
Abstract
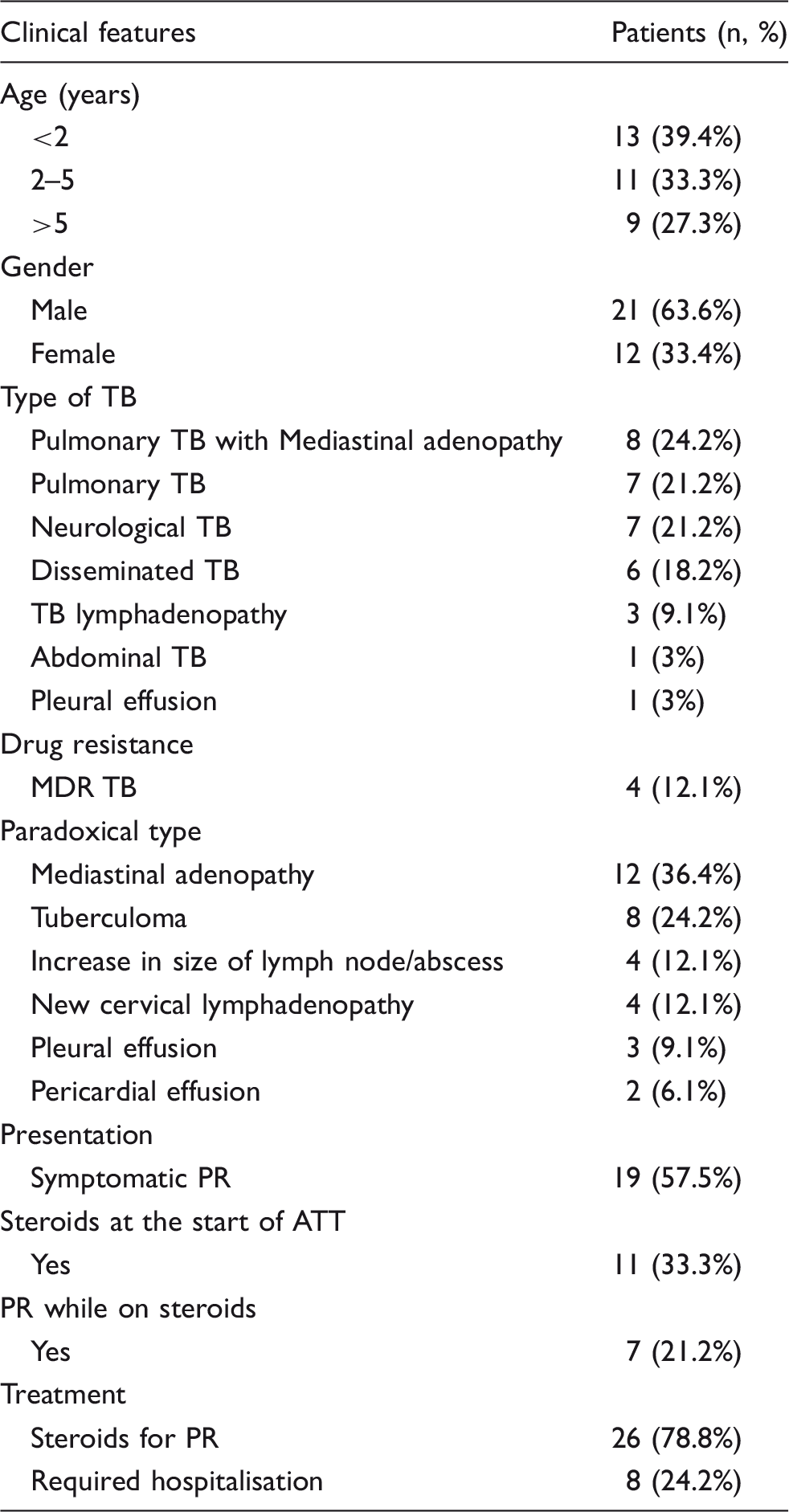
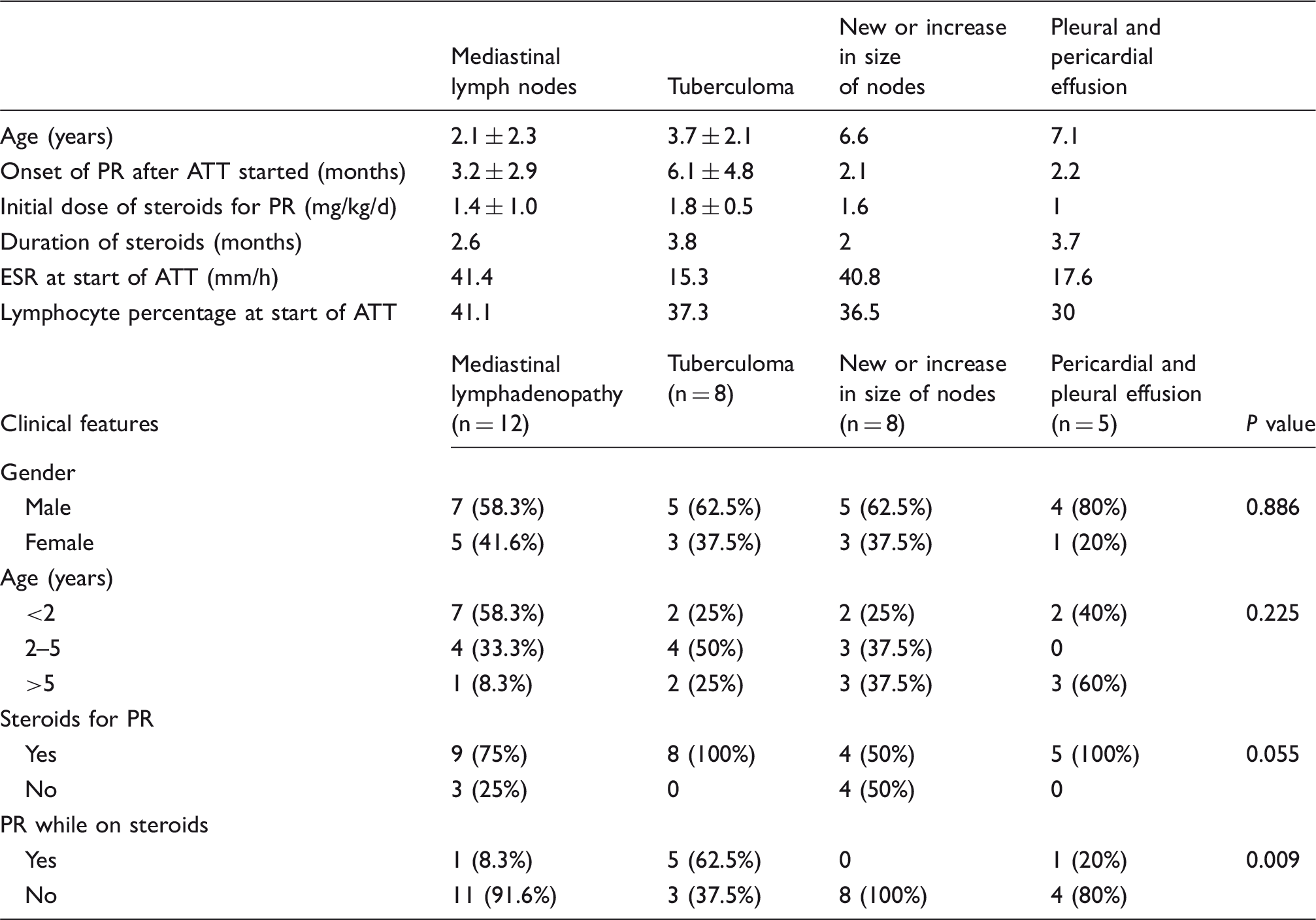
We sought to determine the incidence and clinical spectrum of the paradoxical reaction (PR) to treatment in 1000 children with tuberculosis (TB). Its incidence was 3.3%, presenting as mediastinal adenopathy (n = 12), central nervous system (CNS) tuberculoma (n = 8), increasing size of lymph nodes (n = 8) and serositis (n = 5). Symptoms included breathlessness (n = 7, 21.2%), neck swellings (n = 5, 15.2%), hemiplegia (n = 3, 9.1%), raised intracranial tension (n = 2, 6.1%) and fever or diabetes insipidus (n = 1, 3% each). The mean age of onset of PR was 3.5 months after the start of anti-TB medication. PR was seen predominantly in boys. Mediastinal lymphadenopathy was more common in children aged <2 years. Tuberculomas were more common in children aged 2–5 years. Nodal enlargement and serositis were seen equally in all age groups.
Introduction
During the treatment of tuberculosis (TB), paradoxical reaction (PR) can occur. It is defined as the clinical or radiological worsening of the pre-existing tuberculous lesion or the development of a new lesion in a patient who initially improves with anti-tuberculosis therapy (ATT), 1 in the absence of disease relapse. It occurs in about 11–15% of patients with TB. 2 It is unpredictable in its timing (occurring anything from a few days to many months [range, 14–270 days] after the start of anti-tuberculosis chemotherapy) and in its duration and severity. 1 PR can occur in both HIV-uninfected and HIV-infected patients. It may manifest as recrudescence of fever, enlarging adenopathy, worsening pulmonary infiltration, pleural effusion, ascites, new or enlarging parenchymal CNS lesions, superior vena cava syndrome and involvement of bone, skin and soft tissue.3–6 While these reactions are self-limiting, respiratory failure and death have been described, mainly with miliary and pulmonary disease. 7 This study was undertaken to determine the incidence and clinical profile of children with PR.
Material and Methods
Our retrospective observational study was conducted after approval from the institution ethical committee. All children aged up to 15 years with TB and with PR who presented to the TB clinic during 2007–2012 were included. Records of all patients were evaluated; clinical history, examination findings and laboratory investigations were noted. Patients with drug-resistant TB on treatment with second-line therapy who had development of new lesions not related to treatment failure and were responding to the second-line therapy were also included. Patients who worsened owing to treatment failure, to non-compliance or to drug resistance, and HIV-infected patients and patients with congenital immunodeficiencies were excluded from the study.
PR was determined if there was clinical or radiological worsening of pre-existing the tuberculous lesion or the development of a new lesion in a patient who had initially improved with ATT and/or had become culture/smear-negative for TB or, in patients in whom cultures could not be done, when improvement was noted on continuing ATT. Worsening of radiological findings was defined when pleural or pericardial effusion appeared or increased, new parenchymal lesions developed with or without mediastinal lymphadenopathy, neuroimaging showed new lesions or increase in tuberculomata, or there was an increase in the size of existing lymph nodes.
Age, sex, onset of PR after treatment, duration of PR, types of PR and requirement of steroids for treatment of PR were noted and details of clinical history, examination, investigations and treatment were recorded. All patients underwent chest radiography and had Mantoux test, full blood count and erythrocyte sedimentation rates (ESR) done. Further investigations, such as culture/smear, were carried out as and when required. Cerebrospinal (CSF) PCR was done in patients who could afford it. Specific investigations such as biopsy, fine needle aspiration cytology, neuroimaging or chest imaging and ultrasound examination were done as required. Investigations were repeated whenever necessary. Patients were treated with standard ATT protocol as per RNTCP 2010 guidelines. No patients were under a directly observed treatment schedule (DOTS) and all were taking medicines as prescribed at home.
Descriptive data were analysed in proportion and percentage. Types of paradoxical reaction with various clinical parameters were analysed with χ2 and Fisher’s exact test. P value < 0.05 was considered significant. Numerical data were analysed by statistical significance between the mean calculated by Student’s t-test. The risk of getting various types of paradoxical reactions with various factors such as age and gender was determined by odds ratio (OR). All data were statistically analysed using SPSS software version 18 and Primer.
Results
Demographic pattern of patients and type of paradoxical reactions.
Clinical factors associated with various types of paradoxical reactions (PR).
Discussion
In 1000 TB patients, paradoxical reactions were only seen in 33 and thus the sample size in our study was small. In adults, the incidence of PR has been reported as from 2.4% in pulmonary TB 8 to 23% in lymph node TB, 9 23% in pleural TB 10 and 17.2% in CNS tuberculosis. 11 PR has been reported in up to 35% of immunocompromised patients with HIV infection and in 2–10% in immunocompetent patients.12,13 None of our patients had HIV and thus we cannot comment on the incidence of paradoxical reaction in HIV-positive patients as reported elsewhere.8,14
It has been suggested that a higher bacillary load also predisposes patients to develop a PR. 15 That the reaction can occur even after prolonged therapy suggests that the antigenic stimulus may be poorly cleared from disease sites. M. tuberculosis has a number of insoluble lipid-rich antigens in its cell wall that potentially invokes an inflammatory response, a mixed type 1 T helper cell (Th1) and type 2 T-helper cell (Th2) response 15 and the activation of mononuclear phagocytes, and it may be that these components are responsible for the phenomenon of a deterioration in TB status. 16 Thus, it would be expected that PR would be more frequent in adults owing to the multibacillary nature of the disease in adults and less frequent in children due to the paucibacillary nature of disease in children. However, in our study, paradoxical reaction was seen mostly in children aged <5 years. Apart from bacterial load, other body responses may also have a role in causing PRs which may lead to more young people being affected.17,18
Lymph node enlargement either as mediastinal adenopathy or an increasing size of cervical nodes was a most common feature. More than half were symptomatic and approximately 25% had tachypnoea. Thus, children with pulmonary TB should be carefully monitored for respiratory distress and it should be noted that such clinical deterioration may suggest PR.
CNS tuberculoma was seen in more than one-quarter. Why the tuberculoma occurs on treatment is not properly understood. One possibility is that this occurs because of decreased penetration of anti-tubercular drugs into the brain. Restoration of the blood–brain barrier (BBB) with appropriate treatment is thought to result in reactivation of latent foci. 11 However, this hypothesis cannot explain the development or enlargement of intracranial tuberculomas which are treated with isoniazid and pyrazinamide, both of which freely cross the BBB in the absence of inflamed meninges. The reason for the occurrence of this response in only some cases and not all suggests that it depends on host immune responses, virulence of tubercle bacilli, antigen load and effective ATT. The improvement seen with steroid therapy for PR in neuro-tuberculosis may be due to a reduction in cerebral oedema and/or to a direct anti-inflammatory mechanism on the cerebral vasculature. 19
PR were seen in approximately 20% with disseminated TB. This suggests that overall mycobacterial load can influence the development of PR. Campbell and Dyson 20 proposed that rapid killing of bacilli by effective ATT may release large amounts of tuberculoprotein and other cell wall products, generating a hypersensitivity reaction.
Five patients presented with serositis, of whom two had pericardial and three had pleural effusions. Pericardial effusion is a rare manifestation of PR. For pleural effusion, it is speculated that this results from the rupture of a subpleural pulmonary tubercular focus into the pleural space, which allows for tuberculoproteins to enter the pleural space and generate the hypersensitivity reaction responsible for a pleural effusion. 21
The usefulness of corticosteroids in the treatment of PR is not well established and controversial. 22 Corticosteroids are usually used for a severe systemic manifestation or a prolonged duration of PR. In our study, more than 75% of the patients with PR received steroids. Jung et al. 10 found that patients treated with steroids had a shorter duration in improvement of pleural effusion compared with patients who did not. In our study, all patients with tuberculoma, pleural and pericardial effusions were treated with steroids. In fact, five (62.5%) with miliary TB and PR were already taking steroids and so required a higher dose. The use of steroids at the start of ATT needs to be assessed. Adjuvant therapy with corticosteroids, in conjunction with ATT, may be appropriate in particular forms of TB. Prospective controlled trials have shown a benefit in tuberculous meningitis, pericarditis and pleurisy. Although benefit has been shown in pleural disease, adjuvant therapy is not routinely required unless there are significant systemic symptoms of fever or a particularly large effusion. Though doses of 2 mg/kg/day of prednisolone have been routinely used, high doses of even 4 mg/kg/day have been tried in patients with CNS TB.23,24
In conclusion, the occurrence of PR during ATT needs vigilance. Prompt recognition is essential to differentiate it from treatment failure or drug resistance. PR does not need change in ATT though sometimes the addition or dosage adjustment of steroids is needed to control symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.