
Abstract
Paediatric surgical disease is a neglected health problem. Patients travel great distances to tertiary level care for management. This study aimed at analysing referral patterns to design an outreach programme for paediatric surgery in KwaZulu Natal. Data forms of patients referred to the service between January and July 2016 were correlated with the clinical record. Delays in management were compared to morbidity and mortality. Out of 781, 158 referrals were accepted as emergencies. The majority (62%) were children aged < 1 year. Gastro-intestinal problems (38.4%) and congenital anomalies (26.9%) formed the majority. Patients who died had a significantly longer delay in transfer. Longer total delay was associated with statistically significant greater morbidity. In a setting where a large rural population is served by single-centre tertiary care, delays exist and contribute to morbidity. The authors advocate the establishment of an outreach programme to address these issues.
Introduction
Paediatric surgical disease is a neglected public health problem, especially in sub-Saharan Africa,1,2 a region with a large paediatric population. In KwaZulu-Natal, 34.7% of the population of 11.1 million is aged under 14. KwaZulu Natal also had the highest number of registered births in South Africa: 328,361 in 2004. 3
Providing surgical services to these children is an essential component of public health delivery. 4
There is a general shortage of paediatric surgeons (PS) in Africa. A 2009 cross-sectional survey of the paediatric surgical workforce capacity in Africa showed that the number of PS ranged from one PS for 6 million children in Malawi (0.17 PS/million) to 120 PS for 36 million children in Egypt (1.5 PS/million). In South Africa, in 2012, there were only 37 registered PS, with seven retired or practising outside the country. The active paediatric surgical workforce therefore equates to one PS for every 2 million children (0.5 PS/million). 5
The scarcity of these resources mandates that patients in need must be referred to a specialist centre, often a great distance from the point of diagnosis. Transport infrastructure remains undeveloped and there is a lack of education and training for peripheral hospital staff in diagnosis, and safe transfer of children with surgical disease. 6
Inkosi Albert Luthuli Central Hospital (IALCH) is an 800-bed tertiary hospital in Durban within which there is a paediatric surgical service consisting of 35 beds attended by four full-time PS and five trainees. It sits at the apex of a pyramidal referral system based on 428 clinics and 198 hospitals under the management of the KwaZulu-Natal Department of Health. Like any pyramidal system, although designed to ensure that patients are managed at an appropriate level and as close to their homes as possible, this has the potential to delay patients, especially those who require tertiary facilities. Owing to a robust general surgical service within the province, and forced by the limited capacity available at IALCH, most surgery in children aged > 5 years is performed at the level of District Hospitals by surgeons who have spent a period in paediatric surgical training during their general surgical training programme. Thus, the patient profile within IALCH is highly selected and consists largely of patients with congenital abnormalities, oncological disorders, specific gastrointestinal (GI) disease such as necrotising enterocolitis (NEC), intussusception or biliary atresia, and paediatric urological problems including disorders of sexual development and renal transplantation. Of 11 health districts within the province, five coastal districts refer tertiary care patients to IALCH. The coastal district includes the major population concentration in eThekwini surrounding the city of Durban (Figure 1).
7
Map of Kwazulu Natal Health Districts and Population Distribution. From: http://medicine.ukzn.ac.za/ClinicalService/MapofKZNHealthDistrictsandPopulation.aspx.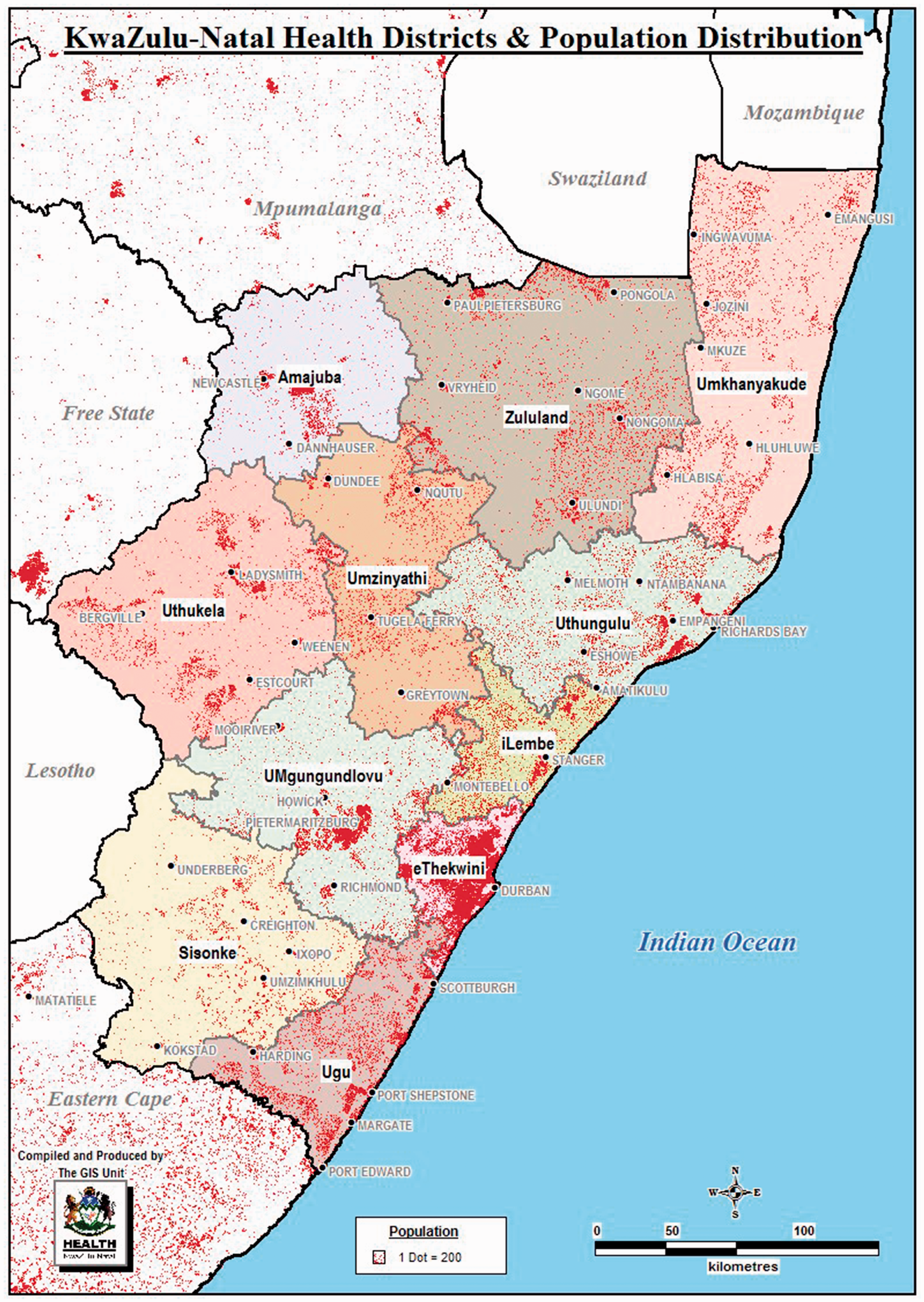
The initial contact from a referring source is by telephone. The Registrar receiving the call records clinical and demographic data onto a referral form and records the final management decision; accept as an emergency admission, as an elective clinic appointment or, if the referral is inappropriate, decline. The latter group are counselled concerning the appropriate referral destination or offered advice on management at source.
The large paediatric population, high surgical disease burden and difficult access to specialist paediatric surgical services highlight the need for an expanded paediatric surgery service.
Our study aimed at using analysis of our referral patterns to design an effective outreach programme.
Methods
The study was approved by the Biomedical Research Ethics Committee of UKZN and the Department of Health of KwaZulu-Natal.
All data forms of patients referred to the service between January and July 2016 were evaluated and correlated with the clinical record. Patient demographics and clinical data were retrieved. The time from presentation at source to initial contact was recorded (referral delay), as were the time from initial contact to arrival of emergencies (transfer delay) and the time from arrival at IALCH to surgery (resuscitation delay). The total delay was a summation of these delays.
In-hospital morbidity and mortality were extracted from clinical records.
Patients were excluded if their medical records could not be traced (n = 4). One patient died prior to transfer and was likewise excluded.
STATA v 13.1 Stats was used for data analysis. Tables were used to assess the distribution of referrals by outcome, age and referral source. Mann–Whitney tests were applied to time variables and outcome
Results
A total of 781 referral forms were analysed.
The distribution of referrals from health districts in Kwazulu Natal to the department of paediatric surgery are shown in Figure 2. The primary disposition of referrals is illustrated in Figure 3.
Number of referrals per district. Chart showing disposition of referrals.

Most of the patients discussed were aged <5 years, with the infant age group highest among the districts (Figure 4).
Chart showing the number of referrals per age group.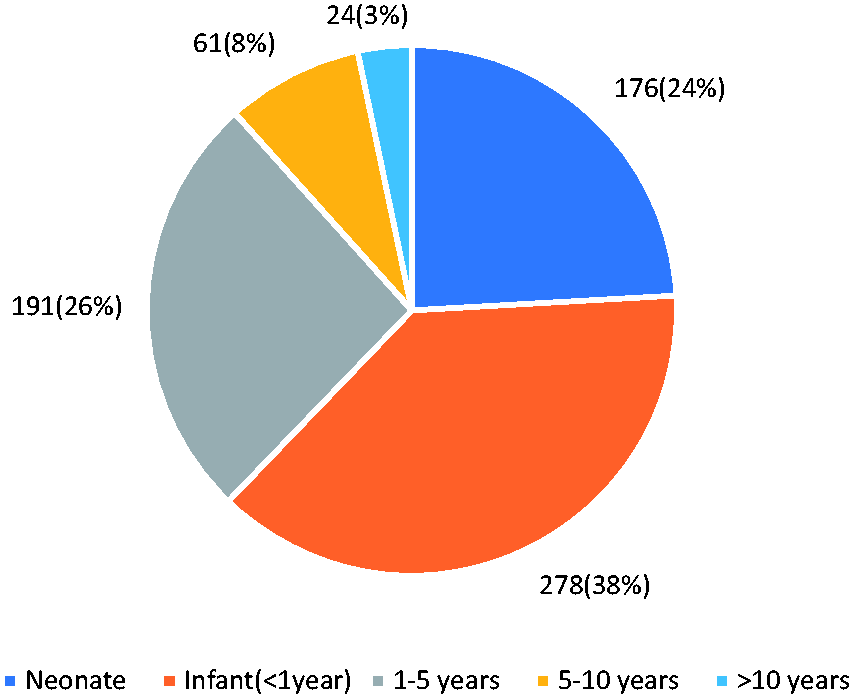
Of congenital anomalies who required emergency admission, 72.3% were neonates, while the remaining proportion were mostly infants (22%) (Figure 5).
Graph showing the number of referrals per diagnostic group.
Referral distribution of diagnostic groups.

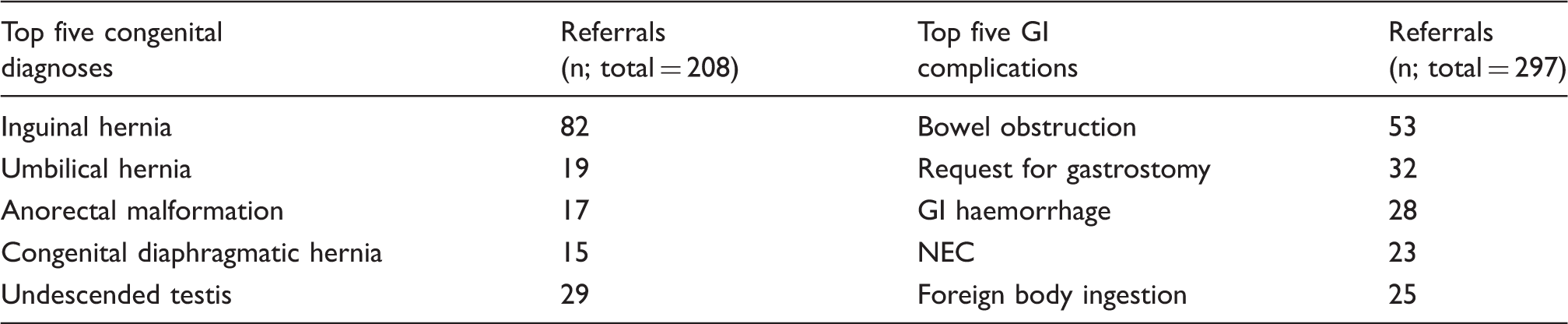
Top five problems for congenital and gastrointestinal (GI) diagnostic groups.
The distribution of diagnoses that were accepted electively is shown in Figure 6.
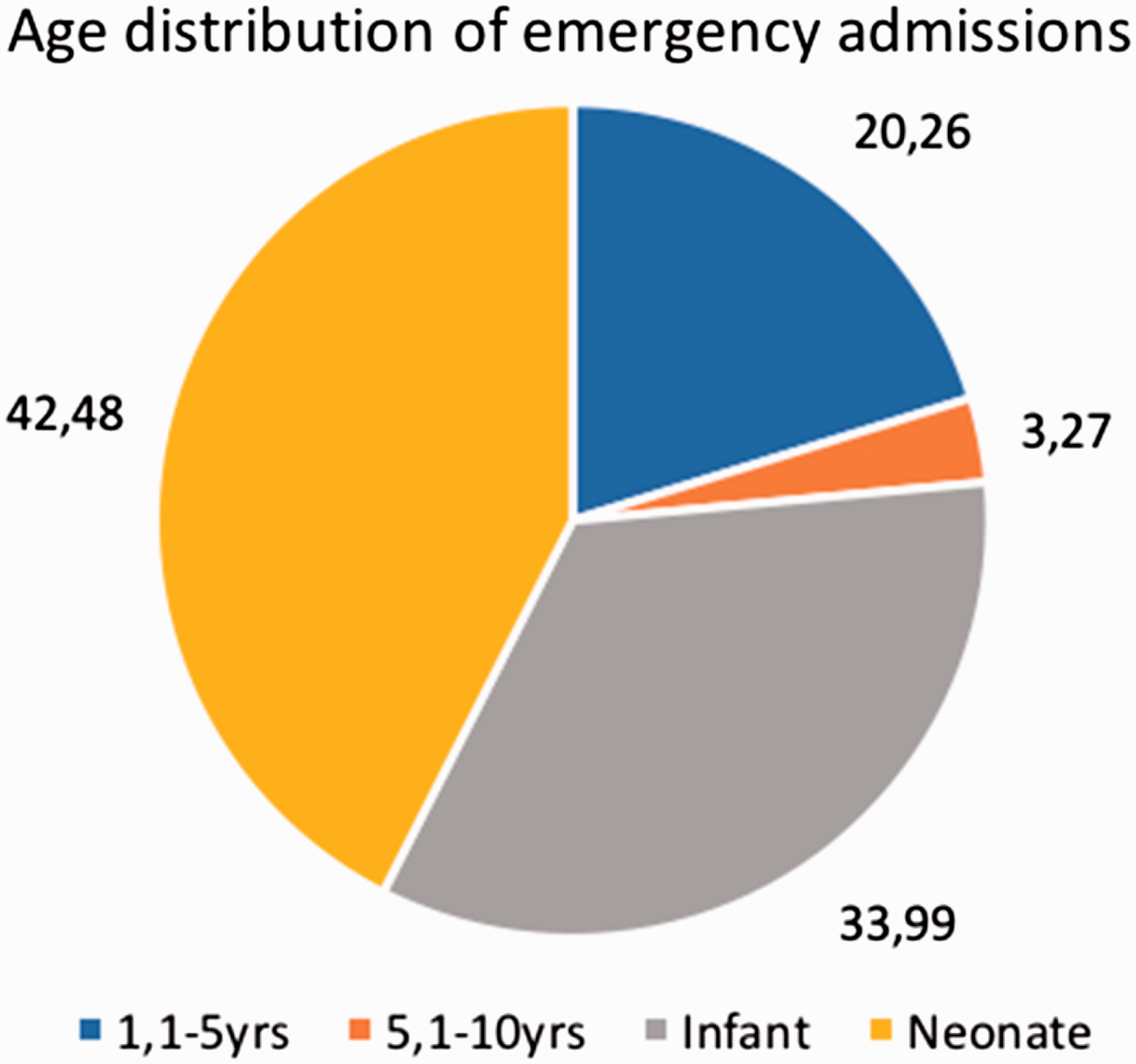
Graph showing the number of clinic referrals per diagnostic group. Chart showing the age distribution of emergency admissions.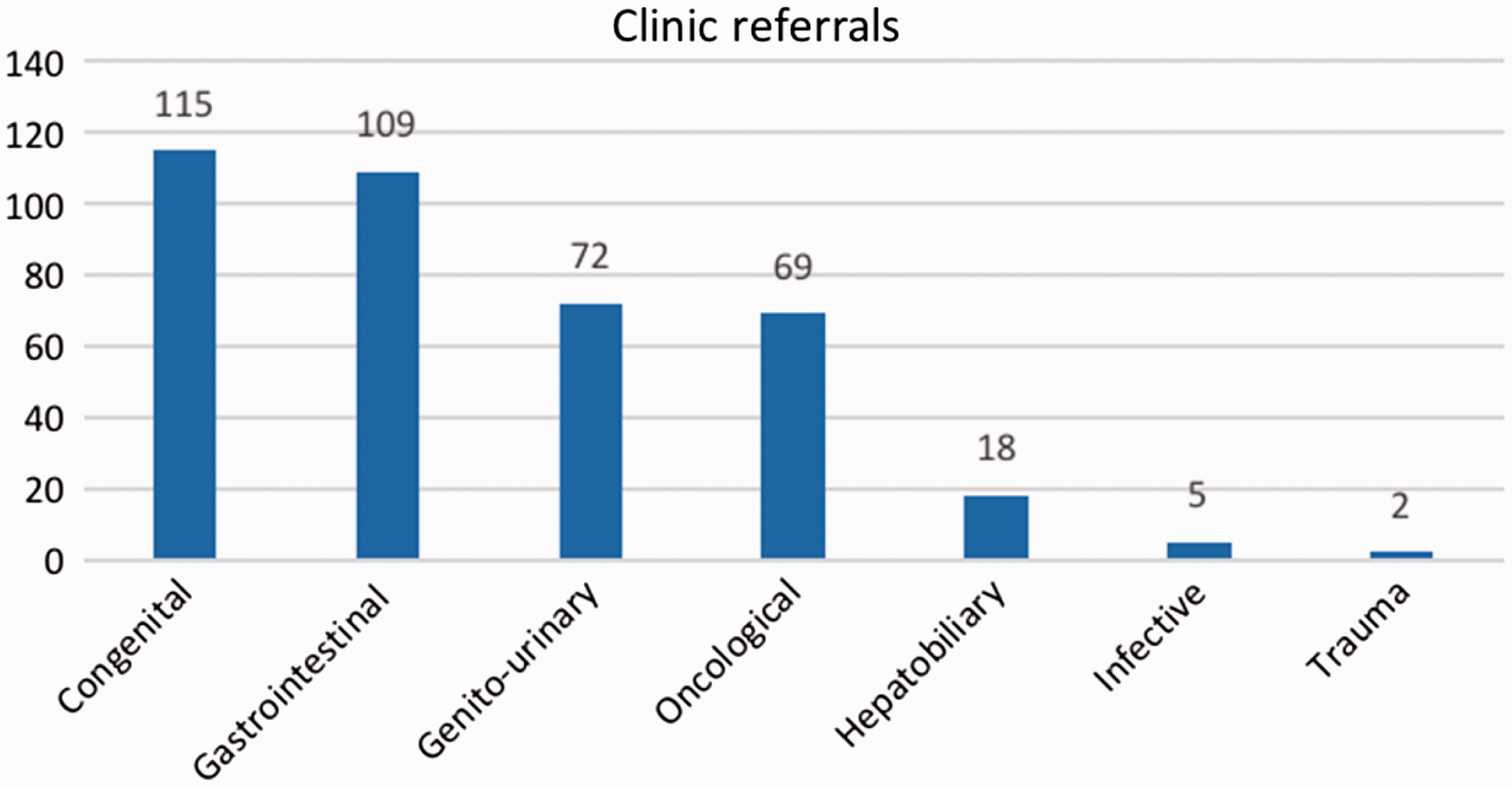
Most of the oncological (83%) and genito-urinary pathology (70%) was accepted electively. Congenital and gastrointestinal pathology were the diagnostic groups requiring the highest proportion of emergency admissions (30% and 29%, respectively).
The total number of emergency admissions was 158. Morbidities were present in 43%. Twelve (7.6%) patients died, five with congenital problems and seven with gastrointestinal problems. The age distribution of emergency admissions is shown in Figure 7.
Referral delay
There was no delay in referral for 60% of the emergency admissions. The median for children who suffered morbidity was one day (range = 0–17 days). Children who suffered morbidity during the treatment phase had a significantly longer delay in referral (P = 0.0039). The median delay in referral for children who died was 1.5 days, but was not significant compared with children who survived (P = 0.08).
Transfer delay
Transfer delay was shown to be related to mortality, but not related to morbidity. The median delay in transfer for children who died was one day (range = 0–4 days). Patients who died had a significantly longer delay in transfer (P = 0.0075). Thirty-four emergency admissions did not require surgery; 50% of emergency admissions had a total delay (from referral to surgery) of less than two days.
Resuscitation delay
Eighty percent of emergency admissions requiring surgery were operated within two days of admission to IALCH. Children with a longer time from admission to surgery had a higher rate of morbidity but this was not statistically significant (P = 0.0614). The median delay for those dying or suffering morbidity was one day (range = 0–24 days).
Total delay
Fifty percent of emergency admissions had a total delay (from referral to definitive care) of less than two days. This was shown to be directly related to morbidity (P = 0.0022). Patients suffering morbidity had a significantly longer total delay than those who did not. Children who died had a median total delay twice as great as survivors although this was not statistically significant (P = 0.095).
Discussion
There is a paucity of data regarding the epidemiology of paediatric surgical disease in sub-Saharan Africa. However, the lack of PS in the region leaves a large gap in the care of complex surgical conditions and this, along with a lack of resources and infrastructure, contributes to poor outcomes for children with surgical disease.
The first step in solving the problem of service delivery is first to identify the extent of the problem.
The epidemiology of the referrals and admissions to IALCH differs from other African centres in Sudan, Nigeria and Gambia, as the referral system and entrance criteria differ. Trauma and infective problems accounted for just three and four emergency admissions, respectively, in six months. This differs from other epidemiological studies in Africa, which list trauma and infective pathology as the top three clinical problems.8–10
Congenital anomalies and gastrointestinal problems make up the majority of IALCH emergency referrals, and the patients are mostly neonates and infants. This is largely due to the robust general surgical service offered in secondary hospitals in the region, which addresses surgical pathology including trauma and gastrointestinal pathology in children aged >2 years, and surgical infections in all age groups. This helps to alleviate the burden on the paediatric surgical unit in IALCH, which focuses on specialised surgery for congenital anomalies, and gastrointestinal pathologies in children aged < 2 years.
The burden of paediatric trauma and surgical infections is therefore not illustrated in these results, but remains an important area of concern in Africa.
The existing pyramidal referral system, along with inadequate transport infrastructure, results in frequent delay in the management of patients with complex surgical problems. These delays have significant consequences in terms of patient morbidity and mortality. It is clear that the greater the distance from source to IALCH, the greater will be the transfer delay meaning that rural patients are specifically disadvantaged.
While expanding the number and distribution of PS remains the long-term goal, there is a need for a more urgent response. These data suggest targets for educational and outreach initiatives which have so far been restricted by a lack of available personnel. The six-month period of data collection precluded the recognition of pathology, such as intussusception, that may have a seasonal variation in incidence but the majority of referred patients were suffering disorders with clearly no recognised variation.
Attempts to use video-conferencing for both patient management and education have been only partially successful with difficulties encountered in the availability of staff at peripheral institutions and in the maintenance of the technological infrastructure.11,12
The enhancement of the training and skill of transport personnel has the potential to reduce the resuscitation time by delivering a patient in a stable condition. While clearly established for neonates, the quality of care during transportation has potential consequences for all children.
Although it may be argued that the circumstances of IALCH are unique, the principle of a pyramidal referral system is generally accepted. Thus, while specific patient characteristics might vary, the principle of delay with its attendant consequences is likely to be universal. Only by reviewing referral data can the sources of these delays be defined and corrective policies introduced and the disadvantage of a rural place of origin be eliminated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.