
Abstract
Chronic kidney disease (CKD) is a major cause of morbidity and mortality among individuals with HIV infection. Screening for proteinuria in HIV-infected children will help in early detection and treatment, and thus prevention and progression to CKD to end-stage kidney disease (ESRD). We screened 139 HIV-infected children aged 18 months to 18 years for proteinuria by urinary dipstick and confirmed by spot urine protein-to-creatinine ratio. If proteinuria was absent by the above methods, patients were screened for microalbuminuria by urinary albumin to creatinine ratio. We found proteinuria in 11.5% and microalbuminuria in 10.6% of our study population. The prevalence of proteinuria was higher in the advanced stages; 8.05% in stage 1, 12.12% in stage 2 and 26.32% in stages 3 + 4.
Introduction
HIV infection in children can lead to chronic glomerular disorders, such as HIV-associated nephropathy (HIVAN), HIV immune complex kidney disease (HIVICK), thrombotic microangiopathies, disorders of proximal tubular function and acute kidney injury. HIVAN is characterized by heavy proteinuria and nephrotic syndrome leading progressively to chronic kidney disease (CKD). 1 The commonest manifestation of HIVAN is persistent proteinuria. 2 Micro-albuminuria precedes proteinuria and has been shown to be an early manifestation of HIVAN. During the pre-antiretroviral therapy (ART) era, approximately 40% of all children infected with HIV in the United States presented with renal complications. 3 Strauss et al. reported the prevalence of childhood HIVAN to be 10–15% in the USA with over 95% being African American in origin. 4 Early detection of microalbuminuria may detect early onset of renal impairment thus facilitating prompt institution of antiretroviral therapy (ART) which will further help reduce mortality and morbidity associated with CKD in children. 5 There are few reports on the prevalence of proteinuria in children having HIV infection from India, hence our study was planned.
Patients and Methods
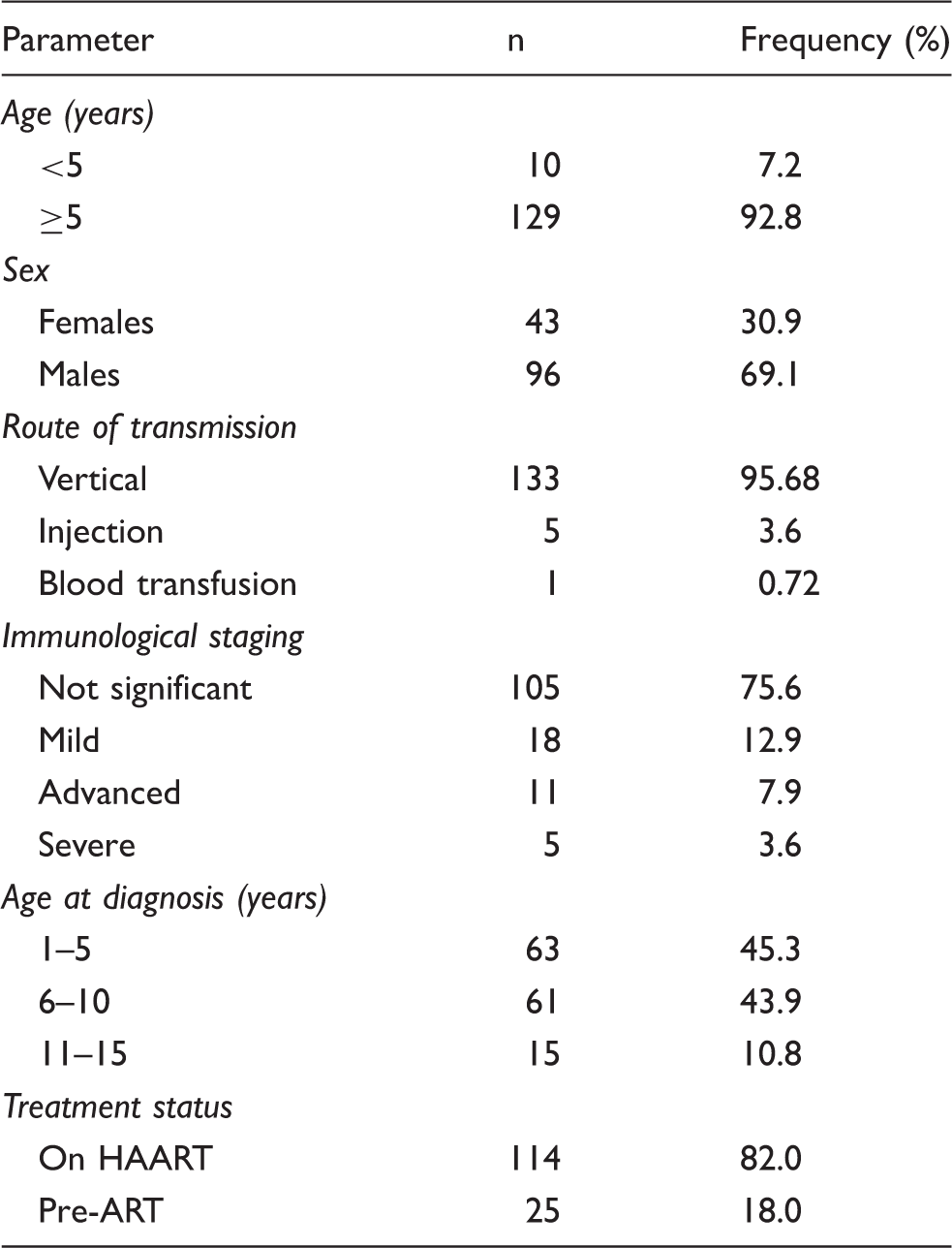
We screened 139 HIV-positive children consecutively aged between 18 months and 18 years who attended the ART clinic from November 2012 to March 2014. Those with any febrile illness, known case of CKD, autoimmune disease or taking steroids, angiotensin converting enzyme inhibitors or angiotensin receptor blockers were excluded from the study. Confounding factors for proteinuria such as exercise, cardiac failure, hyperglycaemia, hypertension and urinary tract infections were also excluded. A detailed clinical history, demographic data, World Health Organization (WHO) staging and treatment protocols were recorded. Investigations included complete blood count, liver and kidney function tests, blood glucose, serum electrolytes, serum cholesterol, complement levels (C3/C4), ANA, CD4 count, HbsAg and anti HCV. Early morning mid-stream urine samples were collected for determination of proteinuria by dipstick, and urine protein to creatinine ratio (Up:Uc). At a subsequent visit one month later, urine samples were collected and investigations repeated. Proteinuria was defined as a urine dipstick finding of 1+ or more on two or more occasions in the absence of fever and urine protein-to-creatinine ratio (each measured in mg/dl) of ≥0.2 with or without the presence of haematuria on urine microscopy. 2 Proteinuria was graded by dipstick as: >30 mg/dl (+), >100 mg/dl (++), >300 mg/dl (+++), and >2000 mg/dl (++++). Quantitative determination of human albumin in urine was done by immunoturbidimetric assay and according to the urine albumin/creatinine ratio (ACR) subjects were categorized 6 as normoalbuminuric (<30 mg/g), microalbuminuric (30–300 mg/g) or macroalbuminuric (>300 mg/g).
Results
Baseline characteristics of study population.
Characteristics compared in patients with and without proteinuria.
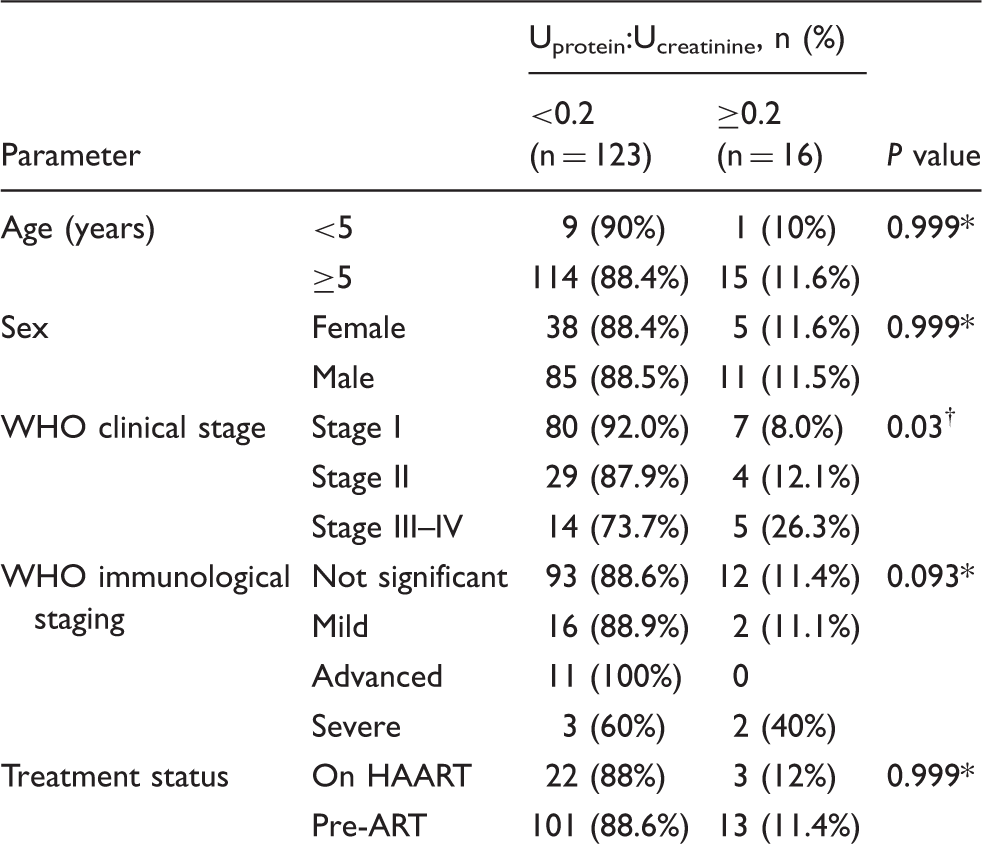
Fisher’s exact test.
Chi-square test.
Discussion
The prevalence of proteinuria was low when compared to previous studies. Studies from Africa have reported values in the range of 14.8–33%.7–9 Our lower prevalence may be due to different ethnicity and, moreover, the majority (86%) were at an early clinical and immunological stage of illness. As the disease advances, there is an increase in severe opportunistic infections which predisposes to sepsis and drug-induced kidney injury. A total of 82% of our patients were on antiretroviral therapy (ART). Three of the 25 ART-naïve patients had proteinuria. The mean duration of ART was almost similar in children with and without nephropathy (3.5 ± 2.4 years versus 3.4 ± 3.1 years). In children, initiation of ART with reduction of viral load and restitution of the immune system currently provides the most promising treatment to prevent the progression of childhood HIVAN to ESRD.9,10 Follow-up studies on children with HIVAN who were started on ART reveal reduction in proteinuria with decrease in viral load.2,9 Indinavir, atazanavir and tenofovir disoproxil fumarate (TDF) are antiretroviral agents commonly associated with direct nephrotoxicity. 11 Three of five patients with HIV-HBV co-infection who received combination of TDF + 3TC + EFV had proteinuria. No patient was receiving indinavir or atazanavir. Proteinuria due to Tenofovir may be due to proximal tubular damage leading to the renal Fanconi syndrome. 12 It is difficult to assess whether our patients had drug-induced proteinuria; however, Tenofovir is not prescribed for children aged less than 2 years, nor is it recommended as part of first-line treatment in children with Tanner stages 1–3, but the US FDA recently approved Tenofovir for use in children aged over 2 years. 13
Microalbuminuria in HIV-infected children has been determined in few studies in the past. In a recent study from the Congo, the prevalence was 18% in HIV-infected children and 2% in HIV uninfected children. 14 Microalbuminuria points towards early onset of renal impairment, thus prompt institution of ART in combination with ACE inhibitors or angiotensin receptor blockers (ARBs) to halt disease progression is recommended. 15 The HIV Medicine Association of the Infectious Diseases Society of America 16 recommend screening early markers of kidney damage, including proteinuria, from the time of HIV diagnosis in children and adolescents at least annually and more frequently with additional kidney disease risk factors. The rationale of screening of proteinuria in HIV-infected children is diagnosis of CKD and prevention of its gradual worsening. In India, comprehensive guidelines have been published by the National AIDS Control Organisation (NACO) for HIV care and treatment in children. 17 Limitations of the study include cross-sectional design, no control group and non-availability of viral loads in our patients.
In conclusion, we found proteinuria in 11.5% and microalbuminuria in 10.6% of our study population, even in early stages of disease. Our study may imply a significant burden of subclinical renal disease in HIV-infected children with normal renal function, irrespective of the clinical or immunological stage of HIV. Early screening should therefore be taken into account in defining a cost-effective strategy to prevent progression toward ESRD, particularly in resource-limited settings where substitute kidney treatments are generally unavailable.
Footnotes
Acknowledgements
This paper was presented at the XII Asian Congress of Pediatric Nephrology, 4–6 December 2014 in New Delhi, India. The authors thank Dr Shilpa Khanna Arora for her contribution in revising the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.