
Abstract

Background
Rickettsioses are prevalent throughout the world, and there have been increasing reports of outbreaks in humans from across India in recent years. 1 Rickettsiae are obligate intracellular gram-negative coccobacilli, usually transmitted to humans by infected arthropods such as ticks or mites. Rickettsiae are classified under five groups: (1) spotted fever group, including R. rickettsii, R. conorii and R. akari; (2) Typhus group, including R. prowazekii and R. typhi; (3) Scrub typhus (R. tsutsuga-mushi); (4) Q fever (Coxiellaburnetii); and (5) Neorickettsiosis. Rickettsial infections are characterised by the triad of high-grade fever, malaise, headache and skin rash. Their described manifestations include petechial lesions on the bulbar conjunctiva, Parinaud’s Oculoglandular syndrome, corneal ulcers, uveitis, retinal vasculitis, endophthalmitis and anterior ischemic optic neuropathy which could be sight-threatening.2–4 We report a similar case from south India, where a patient developed progressive decrease in vision owing to macular retinitis in both eyes, following a bout of fever with rash. The clinical features, serology and response to therapy were suggestive of Rickettsial aetiology. With the emergence of Rickettsial disease outbreaks including scrub typhus and the spotted fever group of diseases in India in recent years, ophthalmological screening will have an important role in supporting the diagnosis and preventing sight-threatening complications.
Case presentation
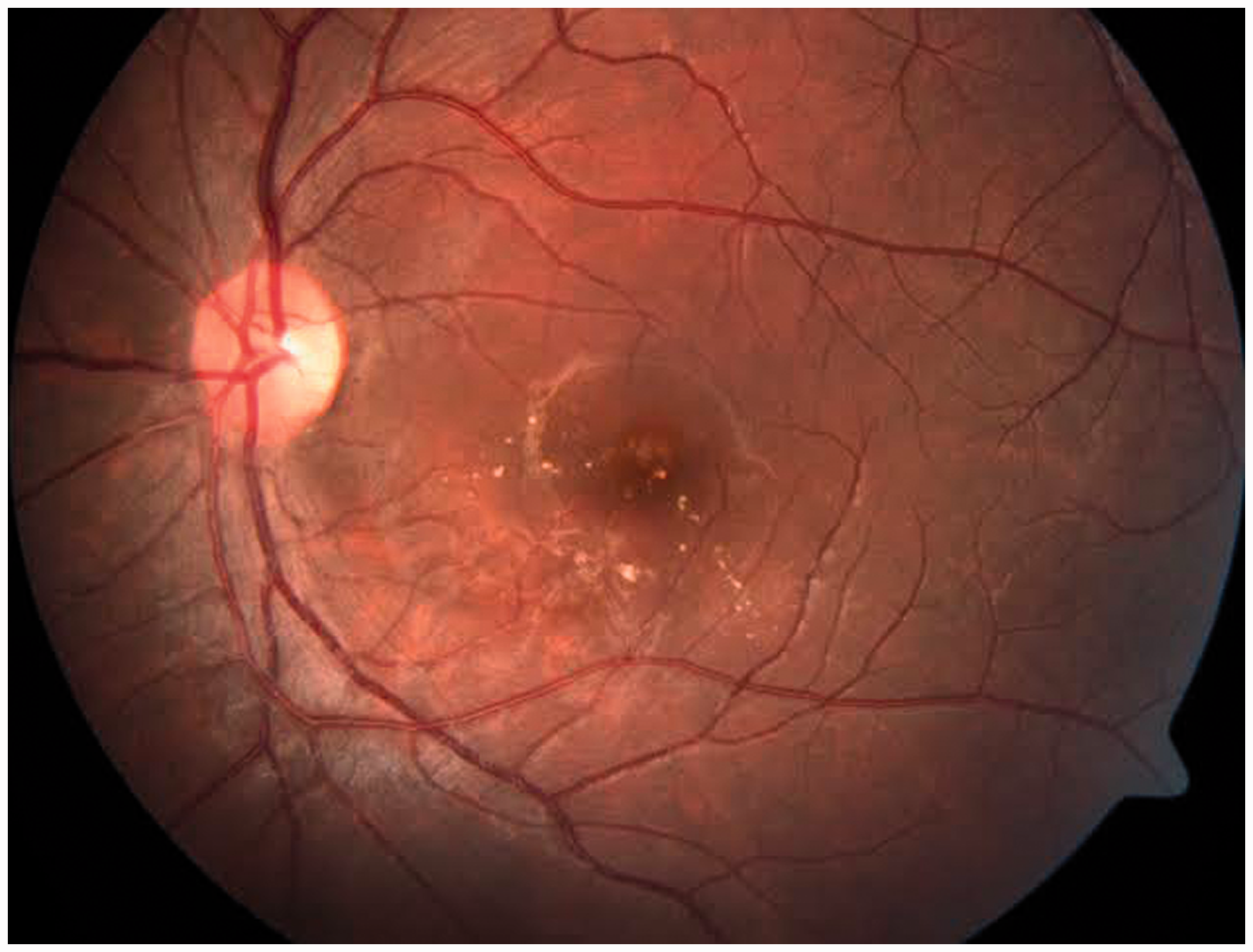
A 22-year-old woman presented with a history of painless progressive diminution of vision in both eyes over two weeks. She did not have any prior ocular morbidity. One month earlier, shortly after returning from a vacation to her relative’s home in a densely forested area, she had developed high-grade fever which preceded a generalised distribution of a macular spotted rash over the trunk and subsequently the limbs. It was associated with severe malaise, but there were no ocular symptoms. No investigations had been done earlier. Her previous prescription showed that she had been treated with antipyretics. No antibiotics were administered during the earlier episode of fever. On examination her best corrected vision was 20/120, N18 in the right eye (RE) and 20/50, N6 in the left eye (LE). Anterior segment and intraocular pressure in both eyes were normal. The vitreous had few cells with grade 1 haze in the RE, but the LE was unremarkable. There were multiple white patches adjacent to vascular arcade in both maculae, with adjacent oedema, macular star and disc hyperaemia (Figures 1 and 2).
Fundus photograph of right eye at presentation. Fundus photograph of left eye at presentation.

Investigations
Routine investigations for malaria, enteric fever and Chikungunya were negative. Treponema pallidum haemagglutination test (TPHA), serology for human immunodeficiency virus, antinuclear antibody (ANA), serum IgM and IgG to Toxoplasma gondii and Mantoux test were negative. Complete blood counts and chest X-ray were normal. IgM for scrub typhus was negative. Weil Felix test was positive and in favour of the spotted fever group (OX K: 1:80; OX19:1:320; OX 2:1:320). 5 Immunofluorescence and PCR could not be done due to financial constraints.
Treatment
Since the patient was not treated with antibiotics during the earlier episode of fever she was now treated with oral. Doxycycline 100 mg bid for 10 days along with oral Prednisolone 1 mg/kg/day with a weekly tapering dose.
Outcome and follow-up
On follow-up after six weeks, the patient’s visual acuity had improved to 20/30, N6 (RE) and 20/20, N6 (LE) with resolution of retinitis patches and macular oedema in an incomplete macular star pattern (Figures 3 and 4).
Fundus photograph of right eye post treatment after 6 weeks. Fundus photograph of left eye post treatment after 6weeks.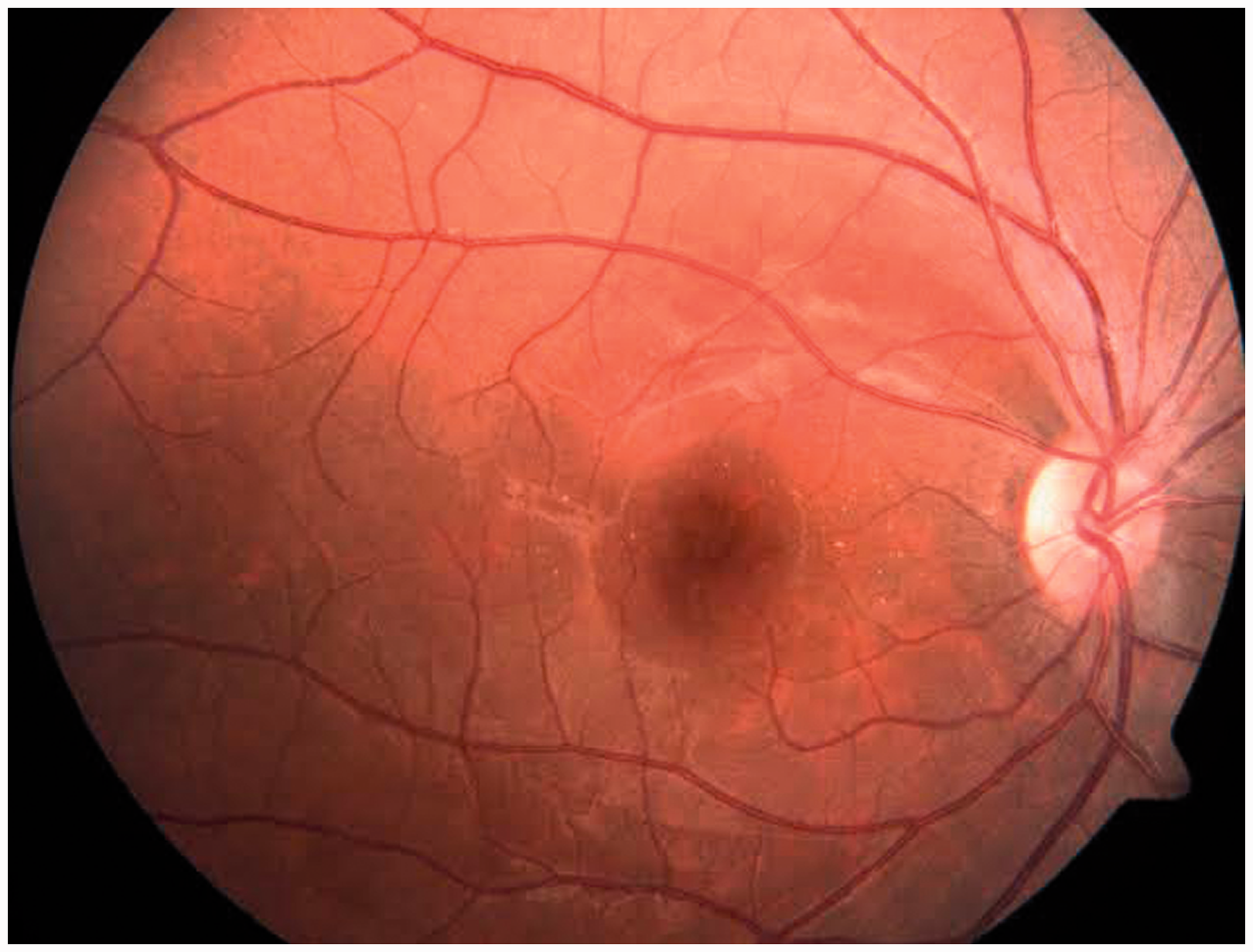
Discussion
Rickettsial infections have a worldwide distribution and outbreaks have been reported from the sub-Himalayan terrain of north India. Over the past decade, there has been an increase in such reports from the southern states. 6 The overlapping symptoms with other common exanthematous fevers and lack of access to specific serological markers for Rickettsioses also contributes to misdiagnosis as viral fever. Early detection can ensure complete treatment, with oral. Doxycycline (100 mg bid for 7–10 days) being the drug of choice.7,8
Although the exact pathology of Rickettsial ocular damage is not known, Rickettsiae are known to propagate within damaged endothelial cells. Vessels become blocked by thrombi producing vasculitis and the ocular manifestations. The time duration between the Rickettsial infection and ocular manifestation may vary and has not been definitively described thus far.
Conclusion
Neuroretinitis represents a self-limiting, benign, systemic inflammatory process with rarely a specific aetiology being identified. It is essential to consider Rickettsioses in the differential diagnosis of neuroretinitis especially if the patient is from an endemic area. Early diagnosis and treatment with doxycycline may help to prevent sight-threatening complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.