
Abstract
Tuberculosis (TB) and malignancy are among the most important current global health problems. Many authors suggest that their coexistence is a chance association owing to their high prevalence. There is, however, enough evidence that one condition may predispose the other. In our retrospective report of two cases, TB in draining lymph nodes was discovered incidentally on histopathology, following surgical resection for malignancy. The possibility of coexistent lesions, especially in regions endemic for TB, mandate a detailed histopathological examination to prevent the chances of diagnostic failure and thus therapeutic error.
Keywords
Introduction
Tuberculosis (TB) is an important public health problem, being highly prevalent in low- and middle-income countries such as India. The incidence of cancer also shows a rising trend; thus the two may readily coexist. While this may simply be due to their high prevalence, evidence suggests one condition may predispose the other. A chronic inflammatory condition such as TB may initiate a sequence of metaplasia and dysplasia resulting in neoplasia. Moreover, cancer and its therapy may contribute to an immunocompromised state which may activate latent TB infection. 1
The concomitant presence of two diseases in one organ almost always poses a diagnostic and therapeutic challenge. Missing one of the diagnoses limits therapeutic success. We hereby present two cases of coexistent TB and malignancy in which TB was discovered incidentally following surgery.
Case 1
A 40-year-old man, known to have had laser excision of a laryngeal glottic squamous carcinoma (stage T1N0), presented with a recurrent lesion 5 months following surgery. Histology revealed a spindle cell carcinoma, which was treated by radiotherapy at a dosage of 68 Gy. Three months after completion of radiotherapy, he again developed hoarseness. There was no associated co-morbidity. An indirect laryngoscopy and subsequent flexible fibre optic laryngoscopy revealed a nodule involving the anterior commissure with restricted movement of the right vocal cord. No cervical lymph nodes were palpated. Magnetic resonance imaging (MRI) of the neck, however, revealed an irregular lobulated heterogeneous lesion with a nodular component projecting into the laryngeal lumen, compromising the airway. Multiple mildly enlarged lymph nodes were seen along the right carotid sheath at levels II, III and IV. Biopsy of the laryngeal growth confirmed recurrent spindle cell carcinoma. On immunohistochemistry, tumour cells were positive for cytokeratin (CK), smooth muscle actin (SMA), CD-34, S-100 and negative for desmin. A total laryngectomy with selective right neck dissection was performed. Postoperative histopathological examination confirmed the spindle carcinoma (pT3N0) with focal myxoid and neural differentiation involving the glottic region extending to the subglottic. The lymph nodes showed necrotising granulomata and stains for acid fast bacilli were positive. Lymph nodes were free of metastasis. Nested PCR assay for Mycobacterium tuberculosis performed on the paraffin embedded lymph node tissue was positive. The postoperative recovery was uneventful and antitubercular treatment was commenced.
Case 2
A 65-year-old man presented with abdominal pain, with difficulty in eating and constipation for the previous 8 months. There was no history of fever or previous record of TB. Clinical examination revealed an abdominal mass extending from the left hypochondrium to the lumbar region. An abdominal computed tomography (CT) scan revealed a large enhancing mass along the greater curvature of stomach measuring 12.8 × 9.4 × 7.7 cm. Multiple enlarged perigastric lymph nodes were also seen. The findings were suggestive of a gastrointestinal stromal tumour (GIST). The patient underwent a subtotal gastrectomy with partial colectomy and resection of a portion of jejunum as the tumour was adherent to both these structures. Grossly, the tumour was located along the greater curvature, extending from inner gastric wall to the serosal aspect of the adjacent colon and was solid, firm and grey-white in colour. Several lymph nodes isolated from the greater omentum showed necrosis. The segment of jejunum had two diverticula of 3.5 cm and 2.5 cm in diameter. Histologically, a spindle cell tumour with mild to moderate pleomorphism with minimal mitotic activity (2–3/50 high power field) was demonstrated. Associated lymph nodes had epithelioid cell granulomatas with Langhan’s giant cells and positive acid fast bacilli on Zeihl Neelsen staining (Figure 1). A diagnosis of GIST with tubercular lymphadenitis and jejunal diverticulosis was proffered.
Photomicrograph from case 2 showing (a) spindle cells arranged in fascicles showing moderate pleomorphism (Haematoxylin and Eosin [H&E] × 400); (b) epithelioid cell granulomata in the lymph node [H&E] × 100); inset shows AFB on ZN stain × 1000.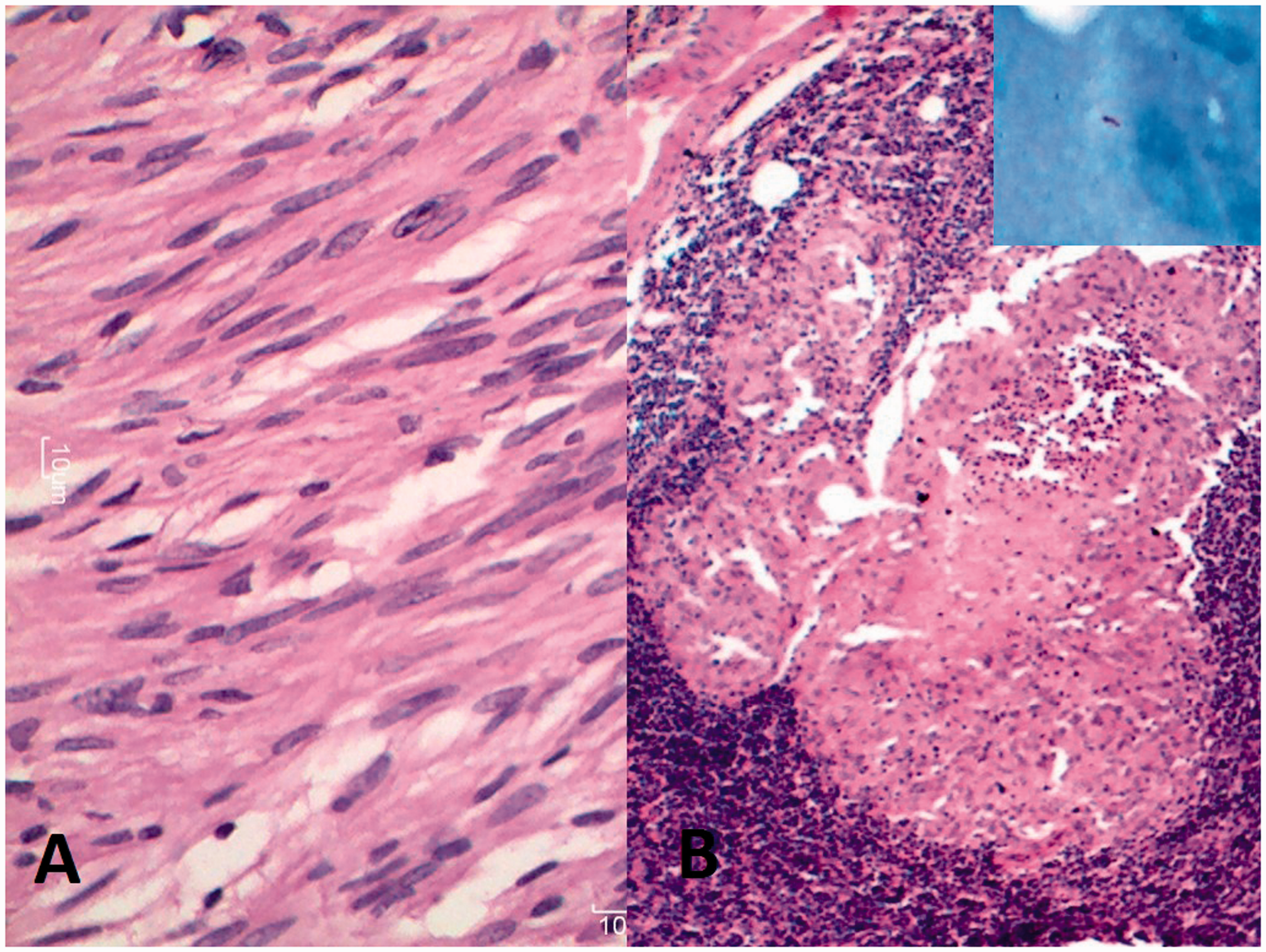
Discussion
TB and malignancy are among the most important current global health problems. According to Kaplan et al., 2 concomitant TB and malignancy have been reported most commonly in Hodgkin’s lymphoma followed by sarcoma, leukaemia and lung cancer. Uncommonly, TB has also been found with carcinoma of the breast,3–5 colon,6,7 uterus, bladder, larynx, tongue and mouth,8–11 stomach12–14 and prostate. Both the cases reported in this series showed TB coexisting with solid organ malignancies.
The pathophysiological and clinical implications of such coexistence have not been explored completely. Although newer imaging modalities and laboratory tests help in the diagnosis, the ability of TB and malignancy to mimic each other clinically presents a serious challenge. 1 Further, if TB is masked by malignancy, the therapy instituted for the latter may cause immunosuppression and thereby result in dissemination of TB with fatal results. 1 Finally, the presence of TB in lymph nodes may lead to drastic over-staging of a cancer. 3
Cytology and histopathology should also be interpreted with utmost caution as there can be varied atypical presentations owing to immunosuppression. For example, necrosis and inflammatory cells alone may be found without granulomata in extrapulmonary TB. 15 Furthermore, granulomatous inflammation may rarely be seen in lymph nodes draining a primary tumour, both with or without the presence of metastasis. Granulomatous reaction may be due to foreign body reaction to tumour necrosis, therapy-related (including BCG inoculation) or systemic disease such as sarcoidosis. Therefore, a careful scrutiny of granulomatas is important to prevent under-diagnosis of metastatic disease or over-diagnosis of TB. The prognostic significance of granulomata is currently unknown. 16 Moreover, fine needle aspiration from such problem cases may be misleading, especially if only one set of cells is commented upon. The need for multiple attempts should be stressed upon for all palpable lumps. 4
The polymerase chain reaction test (PCR) for TB should be used in dubious cases. In addition to histological examination, microbiological evaluation (stain and culture for M. tuberculosis) should be conducted to avoid missing out on the diagnosis. 1
In cases where TB was the primary diagnosis, the discovery of cancer may be delayed due to masking by a tubercular lesion, and this suggests that in patients having a tubercular lesion who show little improvement of symptoms despite antituberculous therapy, coexisting cancer should be suspected by the clinician before suspecting multi-resistant TB. 17
The latent period for the diagnosis of cancer in a patient with inactive pulmonary TB is somewhat shorter if both the diseases are located in different areas of the lung. However, when cancer is associated with active TB and the two coexist in the same lobe, much more time elapses before the cancer is diagnosed. The advances in imaging techniques have increased the accuracy in the diagnosis of lung cancer. 17
Tubercular lymphadenitis is the most frequently encountered form of extrapulmonary TB which may involve cervical, axillary or inguinal lymph nodes. However, primary axillary tubercular lymphadenitis is extremely uncommon in adults and can be due to either retrograde spread from the mediastinal nodes or haematogenous spread from a subclinical focus, not detected by routine investigations. 4
HIV-positive individuals have a substantially higher risk of some types of cancers (cervical cancer, non-Hodgkin’s lymphoma and Kaposi sarcoma) compared with uninfected people of the same age. Moreover, HIV infection is one of the most important risk factors for progression to active TB disease. 18 The collision of these three world health pandemics will have a devastating impact in resource-limited settings such as India. Therefore, clinicians ought to be aware of such a possibility in HIV-positive individuals.
Interestingly in our two cases, TB coexisted with spindle cell tumours. This association has not specifically been highlighted before, although TB may mimic the latter. 12
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.