
Abstract
Background
Ectopic pregnancy contributes to maternal morbidity and mortality, especially in low-resourced countries with limited facilities for early diagnosis and treatment. It is a very challenging condition to diagnose. Patients may collapse and die while undergoing investigation.
Aims
To assess surgical treatment given to patients presenting at Mpilo Central Hospital, the challenges that are faced and the outcomes; and also to document how women survive this dangerous condition in a setting challenged by low resources.
Results
All the patients had prompt life-saving surgery within 48 h of admission despite the challenges faced. The survival rate was 100% during the period of the study.
Conclusion
It is possible to prevent maternal mortality in low-resource countries by maintaining basic clinical and surgical skills.
Introduction
Ectopic pregnancy is a pregnancy that exists extra-uterine. It is the most dangerous, life-threatening, gynaecological emergency. It contributes to maternal morbidity and mortality. Ectopic pregnancy affects 1–2% of all pregnancies and is responsible for 9% of pregnancy-related deaths in the USA. 1 Some ectopic pregnancies resolve spontaneously but others continue and can lead to rupture of the Fallopian tube. 2 The risk factor is Chlamydia trachomatis infection 3 that causes chronic tubal damage leading to abnormal blastocyst implantation in the Fallopian tubes instead of the corpus of the uterus. Symptoms range from none to shock 4 and catastrophic demise from hypovolaemic shock. In low-resource settings, the presentation, diagnosis and management of ectopic pregnancy can be challenging.
Methodology
This was a retrospective descriptive cohort study in a tertiary referral centre. The records from the gynaecology ward/theatre/casualty/mortuary registers were used to identify all the patients that were admitted/seen to/at the hospital with a diagnosis of ectopic pregnancy from 1 January 2016 to 30 November 2016. This information allowed patients’ case-notes to be retrieved from the hospital records department. There were 65 patients with a diagnosis of ectopic pregnancy admitted during this period of the study and their case-notes were pulled out. Information on the demographic, investigative, treatment and outcome parameters were then collected using a data collection sheet. The SPSS Version 21 statistical tool was used to calculate the mean and standard deviation (SD) figures. There were three patients with a missed diagnosis that were later brought in dead and these patient details were not analysed in the study.
Results
Patient characteristics.
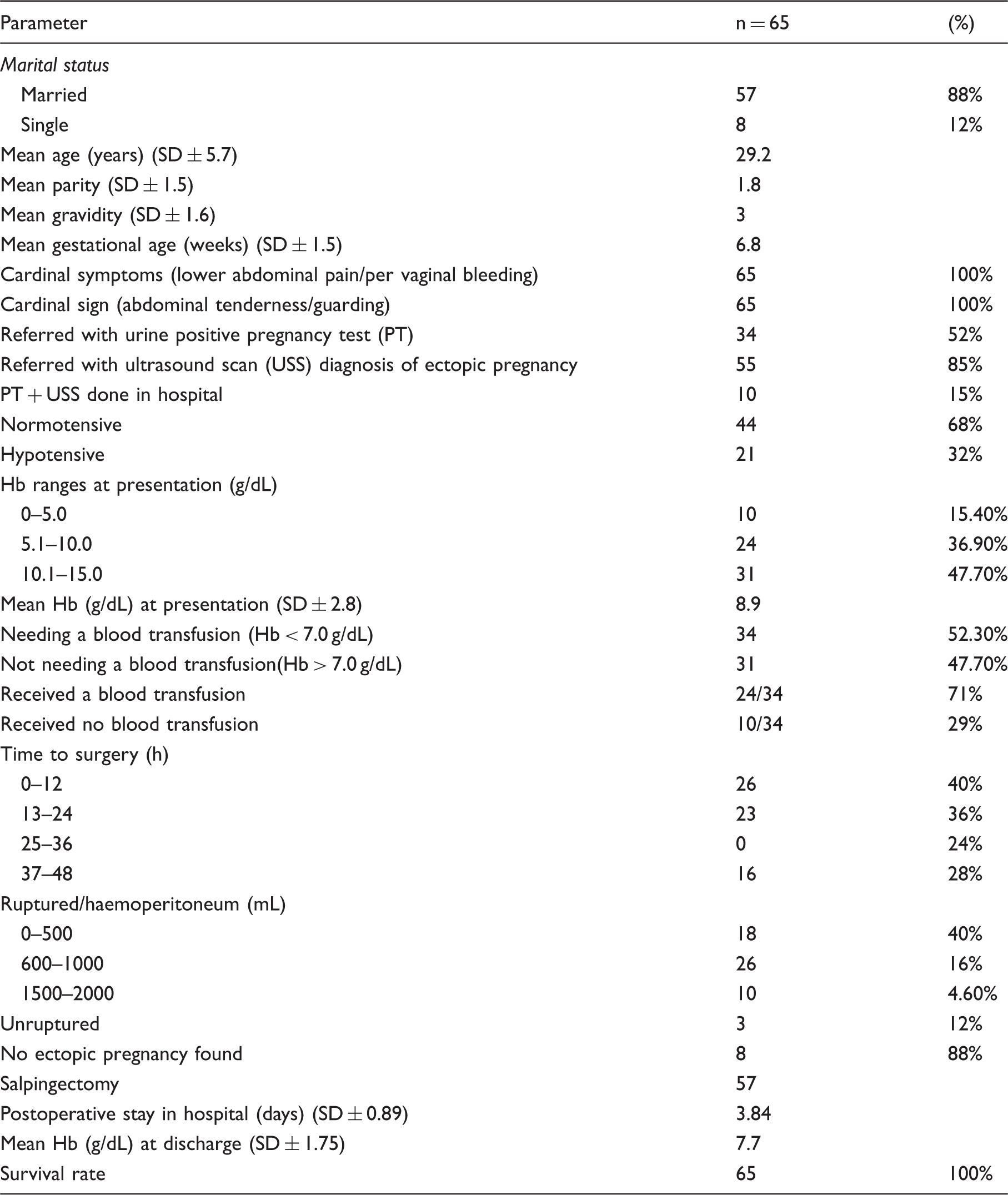
A urine pregnancy test was done in 52% of cases and 85% of the patients had already had an abdominal ultrasound scan at the time of admission. These patients had consulted private doctors and had been scanned by private ultrasonographers. The rest were admitted via the Casualty Department and during the study period. Three were missed and the diagnosis was confirmed at postmortem examination when the patients were brought in dead. Only 15% of the patients had both a pregnancy test and ultrasound scan done in the hospital; 32% of patients presented with hypotension.
Of the patients, 47.7% presented with a haemoglobin (Hb) level of > 10.1 g/dL, 36.9% with a Hb level of 5.1–10.0 g/dL and 15.4% of the patients had a Hb level of < 5.0 g/dL. Those with a Hb level of < 7.0 g/dL (52.3%) were prescribed a blood transfusion, 24/34 (71%) patients received a blood transfusion intra-/postoperatively. Ten patients (29%) did not receive a blood transfusion despite the prescription. This was due to the unavailability of blood transfusion products due to stock shortages at the blood transfusion unit.
Most patients (76%) underwent surgery within 24 h of admission. Of these patients, 24% had delayed surgery that was done 37–48 h after admission. This delay was due to either a misdiagnosis of threatened miscarriage and/or the patient underwent investigations such as ultrasound scans before a decision was finally made to take them to theatre for laparotomy.
At surgery, 84% had a ruptured ectopic tubal gestation, 16% had a haemoperitoneum of 1500–2000 mL; 4.6% of the ectopic pregnancies were unruptured. Salpingectomy was done in 88% of cases. There was no ectopic gestation found at laparotomy in 12% of the patients, their diagnosis being normal pelvic organs or ovarian torsion. All these patients with negative findings for ectopic gestation had delayed surgical intervention and all had positive pregnancy tests and inconclusive scan reports. It is possible that they may have had a miscarriage or an early intra-uterine pregnancy that was missed on ultrasonography or it was too early to be detected.
The mean hospital stay postoperatively was 3.84 days (SD ± 0.89). The mean discharge Hb level was 7.7 g/dL (SD ± 1.76). The survival rate was 100% during the period of the study.
Discussion
Ectopic pregnancy can have catastrophic consequences. It poses great diagnostic challenges; this is more so in low-resource countries where they contribute significantly to maternal mortality. At the same time, the safety of the patient is important. 5 Any patient of reproductive age with lower abdominal pain and/or per vaginal bleeding should have a differential diagnosis of ectopic pregnancy and must be investigated for this diagnosis. All casualty departments must take extra caution when dealing with women of reproductive age complaining of vague pelvic/abdominal pains before they are sent away. A digital vaginal examination may cause rupture and cause patient demise; hence, care must be taken where there is no immediate access to theatre.
Therefore, these results presented here are encouraging as they show that even in low-resource settings maternal mortality can be tackled by using basic clinical and investigative tools to institute prompt life-saving surgery. It was not possible to do the pregnancy test on everyone, either due the unavailability of the test or the diagnosis was very clear or the patient was in a state of collapse. Basic ultrasonography is the most diagnostic tool 6 used to aid in the diagnosis. In this study, 84% of the patients had already undergone this test at the time of admission and the diagnosis was clear. The other 16% underwent the test in hospital before surgery was performed. In these low-resource settings, patients’ delay in seeking treatment and doing serial ßhCG levels would cause further delays and can lead to catastrophic results. These tests and diagnostic laparoscopy 7 are not readily available.
Blood transfusion products are not readily available, hence ten patients out of the 34 that needed a blood transfusion did not get a blood transfusion. In our unit, a blood transfusion is thought to be indicated when the patient is in hypovolaemic shock or the Hb is < 7.0 g/dL and they are going for surgery. The risk of HIV infection is low as the local blood bank uses international standards for blood donation and screening. There are no sophisticated facilities for autotranfusion like a Cell Saver® in low-resource settings, but in a shocked patient with a ruptured ectopic pregnancy this may not be appropriate, and a simple manual method using a sterile ladle, sieve, contents of a blood collection bag to prevent any further clotting and a filtered giving set works well if there is no donor blood available.
The treatment of ectopic pregnancy is usually salpingostomy or salpingectomy. 8 Of the patients, 56% already had a significant haemoperitoneum (600–2000 mL) and underwent salpingectomy. Salpingostomy was not carried out as the cases were operated upon by middle-grade doctors who were not familiar with this technique.
Other treatment modalities, such as expectant management or methotrexate injections, 9 are either inappropriate or resources do not allow them to be carried out. Success rates after methotraxate treatment are in the range of 75–90% 10 and are claimed to be as effective as surgical treatment. 9 If there is diagnostic doubt, prompt laparotomy should be carried out to save lives, especially in settings were resources are scarce. In rural areas where there are no diagnostic laparoscopic facilities, mini-laparotomy may be done and surgery performed by those skilled in this procedure. It is better to have a negative ectopic pregnancy rate of 12% than receive postmortem reports of ruptured ectopic gestations. Those patients that already show signs and symptoms of intra-abdominal bleeding, surgery should not be delayed surgery while awaiting investigations such as ultrasound scans. Prompt surgery must be carried out. This is the teaching at this unit; hence, the survival rate of diagnosed patients was 100%, or 96.6% if the three cases where the diagnosis was missed are included.
The crude intra-uterine rate 24 months following salpingectomy is 55.5% with a recurrent rate of 8.1% for salpingectomy and 6.3% for salpingostomy. 11 This should be discussed with the patient; those who have completed their families should be offered bilateral salpingectomy and prevent recurrence that may be fatal in the future for the patient.
Conclusion
This study has shown that it is possible in low-resource settings to care for women and prevent maternal morbidity and mortality by using simple methods and little available resources and offering prompt life-saving surgery. The 12% negative ectopic pregnancy rate is justifiable in that, faced with a potentially devastating life-threatening condition and little resources, the only option left is life-saving surgery that can produce a 100% survival rate. Attention should focus on capturing all those women that have a diagnosis missed at the Casualty Department and die later at home.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.