
Abstract
The spectrum of liver disease among HIV-infected patients is changing. In the era of antiretroviral therapy, opportunistic infections are diminishing and deranged liver function appears to be due usually to drug-induced liver injury, alcohol, non-alcoholic steatohepatitis (NASH) or chronic hepatitis B. To test this hypothesis, 98 HIV-positive patients with deranged liver function were compared with matched HIV-positive patients with normal liver function and likewise matched HIV-negative patients with normal liver function tests.
Keywords
Introduction
Hepatobiliary diseases make a major contribution to the morbidity and mortality of HIV-infected people. 1 With the introduction of antiretroviral treatment (ART), HIV-infected patients are experiencing longer life expectancy and some reports suggest liver disease as the leading cause of death. 2 In these patients, hepatic abnormalities are attributed to chronic viral hepatitis (B and C) as co-infections, presumably owing to shared routes of transmission. 3 Opportunistic pathogens (viz. cytomegalovirus) and tumours (viz. lymphoma and Kaposi’s sarcoma) were common causes of hepatobiliary derangement in the past, but these are diminishing. 4 Tuberculosis is, however, increasingly prevalent in low- and middle-income countries (LMICs) in HIV-infected patients and this may itself result in liver function derangement. Elevation of hepatic enzymes may also be the result of multiple factors such as chronic alcohol consumption, drug addiction, lipid-lowering drugs, ART itself or hereditary diseases. 5 In addition, it has been proposed that HIV itself causes direct damage to hepatocytes. 6 Furthermore, with a rising incidence of obesity, reports have suggested that non-alcoholic fatty liver disease (NAFLD) may be important both in the general population and in HIV-infected patients.7,8 Information from the latter countries is normally based either on liver histology or clinical diagnosis. 9 The study was therefore carried out incorporating both clinical and histological parameters for the evaluation of deranged liver function in HIV-infected patients.
Methods and Materials
This prospective cohort study was conducted at a tertiary care centre in Mumbai. The study population consisted of confirmed HIV-infected patients with abnormal liver biochemical tests attending from December 2013 to June 2014. Patients with abnormal liver enzymes (levels >1.5 the normal range), either symptomatic or asymptomatic, taking ART or not, were included. HIV-positive patients aged below 18 years and pregnant women were excluded. Equal numbers of age- and sex-matched HIV-positive and HIV-negative patients with normal liver function as controls were taken from the general outpatient clinic (Figure 1). All participants provided written informed consent, and the study was approved by the local Institutional Ethics Committee.
Flow diagram of study.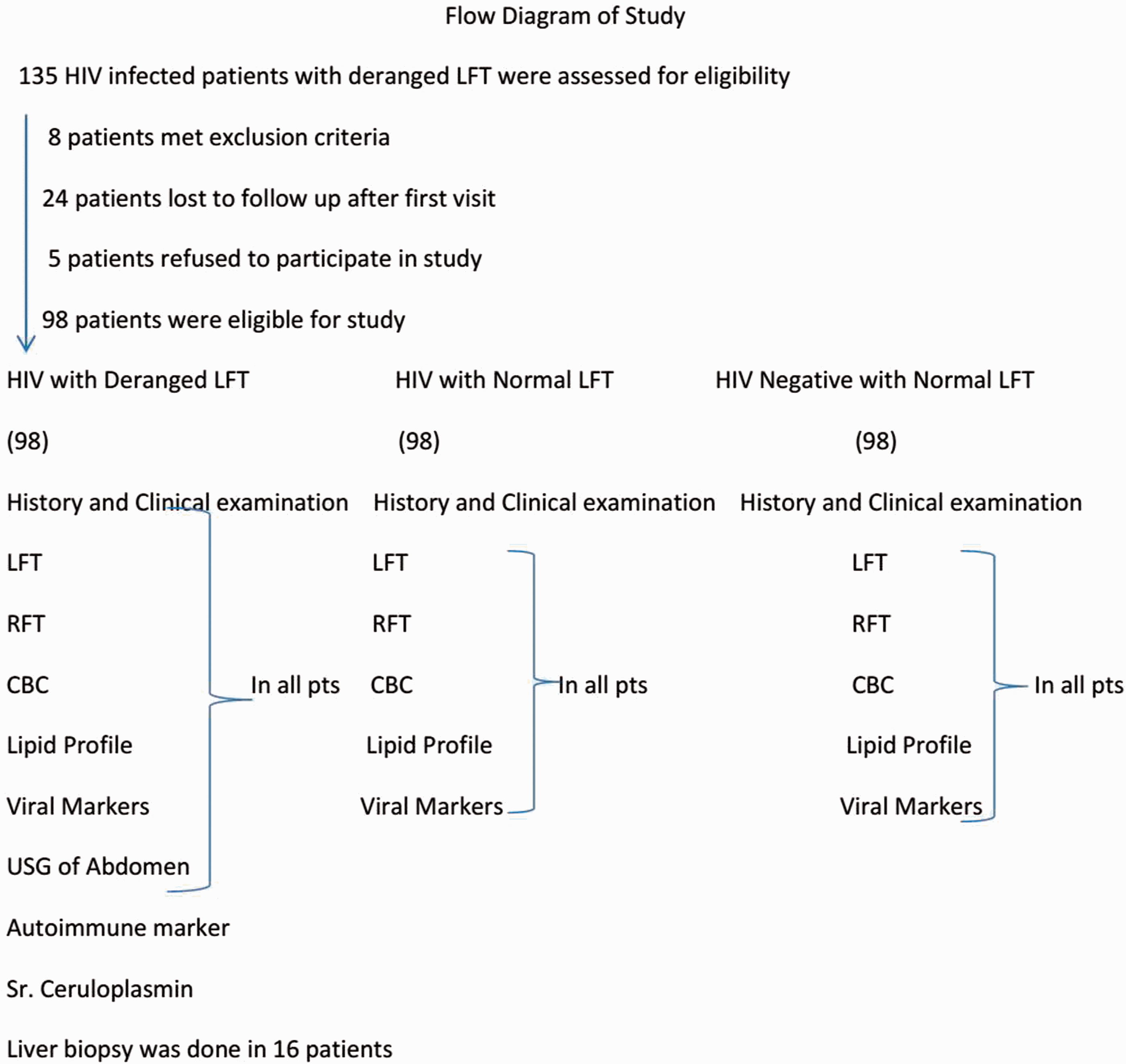
Demographic details of all patients were recorded. Clinical history included presenting complaints of recent illness, duration of HIV-positivity, details of alcohol ingestion, duration of ART, anti-tubercular, diabetic, anti-hypertensive and lipid-lowering medication were recorded. Alcoholic liver disease was excluded as cause of disease if intake was <30 g/day and <150 g/week for men or <20 g/day and <100 g/week for women.10,11 A detailed clinical examination was performed in all patients. The body mass index (BMI) was calculated as kg/m2. A recent CD4 count, the type of antiretroviral drugs used and the temporal relationship between symptoms and any medication received was recorded. Drug-induced liver injury (DILI) was diagnosed based on such temporal relationship and depending on resolution of liver function derangement after stopping the culprit drug and exclusion of other causes of liver injury. 12 All patients had full blood count (FBC), fasting blood sugar, levels of serum transaminases (ALT and AST), bilirubin, alkaline phosphatase (ALP), total protein, albumin, prothrombin time (PT), international normalized ratio (INR), fasting serum total cholesterol, serum triglyceride, hepatitis B surface antigen (HBsAg), hepatitis C antibody (anti-HCV) and renal function tested. Likewise, all had abdominal ultrasonography of the hepatobillary system performed. In selected patients, hepatitis B core antibody (total anti HBc), anti-nuclear antibody, anti-smooth muscle antibody, anti-liver-kidney microsome antibodies, serum cerulopalsmin and 24 h urinary copper were also tested. In patients with HBsAg or anti Hbc positive status, tests for HBV DNA and HBeAg were performed. Liver biopsy was carried out when the cause of deranged liver function was not identified after virological, radiological and immunological work-up. The AST/platelet ratio index (APRI) was calculated using the formula AST level/reference value/platelet count (×109/L) × 100.
Statistical analysis
The Mann–Whitney test was used for comparison between the two main HIV-positive groups. One-way ANOVA was used in analysis of quantitative data between all three groups if data passed a ‘Normality test’ and by the Kruskal–Wallis test if data failed. Associations among variables in patients who died compared with those who improved were defined with the help of Binary Logistic Regression. A P value <0.05 was taken as significant. Statistical analysis was done using SPSS Version 16.0 for Windows. 13
Results
Comparison of various parameters among three study groups.

BMI, body mass index; WBC, white blood count.
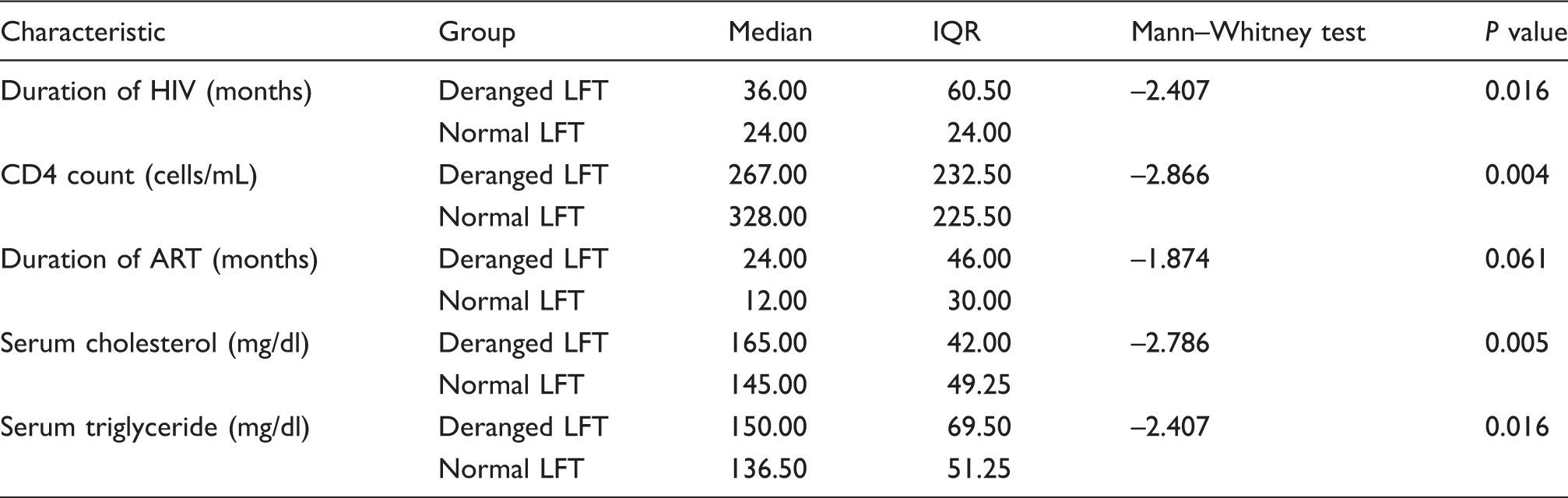
Comparison of various parameters in HIV patients with deranged LFT and normal LFT.
Distribution of lipid profile and liver enzyme as per ART regimen.
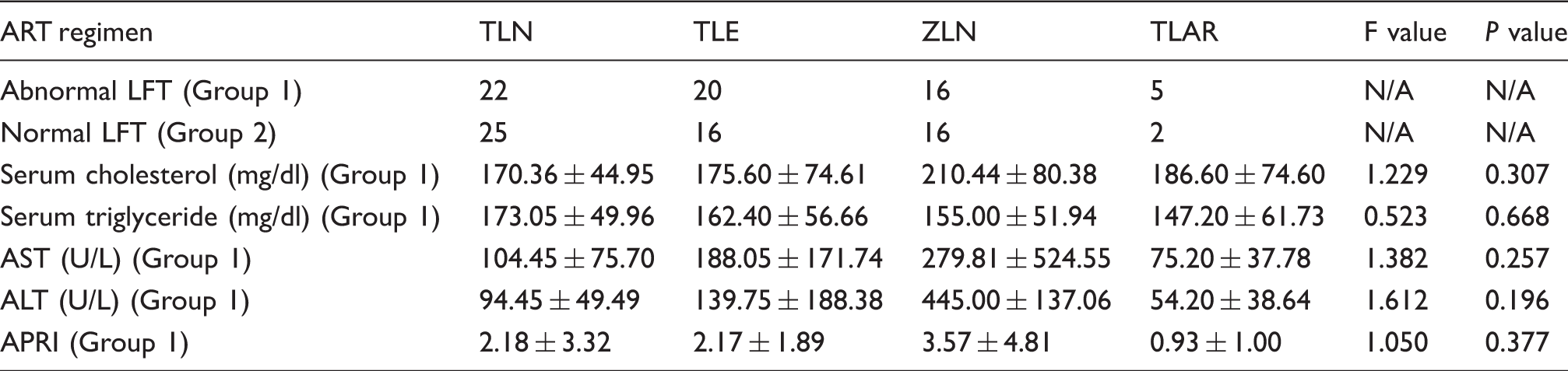
ALT, alanine aminotransferase; APRI, AST platelet ratio index; AST, aspartate aminotransferase; N/A, not applicable; TLAR, Tenofovir (TDF) + Lamivudine (3TC) + Atazanavir (ATV) + Ritonavir (RTV); TLE, Tenofovir (TDF) + Lamivudine (3TC) + Efavirenz (EFV); TLN, Tenofovir (TDF) + Lamivudine (3TC) + Nevirapine (NVP); ZLN, Zidovudine (AZT/ZDV) + Lamivudine (3TC) + Nevirapine (NVP).
The most common causes of liver dysfunction in decreasing order were: DILI, either anti-tubercular (ATT) or ART (29%), chronic hepatitis B (18%), alcoholic liver disease (11%) and NASH (7%). Other causes were rare. Among the 98 patients with deranged liver function, 26 were HBsAg-positive, nine were hepatitis B e antigen (HBeAg) positive and 23 patients had detectable HBV DNA (mean 2.1 × 107). Of the 26 HBsAg-positive patients, five had other factors present such as excessive alcohol consumption and drugs as contributing factors. Contrary to reports from elsewhere, hepatitis C was seen in only two patients. Among 16 patients who underwent liver biopsy, seven had normal liver histology, five had steatohepatitis, two had granuloma and two were found to have cholestasis. The cause of liver disease was unexplained in 12 patients, of whom seven had normal liver histology and five recovered to normal liver function during their evaluation. Hepatomegaly was found on ultrasonography in 50% of patients who underwent liver biopsy. During the mean 6-month follow-up period, eight patients (8.2%) died. Logistic regression analysis for outcome showed that age, CD4 count, total serum bilirubin, AST, ALT, APRI, serum protein, serum creatinine, haemoglobin and white blood cell count were not associated with improvement.
Discussion
Liver diseases in HIV-infected individuals is an emerging issue and there is heterogeneity in its aetiology in different parts of the world. The aetiology of liver diseases is unexplained in nearly 50% of asymptomatic patients in some recent studies. Liver diseases accounts for 10–18% of observed deaths and ranks as one of the first cause of death in HIV patients. 14 Heterosexual transmission accounts for 84.7% in LMICs such as India. 15 With increasing industrialization, injecting drug use is a major a risk factor for both HIV transmission as well as associated HBV/HCV co-infection. It also accounts for the higher prevalence of alcohol abuse and obesity leading to increased liver related death. A study from California, found that in HIV-infected persons, NAFLD was the most common cause of abnormal liver function (30%) followed by excessive alcohol use (13%), chronic hepatitis B (9%), chronic hepatitis C (5%) and more than one diagnosis in 10% of patients. Eighteen percent of patients were obese with a mean BMI of 25.8 kg/m2. However, despite having no evidence of obesity, we found a considerable prevalence of NASH (7%) among our HIV patients which mimics lean NASH seen in Asian countries. 16 In HIV–TB co-infected patients, evaluation of the cause of abnormal liver function is very challenging as it is difficult to differentiate between DILI and tuberculosis immune reconstitution inflammatory syndrome (TB-IRIS). Similar to DILI, TB-IRIS patients can present with jaundice after initiating ART. Histopathological findings which suggest TB-IRIS in liver tissue include large epithelioid granulomata which are again difficult to distinguish from tuberculous granulomata. A study from Tanzania reported that the incidence of DILI in patients on concomitant HIV and TB therapy was almost twice (i.e.10%) that of those treated with efavirenz-based ART only (5.9%). 17 The most common cause of deranged LFTs in our study was DILI (16% in ATT and 14% in ART). There was no statistically significant difference in the incidence of DILI among the various ART regimens although some antiretroviral drugs have propensity to cause DILI more frequently than others. Nucleoside agents may cause direct hepatotoxicity and steatosis due to inhibition of mitochondrial DNA polymerase-γ. 18
HIV-infected patients have been reported to exhibit an abnormal lipid profile which has correlation with CD4 counts. 19 Most studies have showed that triglyceride is increased in HIV patients compared to the general population. This increase is due to raised very low density lipoprotein levels (VLDL) and alteration in cytokine like interferon, interleukins and TNF. 20 The level of serum cholesterol has conflicting results in HIV patients. Generally cholesterol will decrease in advanced HIV disease and its level will increase after HAART treatment. 21 We found significantly high serum cholesterol and triglyceride in the deranged LFT group compared to the normal LFT group; this could explain the increased incidence of NASH in HIV-infected patients. Liver test abnormalities among HIV patients receiving protease inhibitors may be largely related to an increased lipid level, hence adequate control of lipid levels may be useful in preventing liver enzyme elevations and perhaps ongoing liver dysfunction among this patient population.
Haematological abnormalities are prevalent in HIV-infected patients which can cause hyperbilirubinemia (mainly indirect) and elevation of serum AST. Low haemoglobin in the HIV population was associated with a higher death rate in both the low CD4 and high CD4 groups and anaemia was independently associated with a higher mortality at 1 year of follow-up. 22 Similar findings in our patients indicate that as the immunosuppression worsens, the probability of illness due to liver disease increases. 23
The APRI >1.5 is a non-invasive marker of significant liver fibrosis in patients with HIV/HCV co-infection; 24 47% of our patients had APRI >1.5 and seven patients out of eight who died had APRI >1.5. Significant liver fibrosis by APRI score has been reported in 8% of HIV-mono-infected patients. 25 Diabetes mellitus and high HIV viral load were significant risk factors for fibrosis. While HBV/HCV co-infections are obvious causes of liver fibrosis, NAFLD and NASH are other emerging causes leading to chronic liver disease.
Liver test abnormalities may be transient in nature in up to 30% of the general population. 26 Liver histology is critical in the evaluation of abnormal liver tests, especially if the abnormality persists even after eliminating the offending aetiological factor. Initial studies on liver histology in HIV-infected patients revealed that infectious diseases were the most common cause of liver test abnormalities in LMICs. 27 There was a low prevalence of opportunistic infection in our study as most of the patients were on ART with an average CD4 count >310/mm3 and with good performance status. Consistent with a recent study from Africa, our results indicate that DILI due to ART is the most common cause of abnormal liver enzymes. 28 Two of our patients had HIV-induced papillary stenosis and one had nodular regenerative hyperplasia (NRH). The latter is a potential cause of non-cirrhotic portal hypertension in patients with HIV. It is being increasingly recognised among HIV-infected individuals as they experience increased longevity and longer exposure to medications. 29 Most NRH patients have normal liver enzymes and histopathological evaluation remains critical in excluding cirrhosis and other causes of portal hypertension. 30 Didanosine (DDI) has been strongly correlated with ART-associated NRH. Association with azathioprine (AZA), 6-mercaptopurine, 6-thioguanine, busulphan and cyclophosphamide has also been reported in recent studies. 31 The pathogenesis of NRH is believed to be related to the differential blood supply to the liver with areas of ischemia and compensatory hypertrophy which leads to the formation of hepatic nodules. 32
During 6 months of follow-up, eight of our patients (8.2%) died. Even though most of the deaths were in patients with alcohol-related liver disease (alcoholic hepatitis and cirrhosis), we did not find any significant association between various parameters and mortality. In a study from Switzerland, 14.5% deaths in HIV patients were from liver-related causes and predictors of mortality were latest CD4 cell count, age, intravenous drug use, HCV infection and active HBV infection. There was no relationship with duration of ART. 34
A strength of our study is the extensive evaluation of each case to identify the potential causes of liver disease in an HIV-infected clinic population. Patient evaluation included a detailed history with records of medication use and questionnaire of alcohol use, physical examination, laboratory tests, abdominal ultrasound and liver histology. Very few studies from LMICs have extensively investigated HIV patients with deranged LFTs. 33 There are some limitations in this study. It is hospital-based and the sample size of study population is relatively low with a follow-up of only 6 months. Hepatitis B core antibody was done in selected patients and occult hepatitis B could have been missed in a few patients. However, this is unlikely to affect our results, because none of the patients in whom Hepatitis B core antibody was not done had any other evidence of chronic liver disease.
Conclusion
We have demonstrated that DILI is the most common cause of abnormal liver tests in HIV-infected patients. Serum cholesterol and triglyceride levels are significantly elevated in these patients contributing to the rising incidence of NASH. Liver test abnormalities may be transient in nature in the HIV population, thus performing biopsy in selected patients after careful clinical assessment provides valuable information in clinically complex patients. This approach is more realistic and cost-effective in resource-limited nations rather than an aggressive approach of performing a biopsy in every patient for an evaluation of abnormal liver function. Even after such an approach abnormal LFT was unexplained in around 12% of our patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.