
Abstract
A cohort of 50 newly diagnosed patients with pulmonary tuberculosis was prospectively studied and compared with controls to assess and quantify their quality of life using the World Health Organization’s (WHO) Quality of Life (QOL)–BREF score before and after a Directly Observed Therapy Short (DOTS) course. It was concluded that health-related quality of life is impaired by tuberculosis and shows significant improvement with the DOTS treatment.
Introduction
According to the World Health Organization (WHO), tuberculosis (TB) is the second leading cause of death from a single infectious agent. In 2013, the WHO estimated 9 million cases of TB and 1.5 million deaths from TB globally. 1 In India, the Revised National Tuberculosis Control Programme (RNTCP) introduced the Directly Observed Treatment Short Course (DOTS) as its strategy in 1997. 2 This programme monitors the response to treatment of pulmonary tuberculosis on the basis of weight gain and the examination of sputum for acid fast bacilli. 2 In India, TB is associated with social stigma which not only delays the diagnosis but also prevents patients from adhering to treatment. 3 The chronic nature and social stigma associated affects the social and personal lives of patients leading to a diminished quality of life.
The WHO defines quality of life (QOL) as ‘the individual’s perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’. 4 Different instruments have been used to assess QOL. 5 The WHO QOL–BREF score has been validated as an assessment. A Hindi version has been used in many studies to evaluate QOL of tubercular patients in India.2,6,7 It has been used in various other diseases such as asthma, 8 hypertension, 9 depression 10 and cancer. 11
The purpose of this study was to assess the impact of sputum positive pulmonary TB on QOL and to assess how it changes with DOTS.
Material and Methods
Our prospective observational study was conducted in the Department of Pulmonary Medicine and the Department of Psychiatry of a tertiary care teaching hospital of northern India. The study was approved by the Institutional Ethics Committee. Patients with pulmonary TB of category I (Sputum for acid fast bacilli positive, new cases) aged 20–65 years, who registered at the DOTS centre of our Medical College, were included in the study. Patients who had other respiratory co-morbidity and with other known co-morbidities which can affect their QOL were likewise excluded, as were patients with multidrug-resistant TB. Pregnant and lactating mothers were likewise excluded. Controls were selected from the same area covered by the DOTS centre.
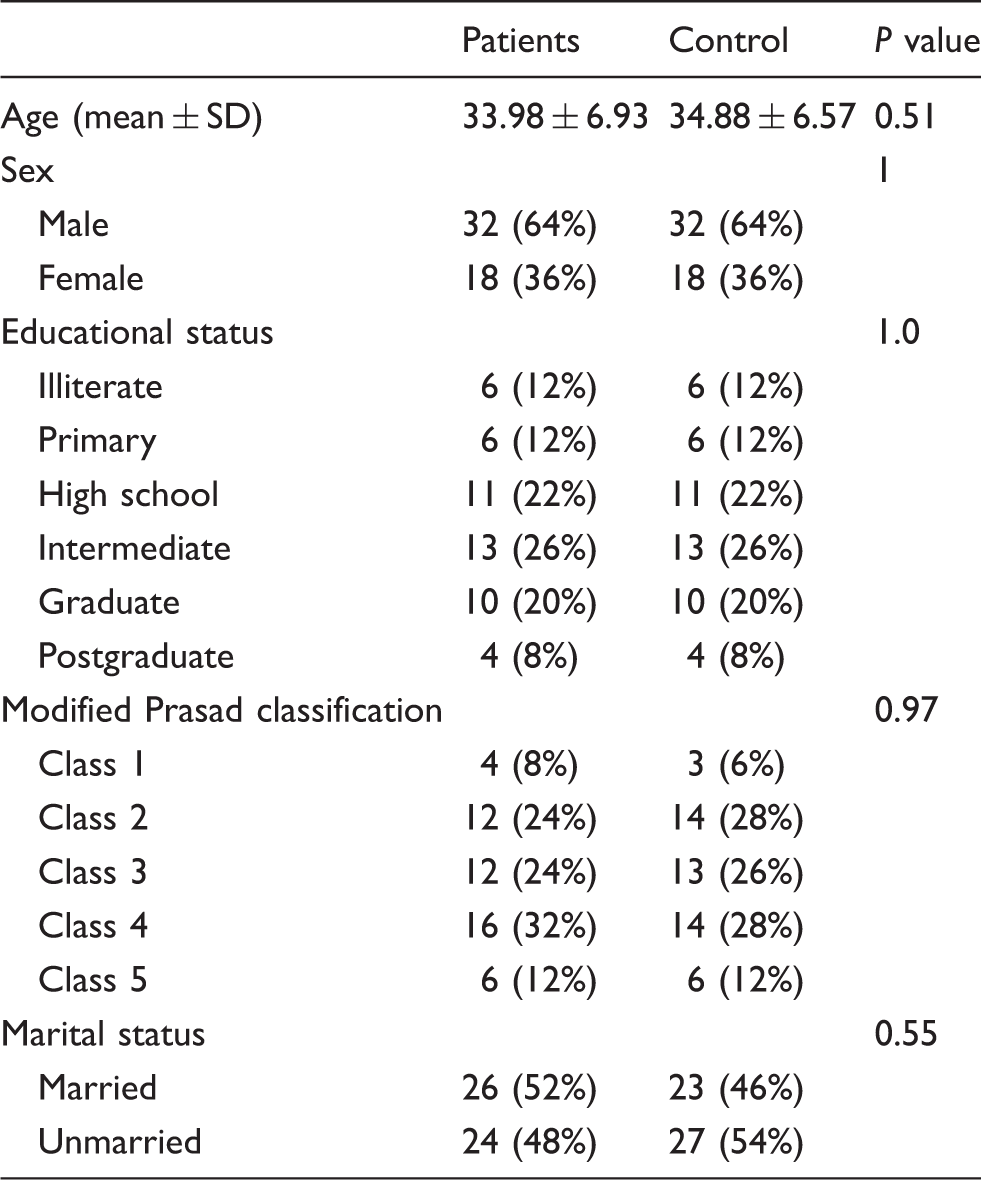
Fifty patients were selected and matched with 50 controls also selected from the same area catered for by the same DOTS centre. They were matched for age, sex, educational and socioeconomic status. Informed consent was taken from both controls and patients. Modified Prasad classification was used to assess the economic status of the study population. 12
All patients were treated with DOTS category 1 treatment. This consists of a 2-month intensive phase comprising rifampicin, isoniazid (INH), pyrazinamide and ethambutol, followed by 4 months of a continuation phase comprising rifampicin and INH. The entire drug was given on an alternate day basis.
Socio-demographic characteristics of all patients and controls were recorded. The Hindi WHO QOL–BREF questionnaire was used. It has four domains: physical health; psychological health; social relationships; and environment. These domains constitute 24 questions, scored on a 5-point Likert scale (example: 5, very satisfied; 4, satisfied; 3, neither satisfied nor dissatisfied; 2, dissatisfied; and 1, very dissatisfied). All the domain scores are scaled in a positive direction. In addition, there are two items examined separately; scores are added up to obtain an overall QOL value. High scores indicate a better QOL. The physical domain has questions related to daily activities, treatment compliance, pain and discomfort, sleep and rest, energy and fatigue. The psychological domain assesses positive and negative feelings, self-esteem, body image and physical appearance, personal beliefs and attention. The social relationship domain covers personal relationships, social support and sexual activity. The environmental domain explores physical security, financial resources, health and social care and their availability, opportunities for acquiring new information and skills, and opportunities for and participation in recreation and transport. In order to compare domain scores the WHOQOL-BREF scores were converted into scores from 0 to 100, with a lowest score of zero and a highest of 100. Patients were asked to complete the WHO QOL–BREF questionnaire at 0, 2 and 6 months of therapy. Controls were also interviewed using the same questionnaire.
Data were analysed using Microsoft Excel version 2007. Quantitative variables were summarised by mean and standard deviation, and categorical variables were summarised by frequency (percentage). Mean scores of patients at different stages of treatment were compared by one-way ANOVA test. QOL scores in the control group were compared with the same in patients of TB at three different stages (0, 2 and 6 months of treatment) by t-test. P value less than 0.05 was considered as statistically significant.
Results
Socio-demographic characteristics of patients and control.
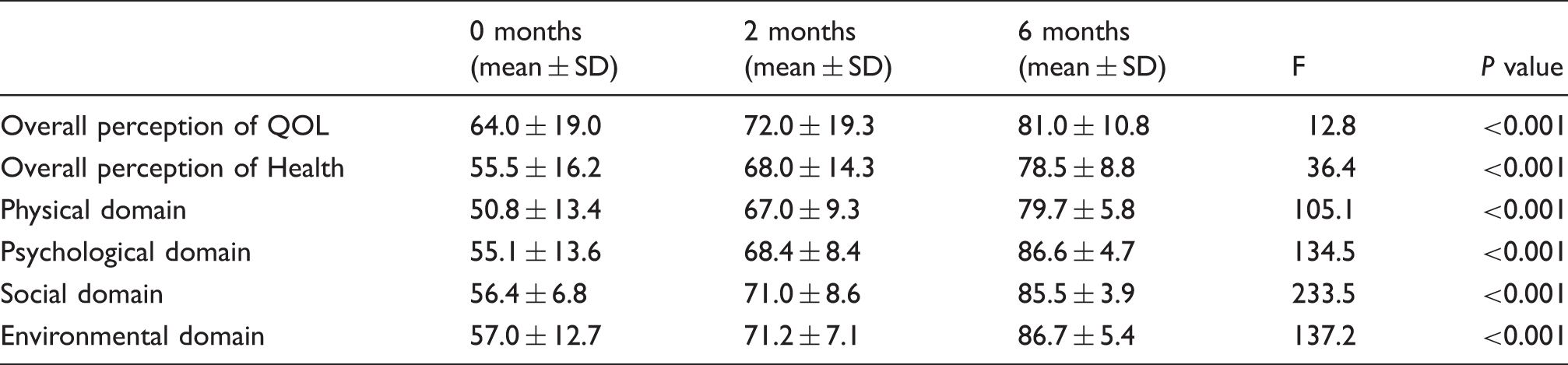
WHO QOL–BREF scores at the various stage of treatment with anti-tubercular drugs.
Comparison of WHO QOL–BREF score between patients and control at various stages of treatment.
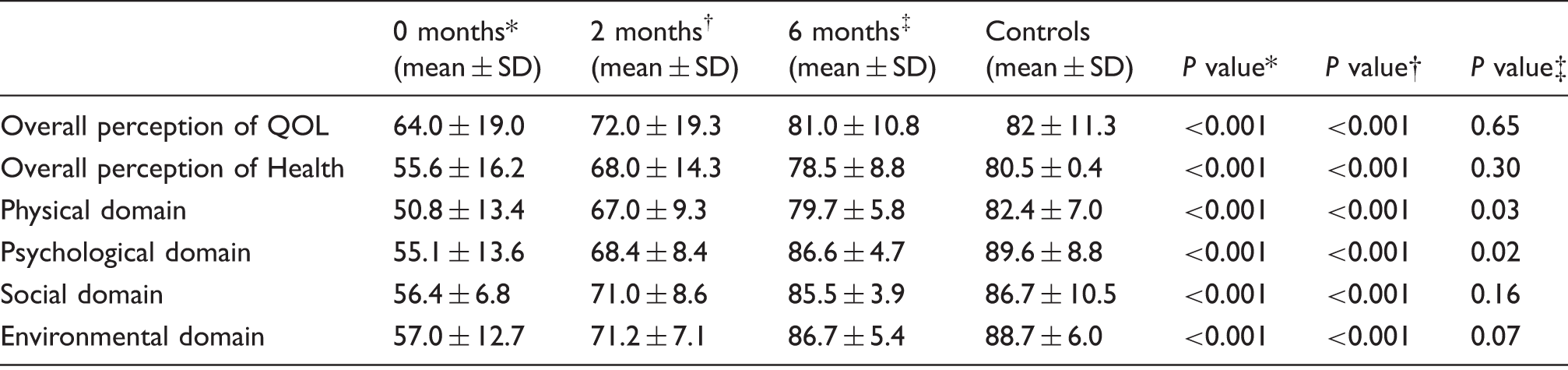
Comparison between 0 months and controls.
Comparison between 2 months and controls.
Comparison between 6 months and controls.
Discussion
In spite of effective drug availability, TB remains a global health problem. TB itself along with its long-term treatment affects the QOL of patients.
TB patients de novo have significantly lower scores of QOL than controls, and the worst affected domain was the physical 2 whether tested by other scoring systems7,13,14 or in more affluent countries such as the UK and USA.15,16
The second most affected domain was the psychological. Aggarwal et al. state this to be so, particularly among those with more severe disease, women, villagers and patients with lower socioeconomic status. 7 Nonetheless a low mental score was more frequent than a low psychological score in China. 18
Social stigma associated with TB has a negative influence on QOL. 3 This is considered to be the reason for the affected social domain of the patients. Social stigma associated with TB makes the sufferer hide the disease from society and thus reducing community participation and sometimes delay in diagnosis and treatment. In a variety of studies, in different settings and using different instruments, subjects with active TB consistently reported poorer health-related QOL. 5
At 2 and 6 months of onset of treatment with a universally positive response to treatment, there was significant improvement in all domains and the overall perception of QOL. However, scores after 2 months of treatment (i.e. after the completion of the intensive phase) continued to be lower than in controls. Our results were similar to others.2,7,13,14 However, Chamla 18 found an initial decrease in physical and mental scores as compared to baseline. Chung and Li found scores then increased after 6 months of treatment. Adverse drug reactions and unemployment were the suggested reason for the initial decline in QOL scores. 19
The overall perception of health and QOL showed significant improvement at the end of treatment. It, however, remained low compared to controls, though this was not significant. A possible reason may be due to alleviations of signs and symptoms. 17
Physical, psychological, social and environmental domains showed significant improvement at the end of the treatment as compared to base line, but remained lower than controls. Balgude et al. 14 predicted that assessment of the scores at the end of 6 months of therapy would have yielded better results. In our study the scores continued to remain low even after the end of 6 months, as found by Atif et al. 20
Limitations
Our study was conducted in the limited cohort of a single DOTS centre. No patients of category II DOTS treatment were included, nor were patients taking treatment outside.
Conclusion
Not surprisingly, TB patients have a poorer health-related QOL than controls. While there is significant improvement with DOTS treatment, none reach control levels even after completion of DOTS. This underlines the need for full rehabilitation, even after finishing the standard drug treatment regime.
Footnotes
Declaration of conflicting interests
The author(s) declared no no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.