
Abstract

Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease with heterogeneous presentations. It is characterised by an autoantibody response to nuclear and cytoplasmic antigens. Multiple factors have been implicated which include genetic, ethnic, immunoregulatory and environmental factors as well as infectious agents of which viruses are the major culprits. 1
Case report
A 17-year-old girl presented with a 7-day history of fever and oliguria. There was no history of arthralgia, rash, haematuria, altered sensorium, convulsions, oral ulcers, alopecia or photosensitivity. Her family history was unremarkable. On examination she had tachypnoea, fever, anaemia, anasarca, bilateral basal crepitations in the chest and splenomegaly.
Investigations on admission confirmed the anaemia (Hb: 8.6 g/dl), a normal white count (4100/mm3), thrombocytopaenia (platelets: 19,000/mm3), normal clotting (INR: 1.1), raised erythrocyte sedimentation (ESR: 55 mm/1st h), abnormal renal function (urea: 29.6 mmol/L, creatinine: 503.8 µmol/L). Liver function test was unremarkable, serum albumin was 0.078 mmol/L and 24-h urinary protein excretion was 1 g. An immunochromatographic test for Plasmodium vivax was positive. Serological tests for dengue, leptospira, HIV, Hepatitis B and C virus and the Mantoux test were all negative.
An abdominal ultrasound scan showed a normal liver, a large spleen of 12.5 cm in length, bilateral hyperechoic kidneys, mild ascites and moderate bilateral pleural effusions.
Our patient was treated with injectable artesunate and received haemodialysis in view of her oliguria, but continued to have persistent proteinuria and deranged renal function tests.
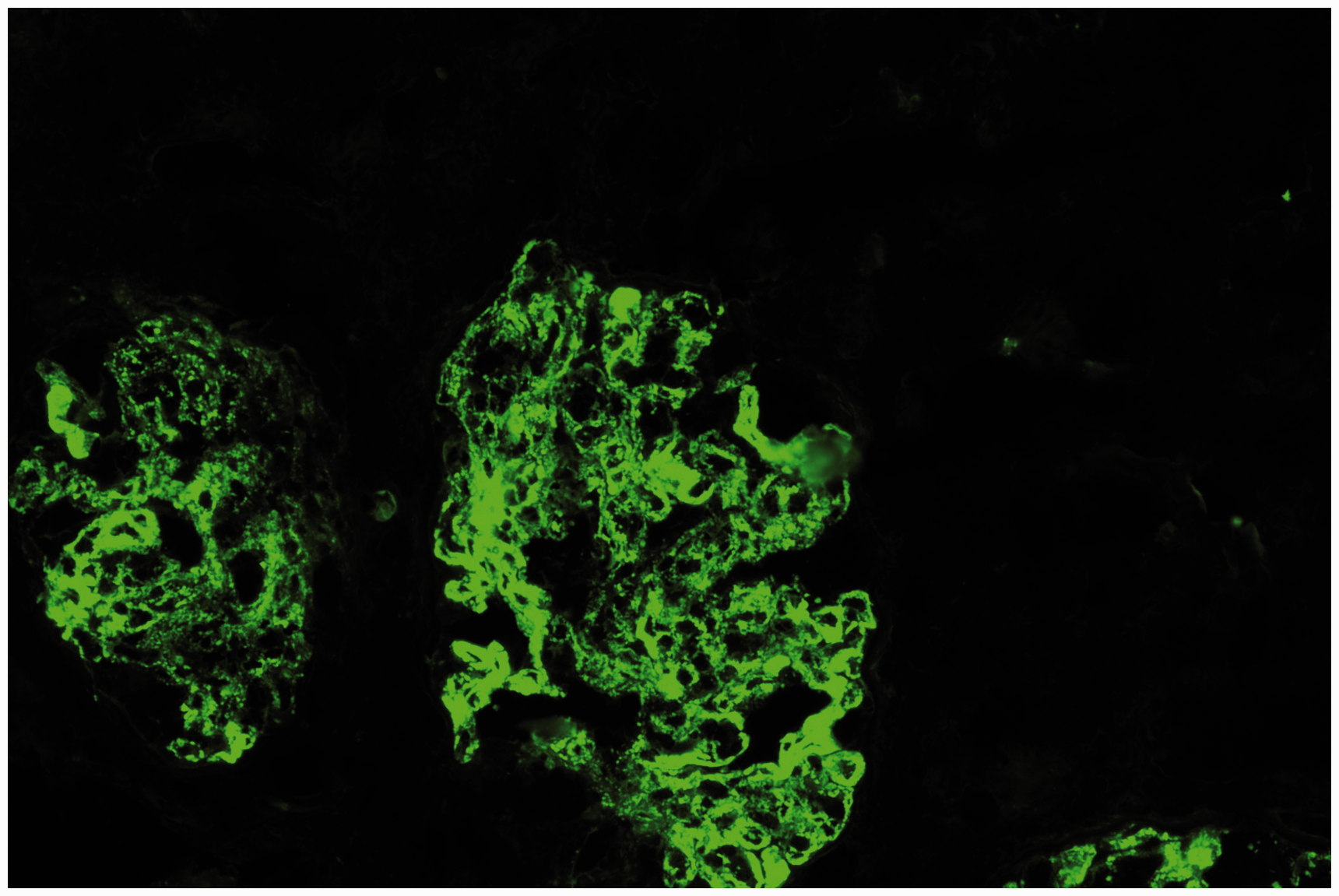
Further evaluation revealed strongly positive anti-nuclear (ANA) and anti-double-stranded (ds) DNA antibody tests. Complement C3 levels were decreased. Polymerase chain reaction (PCR) testing for Cytomegalovirus (CMV) and Epstein–Barr virus (EBV) was negative. A renal biopsy showed diffuse proliferative glomerulonephritis (class IV lupus nephritis) with ‘full house’ immunofluorescence (Figures 1 and 2). A diagnosis of SLE (class IV) nephritis with plasmodium vivax malaria was made. Our patient was treated with pulsed methylprednisolone and cyclophosphamide monthly for 6 months together with oral prednisolone. Her renal function, proteinuria and 24-h urinary protein excretion normalized after 3 months of starting therapy.
Showing diffuse proliferative changes on light microscopy. Showing diffuse proliferative lupus nephritis (staining for C3) on direct immunofluorescence (DIF).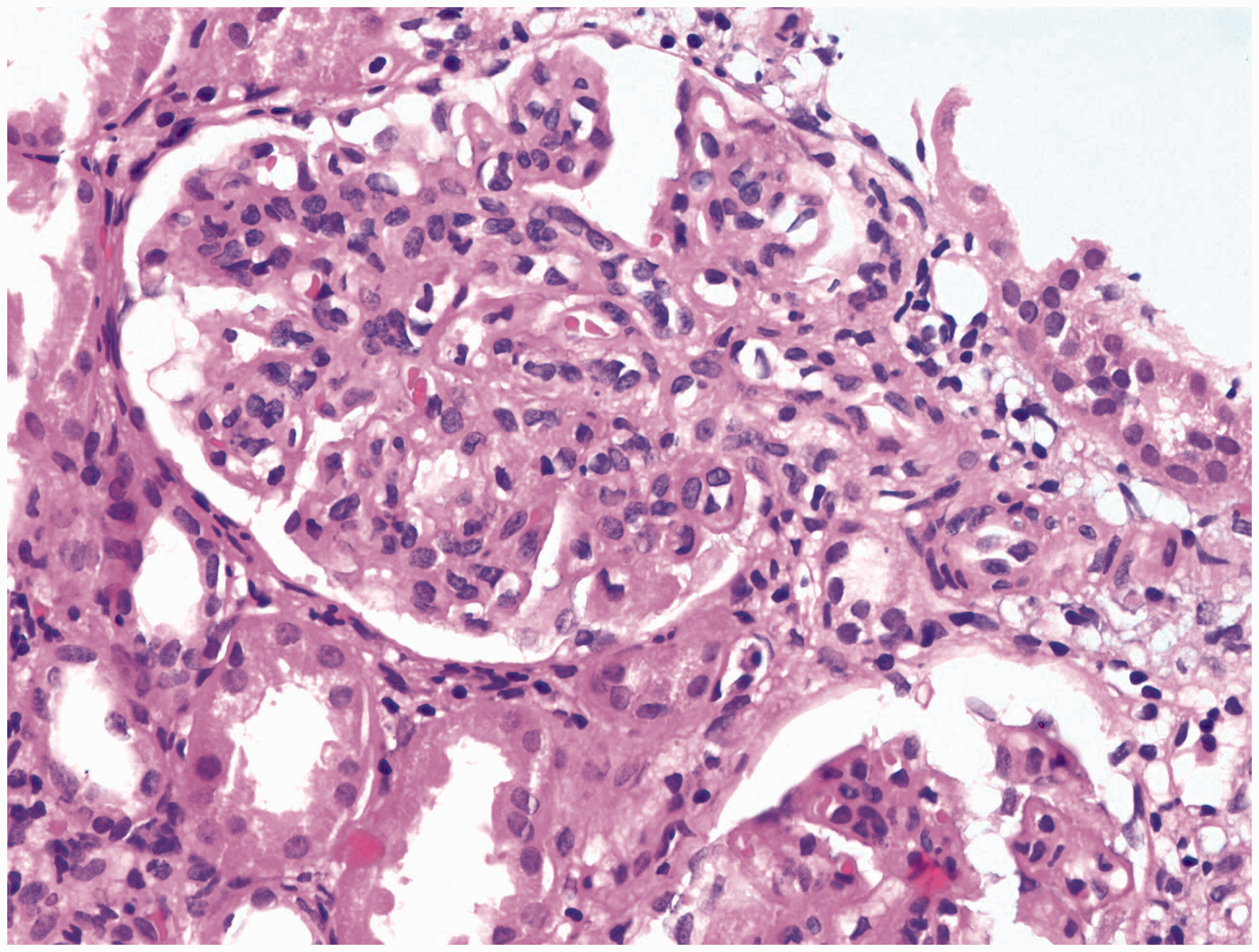
Discussion
For the development of an overt autoimmune disorder, a combination of immunologic, genetic and environmental factors, which might be of an infectious nature, is required.
Infectious agents have long been implicated in the pathogenesis of SLE, and viruses are the most important agents. While EBV and CMV are responsible for the majority of cases, others include parvovirus B19, retroviruses, paramyxomavirus and coronavirus.1–4 It is increasingly evident that some infections may be beneficial and their lack might actually facilitate SLE. Certain reports suggest that the malaria parasite, Toxoplasma gondii and Helicobacter pylori may have such protective effect.5–8
Malaria is a potent inducer of tumour necrosis factor (TNF), a cytokine involved in increased disease severity. As a result of reduced ability to generate TNF in areas where endemicity for malaria is low, there is a greater risk of developing autoimmune disease. 9 Malaria was found to be associated with the development of ANA and anti-ssDNA antibodies in Caucasians visiting tropical countries and in local inhabitants where malaria was endemic. However anti-dsDNA antibodies were not detected in any local inhabitants. Production of anti-DNA antibodies may be a response to circulating plasmodial DNA. 10
Even though well documented association of malaria with SLE lupus nephritis has been reported rarely, the occurrence of both entities could be coincidental. Our patient at presentation had plasmodium vivax infection with renal failure. Although acute tubular necrosis is the most common renal presentation of malaria, diffuse proliferative glomerulonephritis is known. However, the presence of a ‘full house’ pattern on immunofluorescence is very suggestive of lupus nephritis. Moreover, as an evaluation for other possible causes was inconclusive, our supposition is that malaria may have triggered or exacerbated underlying SLE already present in a subclinical form. Even though the mechanism by which malaria might trigger the onset or deterioration of SLE is not known at present, it is possible that tissue damage by malaria exposes auto-antigens for further triggering of an autoimmune response.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.