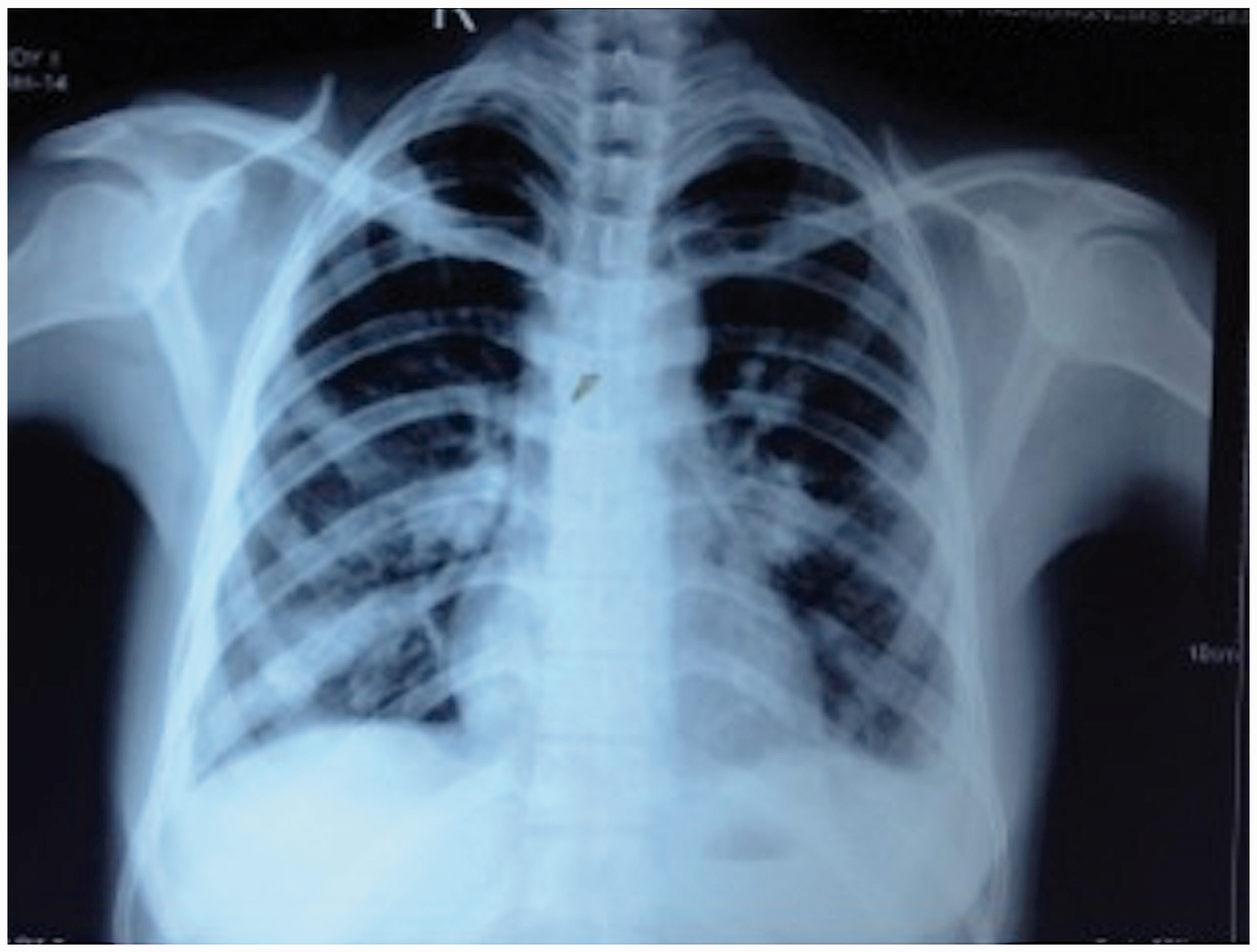
Investigations revealed negative antinuclear antibody (ANA), ANCA and double-stranded DNA antibody; and serum complements (C3, C4) were normal. A thoracic CT scan revealed bilateral pleural effusions, and pulmonary consolidation in a peribronchovascular and subpleural distribution with mild bronchiectasis (Figure 2). Echocardiography revealed a large vegetation attached to the anterior tricuspid valve leaflet causing severe tricuspid regurgitation. A diagnosis of right-sided endocarditis, possibly a consequence of septic abortion, with pulmonary-renal presentation was made. Repeated blood cultures, both aerobic and anaerobic, were negative, due to multiple prior antibiotics. After establishing the diagnosis of IE, retrospective evaluation for cardiovascular risk factors was negative. She was treated with injectable cloxacillin, and referred to a primary care hospital to complete a 4-week course of antibiotics.
CT scan thorax showing bilateral pleural effusion, airspace consolidation in peribronchovascular and subpleural distribution with mild bronchiectasis, and mild to moderate bilateral pleural effusion.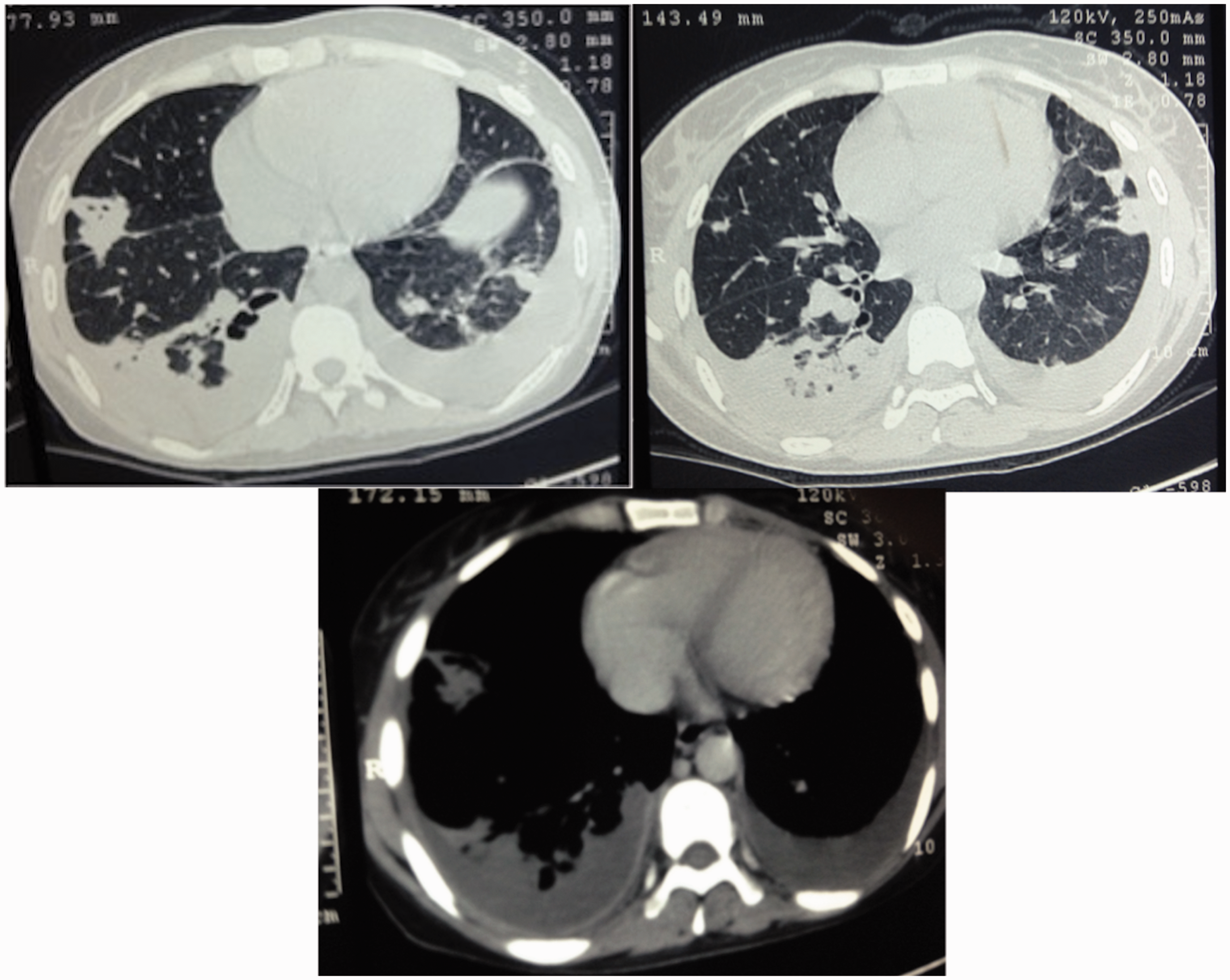
Case 4: IE presenting with acute polyarthritis, fever and bullous cutaneous lesions
A 49-year-old woman presented with fever for 8 days, with recurrent vomiting and painful swelling of small and large joints of upper and lower limbs, starting 2 days after the onset of fever. She had a bullous skin rash over the extensor surface of the elbows and toes, coinciding with onset of polyarthritis, which had subsequently desquamated. She was not sexually active, and had no vaginal discharge. She was hypertensive (170/90 mmHg) with mild pallor, the rash described and tenderness and swelling of elbows, wrists, left side metacarpo-phalangeal joints, right knee and both ankles.
Investigations showed dehydration, a serum creatinine of 229 µM, normalising after admission (53 µM). She had mild anaemia (Hb 10 g/dL, anisocytic with hypochromia), leucocytosis (WCC: 12,600/mm3 with neutrophils 71%) and low Plt (110,000/mm3). Urine showed a mild haematuria. Fever with acute polyarthritis and bullous skin eruption led us to consider gonococcal arthritis; 7 however, the fact that she was not sexually active and had no vaginal discharge ruled this out. In view of her microscopic haematuria with an acute febrile illness, another possibility was IE. Echocardiography showed a vegetation on the aortic valve, confirmed on transoesophageal echocardiography as a papillary fibroelastoma of the aortic valve complicated by endocarditis. After establishing the diagnosis of IE, retrospective evaluation for cardiovascular risk factors was negative. Blood cultures grew MSSA and Pseudomonas, and appropriate antibiotics were commenced. Her polyarthritis improved markedly with non-steroidal anti-inflammatory drugs and she was discharged to complete the course of antibiotics at a primary care hospital.
Case 5: IE presenting as SLE
A 31-year-old man was admitted with fever for 6 weeks. Initial evaluation had shown progressive thrombocytopenia (nadir: 12,000/mm3) with leucopaenia (nadir: 2800/mm3, neutrophils 45%, lymphocytes 43%) and liver dysfunction (AST and ALT initially 2330 and 1697 U/L, improving to 49 and 94 U/L, respectively). Serology for HIV was negative. In view of dengue antigen positivity, he was treated symptomatically and improved. However, his fever recurred, associated this time with a cough and minimal mucoid expectoration. He had lost 12 kg in weight. He was evaluated by several physicians; since no cause of fever could be determined, he was referred as a case of systemic lupus erythematosus (SLE).
Examination revealed mild pallor and splenomegaly. Investigations showed an anaemia (Hb 7 g/dL, with a macrocytic peripheral blood picture), WCC 5500/mm3 with a normal differential count, Plt 97,000/mm3. ESR was 120 mm/h, and CRP 11.1 mg/dL. Ultrasound as well as CT scan of the abdomen revealed splenic infarcts. Three blood cultures grew Enterococcus. Although he had no cardiac murmurs at admission, in hospital he developed early diastolic murmur in the aortic area suggestive of aortic regurgitation. Transoesophageal echocardiography revealed aortic valve vegetations with severe aortic regurgitation and moderate left ventricular dysfunction. After establishing the diagnosis of IE, retrospective evaluation for cardiovascular risk factors was negative. Despite appropriate antibiotic therapy, his clinical course deteriorated with supervening sepsis and acute kidney injury, from which he died 4 weeks later.
Discussion
Patient summary.

Case 1: IE mimicking seronegative RA
Our patient satisfied ACR/EULAR criteria for RA. 8 Odd for RA were lack of erosions on plain radiographs in spite of long duration of disease, and poor response to high dose steroids and multiple disease-modifying agents. Her arthritis had a dramatic response to antibiotics, suggesting it was due to bacteraemia, when it had remained refractory to immunosuppressive therapy. She had no fever, possibly because of immunosuppression. Whenever there are atypical features, even in a patient with inflammatory arthritis of significant duration, we advocate doing blood cultures and a screening transthoracic echo to minimise the possibility of missing out endocarditis.
Case 2: IE mimicking AASV
Although our patient did not satisfy criteria for GPA, 5 this was the best fit clinical diagnosis due to renal involvement, elevated ESR and CRP with ANCA positivity. Valvular involvement with vegetations is rarely described in AASV; 10 only 20 cases are reported in literature, and all but one had a diagnosis of GPA. Aortic regurgitation was the most common abnormality detectable. Vegetations and valvular thickening were notable features, more frequently found at presentation, but some cases developed these during the first year. Our patient most likely had endocarditis all along, due to aneurysm at the first visit (possibly mycotic aneurysm) and microscopic haematuria. Underlying Marfanoid features could have predisposed him to develop infective endocarditis. Transient ANCA positivity can be seen during infections. 11
Case 3: IE mimicking pulmonary-renal syndrome
The presentation with a pulmonary-renal syndrome usually entails differentials of AASV, Goodpasture’s syndrome, antiphospholipid antibody syndrome, SLE or viral haemorrhagic fever. IE causing pulmonary-renal syndrome has rarely been reported, mimicking Goodpasture’s syndrome 12 or granulomatosis with polyangiitis. 13 Right-sided endocarditis can mimic pulmonary-renal syndrome, and it is important to identify this because the treatment is antibiotics, compared to immunosuppression for immune-mediated pulmonary renal syndromes. Blood culture can be negative in up to one-fourth of patients with IE, 14 either due to prior antibiotic therapy or fastidious slow-growing organisms. 15 Renal disease in the setting of IE can be due to immune complex-mediated glomerulonephritis, drug-induced (interstitial nephritis or tubular necrosis) and sepsis-related renal failure.16,17
Case 4: IE presenting with acute polyarthritis, fever and bullous cutaneous lesions
IE can present as fever with polyarthritis. 9 Microscopic haematuria without significant proteinuria helped suspect endocarditis.
Case 5: IE presenting as SLE
Although he did not satisfy SLICC criteria, 18 this patient was referred as SLE in view of fever with pancytopenia. Both autoimmune and infectious disease can present as PUO.19,20 Further investigation proved IE in our patient. This case reiterates the need to consider infectious mimics of autoimmune disease.
Conclusion
IE can mimic a great variety of rheumatic diseases. Two of our patients described fulfilled classification criteria for rheumatic diseases. None had classical features of IE like Osler nodes, Janeway lesions or Roth spots. Review of the recent literature suggests a recent trend towards involvement of apparently normal valves with community-acquired infective endocarditis, 21 and except for case 2 (Marfanoid habitus) and case 4 (papillary fibroelastoma of the aortic valve), none of our other patients had evidence of underlying cardiovascular disease that could have conferred them with a greater risk of developing IE. None of our patients had history of prior cardiovascular risk.
Subtle clinical clues can help to suspect IE early, like microscopic haematuria without any other obvious cause. Whenever in doubt, multiple blood cultures with echocardiography are crucial in establishing a diagnosis. Even if transthoracic echocardiography is normal and clinical suspicion is high, it may be worthwhile doing a transesophageal study considering its high sensitivity. Diagnosing IE is imperative in a rheumatology ward, as patients with rheumatic disease often require immunosuppression. The distinction between the two is not always crystal clear, and the clinician has to rely on their judgement and experience.
Key messages
Infective endocarditis can mimic a wide variety of rheumatic diseases such as rheumatoid arthritis, small vessel vasculitis and systemic lupus erythematosus. Such patients may fulfil classification criteria for various rheumatic diseases, and often may have no prior history of cardiovascular disease or intravascular intervention that could predispose them to develop infective endocarditis. A high index of suspicion is required to distinguish rheumatic diseases from infective endocarditis, because use of immunosuppressive agents can worsen underlying systemic infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.