
Abstract
Scrub typhus, or tsutsugamushi fever, is a zoonosis of rural Asia and the western Pacific islands. The causative organism, Orientia (formerly Rickettsia) tsutsugamushi, is transmitted to humans by the bite of a larval Leptotrombidium mite (chigger). Scrub typhus may have gastrointestinal presentations, such as acute acalculous cholecystitis, duodenal ulcer perforation, peritonitis and gastric ulceration. Acute pancreatitis with scrub typhus has been reported rarely. We report a patient of scrub typhus complicated by acute pancreatitis and acute kidney injury.
Case report
Scrub typhus, or tsutsugamushi fever, is a zoonosis of rural Asia and the western Pacific islands. The causative organism, Orientia (formerly Rickettsia) tsutsugamushi, is transmitted to humans by the bite of a larval Leptotrombidium mite (chigger). Larval mites (of the Leptotrombidium deliense group) usually feed on small rodents, particularly wild rats of the subgenus Rattus. These zones are often made up of secondary or ‘scrub’ growth, hence the term scrub typhus. Scrub typhus can have manifestations of involvement of the lungs, kidneys and central nervous system. We report a patient with scrub typhus complicated with acute pancreatitis and acute kidney injury.
A 42-year-old farmer, a teetotaller, presented with abrupt onset of high grade fever with chill and rigor of 3 days’ duration. He also had 10 episodes of watery diarrhoea and vomiting for 2 days. He had a history of epigastric pain of 2 days’ duration. The patient also complained of back pain, breathlessness and oliguria which lasted 1 day. There was no history of haematemesis, malaena, haematuria or dysuria. On examination, an eschar on the right chest wall medial to mid axillary line was found. Jaundice, anaemia, subconjunctival haemorrhage and paedalodema were also present. He had bilateral crackles and hepatomegaly. Blood pressure was 90/60 mmHg and required two ionotropes. Computed tomography (CT) revealed diffuse enlargement of the pancreas with irregular contour and peripancreatic fat stranding (Figure 1). It also showed the size of the kidneys: right, 11.1 × 5.5 cm; left, 12.0 × 5.3 cm. There was no cholelithiasis. Other investigations were: serum creatinine, 548.2 µmol/L; blood urea, 50.7 mmol/L; serum sodium, 135 mmo/L; serum potassium, 5.6 mmo/L; serum bilirubin, 10.2 µmol/L; serum alanine aminotransferase, 110 IU/L; serum aspartate aminotransferase, 31 IU/L; serum alkaline phosphatase, 140 IU/L; haemoglobin, 143 g/L; total leucocyte count, 18.8 × 109/L; platelet count, 0.27 × 109/L; serum bicarbonate, 8.5 mmol/L; serum amylase, 900 IU/L; and serum lipase, 850 IU/L. Scrub typhus was diagnosed by qualitative immunoglobulin M (IgM) enzyme linked immunosorbent assay. The test was positive with the antibody present at dilution of >1:100. Polymerase chain reaction for 56-kDa antigen of O. tsutsugamushi confirmed the diagnosis of the scrub typhus.
CT scan abdomen axial section, plain, showing diffuse enlargement of pancreas with irregular contour and peripancreatic fat stranding suggested acute pancreatitis. The kidneys are large with a soft tissue density in left kidney.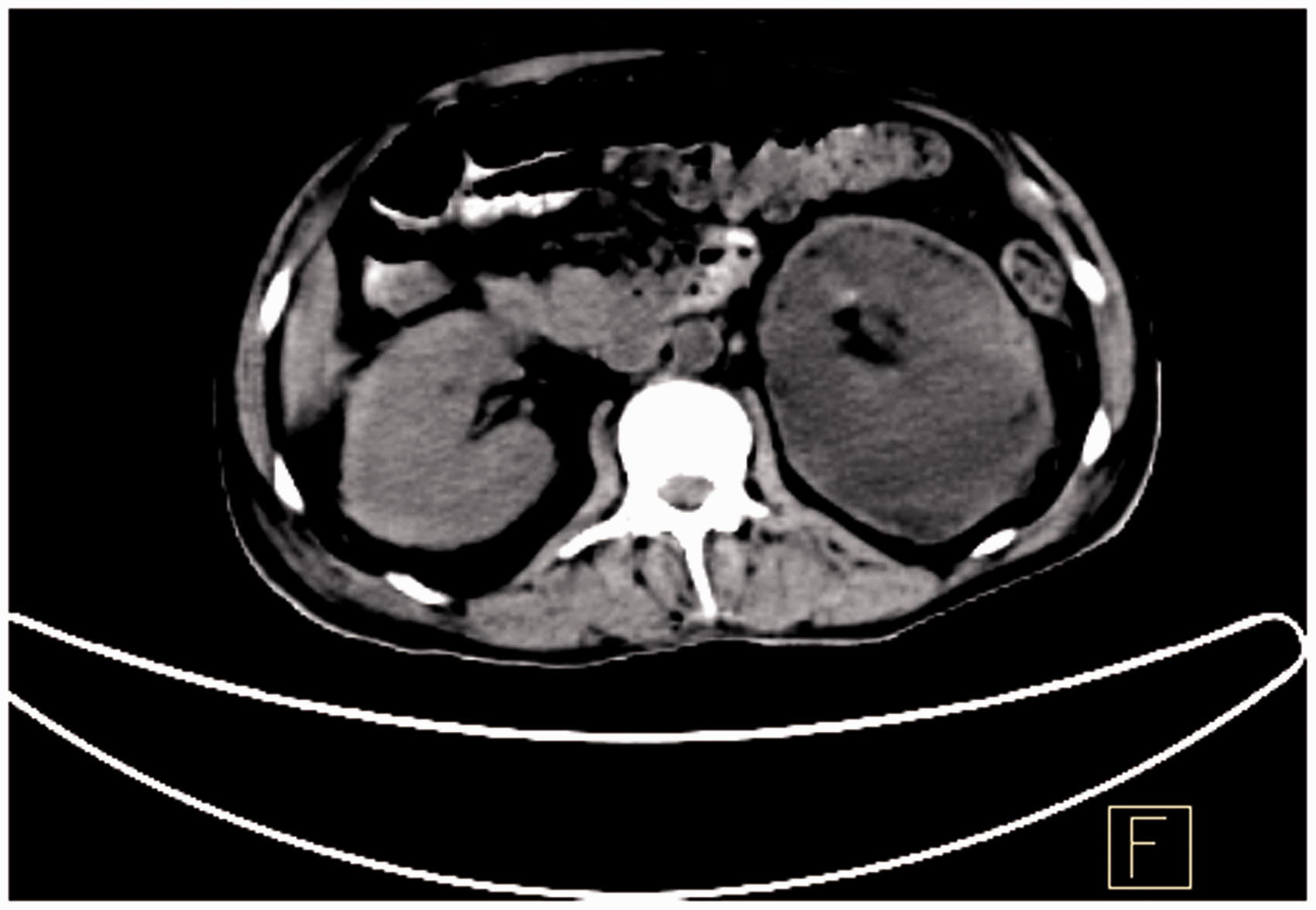
Investigations for malaria, leptospirosis, enteric fever and dengue were negative. Blood and urine cultures were negative. The treatment included continuous renal replacement therapy (CRRT), nil per os, parenteral tetracycline and proton pump inhibitors. The effluent dose of CRRT was 25mL/kg/hour to start with and later increased to 35mL/kg/hour The blood flow was in the range of 75–125 mL/min. Haemodialysis was started 56 h after CRRT. The investigations at discharge were serum creatinine (137.2 µmol/L [1.8 mg/dL]), serum amylase (200 IU/L) and serum lipase (150 IU/L) after 7 weeks of hospital stay.
Scrub typhus may have gastrointestinal presentations, such as acute acalculous cholecystitis, duodenal ulcer perforation, peritonitis and gastric ulceration. There were a few reports of acute pancreatitis with scrub typhus. The reports included it both as an isolated infection1–3 and as a part of mixed infection.4,5 In our patient, the diagnosis of both scrub typhus and the acute pancreatitis was unequivocal. Infectious causes of acute pancreatitis include mumps, coxsackie virus, cytomegalovirus, mycoplasma, legionella, salmonella and aspergillus. The pathogenesis of acute pancreatitis in scrub typhus is unknown. The proposed mechanism is vasculitis and perivasculitis of the small blood vessels due to widespread endothelial cell invasion by the causative organism. 2 Mortality in scrub typhus is in the range of 12–50%. 1 The reported mortality rate due to scrub typhus complicated with acute renal failure was 29.7% 1 and when associated with acute pancreatitis it was 42.8%. 2
Footnotes
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.