
Abstract
Dengue fever has classically been described as a disease of children and young adults. Infants are naturally protected by virtue of maternally derived immunoglobulins, especially in endemic countries. The resurgence of dengue, coupled with the availability of early and sensitive diagnostic methods and a high degree of clinical suspicion, has led to an increasing number of infants being diagnosed. There is a wide spectrum of clinical manifestations, particularly in infancy. Here we describe three cases presenting with diverse clinical features, their subsequent management and outcome.
Keywords
Introduction
Dengue fever is caused by four serotypes of Flavivirus (DENV 1–4) and is transmitted by the bite of an infected Aedes Aegypti mosquito. The disease is endemic in tropical countries and a large number of cases have been reported from the Indian subcontinent.1–3 According to the new World Health Organization (WHO) classification, the spectrum of presentation can range from mild viral illness (dengue without warning signs) to severe febrile illness (dengue with warning signs), and life-threatening severe dengue (with features of plasma leakage that may lead to shock or respiratory distress, severe bleeding, and/or severe organ impairment). Dengue affects all age groups including infants.1–5 Here we describe three cases of infants suffering from dengue with variable manifestations and their associated diagnostic challenges.
Case 1
A 30-day-old, exclusively breastfed, male neonate presented with fever and vomiting for 1 day. On examination, vital parameters, respiratory and cardiovascular examination were normal. There was no rash, moderate hepatosplenomegaly, and no signs of haemorrhage. Several mosquito bite marks were noted on the face. Investigations revealed a normal total leukocyte and differential count but there was a rising hematocrit (30% to 48%) and a worsening thrombocytopenia (87,000/mm3 on the first day falling to 34,000/mm3 by the third day). He was treated, as per protocol, for a presumptive diagnosis of clinical sepsis. C-reactive protein was negative and the blood culture was sterile. Investigations for malaria and a TORCH panel were negative. Maternal platelet counts were normal. The NS1 antigen tested positive. Thus, this patient had dengue with warning signs – hepatomegaly, haemoconcentration and rapidly declining platelet counts. The chest radiograph was normal and an abdominal ultrasound scan did not reveal ascites. The child recovered in 5 days with symptomatic treatment.
Case 2
An 8-month-old female infant, previously healthy, completely immunised who had no history of significant febrile illness since birth, presented with fever, cough and coryza and a single left-sided complex seizure. She had multiple petechiae all over her body, hepatomegaly and extreme generalized oedema, and features of decompensated shock. She was obtunded, with sluggishly reacting small-sized pupils and an extensor plantar response. Investigations revealed a haemoglobin of 122 g/L (haematocrit of 36.4%), total leukocyte count of 7800/mm3, platelet count of 87000/mm3 and compensated metabolic acidosis. The serum calcium and blood sugar levels were normal. Lumbar puncture revealed acellular cerebrospinal fluid with normal protein and sugar levels. Haematuria and clinical features suggestive of disseminated intravascular coagulation subsequently developed. The chest radiograph was normal. Seizures and shock were refractory to treatment, and the child died within 24 h of admission, despite intensive therapy. The blood culture was reported negative. Due to rapid worsening and haemodynamic instability an ultrasound could not be done. Later, dengue serology was reported positive. A diagnosis of severe dengue was thereby established.
Case 3
A 4-month-old, developmentally normal, clinically stable female infant presented with a single brief right-sided seizure. The serum calcium and blood sugar levels were normal. There was a history of hypoglycaemic seizure in the neonatal period but a magnetic resonance imaging, done at the age of 3 months, was normal. On the second day, diarrhoea and coryza ensued, with high pyrexia the following day. On the fifth day, the child’s abdomen distended on account of hepatosplenomegaly and ascites. Fever persisted without any evident localising signs. Investigations revealed thrombocytopenia (85,000/mm3). Tests for malaria, enteric fever and viral hepatitis were negative, though; IgM for dengue tested as positive. Liver transaminase levels were raised but, these declined to near normal levels by the 10th day. Abdominal ultrasonography on the sixth day revealed ascites and pleural effusion, which both resolved during the second week. There was no further fall in platelet counts, nor rise in haematocrit, nor bleeding manifestations. Antibiotics were initially prescribed on empirical grounds, but were discontinued after laboratory results (blood and urine culture sterile). The child recovered fully on symptomatic treatment and was discharged after 2 weeks. This child had dengue fever with warning signs.
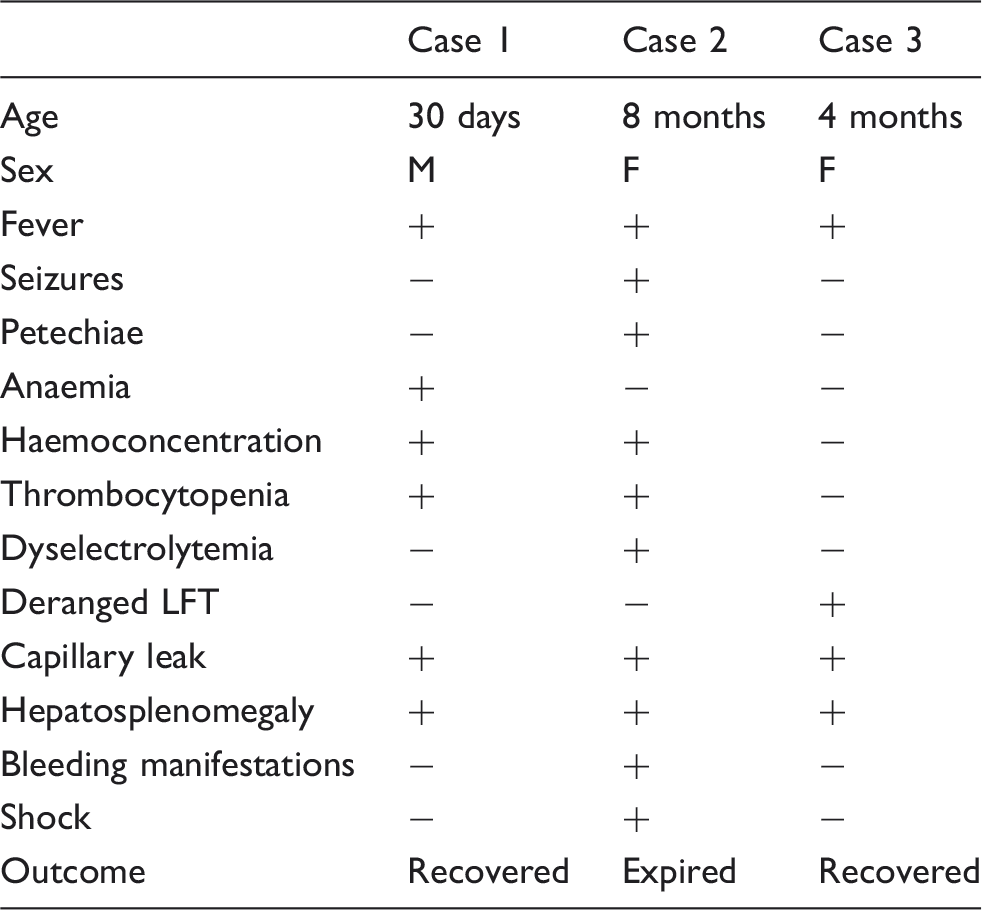
Comparison of clinical and biochemical profile of patients.
Discussion
Dengue virus affects all age groups with infectivity rates in the range of 50–90% in susceptible populations, especially during epidemics. Primary dengue infection results in lifelong immunity to the causative strain of virus and a short-term immunity (of months) against other strains. Severe dengue occurs in a majority of patients with secondary infection as well as in patients with primary infection. In the former, there is marked stimulation of the immune system owing to the presence of cross-reacting antibodies (antibody dependent enhancement [ADE]) and hence, increased cytokine production, which then results in capillary leakage. Primary dengue infection does occur in infants but clinical presentations are similar to secondary infection (probably because of maternally transferred antibodies). Infants with waning immunity and infection with a serotype, other than by types protected by maternally transferred antibodies, usually develop severe dengue.6–8 Infants also have an impaired physiological adaptability to compensate for capillary leakage; hence, there may be rapid clinical deterioration despite aggressive supportive management. It has been proposed that overproduction of both pro-inflammatory cytokines, such as interferon-γ and TNF-α, and anti-inflammatory cytokines, such as IL-10 and IL-6, are involved in the aetiopathogenesis of dengue haemorrhagic fever in infancy. 9 Transplacental transfer of maternal antibodies is of utmost importance in understanding the pathogenesis of this disease in infants and also in organising dengue vaccine trials. 10
The data on occurrence of dengue in infants from the Indian subcontinent are very scarce, varied and unorganised. In 2003, a dengue epidemic in India occurred and four neonates, including one as young as 4 days, were diagnosed positive. 1 In an epidemic in 1996 in Delhi, 9% of paediatric dengue cases occurred in infants (the youngest aged 3 months), while in 2006, a study from Ludhiana reported that infants constitute only 3.7% of all paediatric cases (the youngest aged 9months).3,4 However, infants constituted almost 20% of all paediatric cases during an epidemic in Chennai in 2001. 5 Dengue, and its vast spectrum of manifestations and severity in infancy, have been reported in various epidemics in previous decades. However, its diagnosis and reporting in this susceptible and unpredictable population, has been only rarely emphasised. General danger signs, such as fever, hypothermia, vomiting, refusal to feed, lethargy, irritability or oliguria, cannot distinguish between bacterial or viral sepsis. Thus dengue is another challenge in treating infants with non-specific features.
Severe dengue, with its high fatality rates, is however amenable to control strategies, but only if there is an organised approach to early diagnosis with institution of appropriate fluid therapy and monitoring. Dengue has low infectivity in infants, owing to transferred maternal antibodies. However, these antibodies may themselves result in an enhanced immune response and severe disease. Since, India is an endemic country; a large number of infants are likely to acquire this potentially fatal disease. With 2.5 billion people in over 100 countries at risk globally, epidemiological changes pose a significant problem with a high burden in Southeast Asian countries.8,11 Rapid urbanisation and large migratory populations, increasing population density, unchecked mosquito breeding and lack of sanitation all pose major threats to effective control. 12
The development of an effective vaccine against dengue has had major hurdles since the vaccine must be effective against all four serotypes. Secondary infection with a non-protected serotype in recipients of a single serotype vaccine would otherwise be disastrous. The WHO has approved a new dengue vaccine named Dengvaxia (CYD-TDV). This is a live, recombinant, tetravalent vaccine, used in a three-dose schedule of 0, 6 and 12 months. It has been registered for use in individuals aged 9–45 years and is being used in Mexico, El Salvado, Brazil and the Philippines. The WHO strategic advisory group in April 2016 recommended that countries should consider introduction of this vaccine in geographical settings of high endemicity. 8 There are other candidate vaccines under evaluation in clinical trials as well.13,14 Preventive measures to avoid mosquito breeding must also be emphasised to curb the burden of disease. Personal protective measures are effective but parental awareness regarding them is often lacking.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.