
Abstract
Chronic cor pulmonale is defined as right ventricular failure secondary to pulmonary hypertension. Our study reviewed all cases of chronic cor pulmonale secondary to respiratory diseases in a ten-year period (2004–20014) in the Department of Child Health, Korle-Bu Teaching Hospital, Ghana. Nine cases of chronic cor pulmonale were recorded during the period. The age range was 1–9 years (average age = 3 years). Obstructive sleep apnoea secondary to adenoid hypertrophy was the commonest cause of pulmonary hypertension.
Introduction
Pulmonary hypertension 1 leads to a combination of hypertrophy and dilatation of the right ventricle. According to the Guidelines from American Heart association and Thoracic Society, pulmonary hypertension is defined as resting mean pulmonary arterial pressure > 25 mmHg beyond the age of three months at sea level. Pulmonary hypertension is caused by pulmonary vascular diseases related to cardiac, lung and systemic diseases. In addition, idiopathic vasculopathy occurs which is a diagnosis of exclusion. 2 This is in contrast with acute cor pulmonale, which is defined as acute right heart strain or overload resulting from pulmonary hypertension usually following pulmonary embolism.
Factors contributing to development of pulmonary hypertension include: (1) hypoxia, which is the most potent stimulus for the development of pulmonary constriction;1,3 (2) increase in blood viscosity; 3 and (3) increase in pulmonary blood flow. Pulmonary vasoconstriction produces an acute rise in pulmonary artery pressure. Continuing vasoconstriction with pulmonary hypertension of even a few days’ duration is associated with structural changes in pulmonary vessels, brought about by an increase in the thickness of the medial coat, endothelial swelling, hypertrophy and the appearance of muscle at more peripheral levels than normal. 4 This continued insult leads to a reduction in cross-sectional area of the vascular bed with ventilation-perfusion mismatch.
While the main pulmonary artery and aorta are elastic structures, arteries accompanying conducting airways such as lobar bronchi, respiratory bronchi and alveolar ducts are muscular or partially muscular and, thus, are subject to constriction from hypoxia. The severity of pulmonary hypertension in association with chronic respiratory disease correlates more closely with survival than any other variable studied. 5
A diagnosis of heart failure due to right ventricular hypertrophy requires a high index of suspicion since symptoms of heart failure such as easy fatiguability and tachypnoea are obscured by the primary pulmonary disease itself. The American Heart Association recommends early echocardiographic studies to diagnose pulmonary hypertension in children with obstructive apnoea and sickle cell anaemia. 2 Systolic pulmonary artery pressure can be estimated by echocardiographic Doppler assessment using definition of mean pulmonary artery pressure of >25 mmHg. 2
Our study was propelled by the fact that early diagnosis can lead to treatment of the respiratory disease which would then improve a child’s cardiac status.
Methods
Ours was a retrospective descriptive study reviewing case notes of children admitted with a diagnosis of chronic cor pulmonale seen between January 2004 and December 2014 at Korle-Bu Teaching Hospital, which is the leading tertiary hospital in Ghana. As such, children from across the country are referred to the hospital. Clinical findings included cardiomegaly, hepatomegaly and tachypnoea. Investigations performed included chest radiography, electrocardiogram and echocardiography.
Results
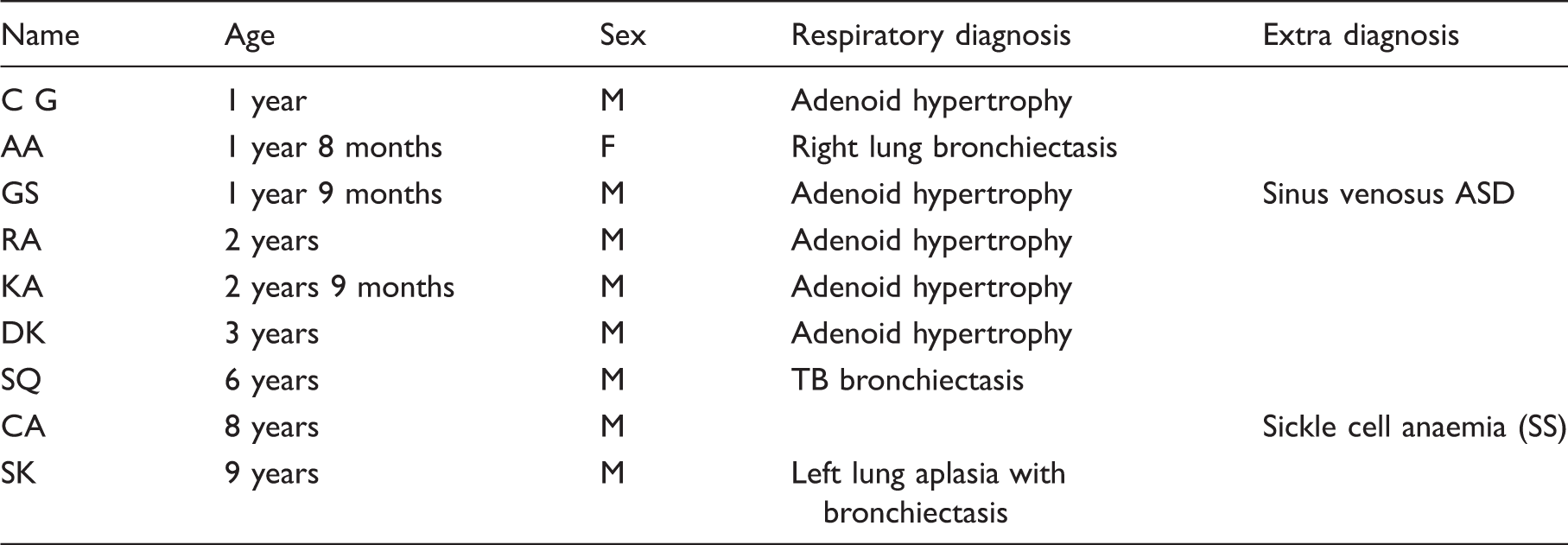
Distribution by age, sex and respiratory diseases.
Discussion
Adenoid hypertrophy was the commonest cause of chronic cor pulmonale in our study. It leads to sleep apnoea, hypoventilation, pulmonary hypertension and failure to thrive if untreated. Adenoidectomy, if done before chronic right ventricular ultrastructural changes have occurred, can lead to regression of the cor pulmonale.
The underlying common link is pulmonary hypertension. Efforts at reducing these pressures are welcome though have limited success. These include oxygen and sildafenil, which have been extensively studied. Nifedipine, a calcium channel blocker, also has a pulmonary vasculature dilating capacity. Nitric acid is an endothelium-derived relaxing factor, which is also useful. All cases were treated for heart failure with furosemide and spironolactone. The incidence of obstructive sleep apnoea and hypoventilation is similar in males and females in prepubertal children. 5 This may explain the gender bias in this study.
Congenital heart diseases were not included in the study. Genetic syndromes such as Trisomy 21 and muscular diseases need further studies to document their contribution to the disease. Korle-Bu Teaching Hospital is the leading tertiary hospital in Ghana. However, there are other tertiary and secondary hospitals where other cases of chronic cor pulmonale secondary to respiratory diseases could have been managed. This gave the authors an impetus to initiate a national registry for these cases, similar to the Spanish Registry. 7
Five of the cases with adenoid hypertrophy had adenoidectomy done which improved the cardiac status of the patients. All the cases are being followed at the departmental cardiac clinic every six months, monitoring respiratory rates, hepatomegaly, oxygen saturation and echocardiography. With the exception of one sickle cell anaemia child who has become oxygen-dependent, parameters showed improvement in the others.
Conclusion
Children with right heart failure should be investigated for pulmonary cause since early recognition and treatment would improve outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.