
Abstract

Introduction
Visceral leishmaniasis (VL), also known as Kala-azar (KA), is a major health problem in certain parts of the world. In VL, a skin manifestation is commonly described as ecchymosis and purpura due to thrombocytopenia. 1 This report describes a case of VL presenting with purpura due to vasculitis.
Case report
In June 2014, a 50-year-old Bangladeshi woman presented for evaluation of her six-month history of irregular fever, significant weight loss and recurrent, painful purpuric lesions. The cutaneous eruptions were bilateral, painful, associated with leg oedema and used to disappear spontaneously. She had neither significant symptoms nor any past or family history, and she had not taken any recent medication. Physical examination revealed purpura, confined to her lower limbs (Figure 1), moderate anaemia and hepato-splenomegaly (4 cm and 8 cm from the right and left costal margins, respectively). Laboratory investigations revealed anaemia (Hb 79 g/L), normal white cell count (2 K/mcL) with normal differentials and normal platelet count (150 K/mcL). The total protein was raised (108 g/L) but albumin was low (26 g/L). The erythrocyte sedimentation rate and C-reactive protein were elevated (135 mm/h and 440 mg/L, respectively). Immuno-chromatography for VL was positive and the splenic aspirate also showed the presence of Leishman-Donovan (LD) bodies. The histopathological analysis of a skin biopsy taken from a purpuric lesion revealed leucocytoclastic vasculitis, but there was no deposition of immunoglobulin or complement in the immunofluorescence test. Serology for rheumatoid factor (RF) and anti-citrullinated peptide antibodies were positive, but antinuclear antibodies and anti-neutrophil cytoplasmic antibodies were negative. Complement levels were normal and serological markers for hepatitis B and C were also negative. Polyclonal gammopathy was detected in protein electrophoresis.
Purpura over the lower limb.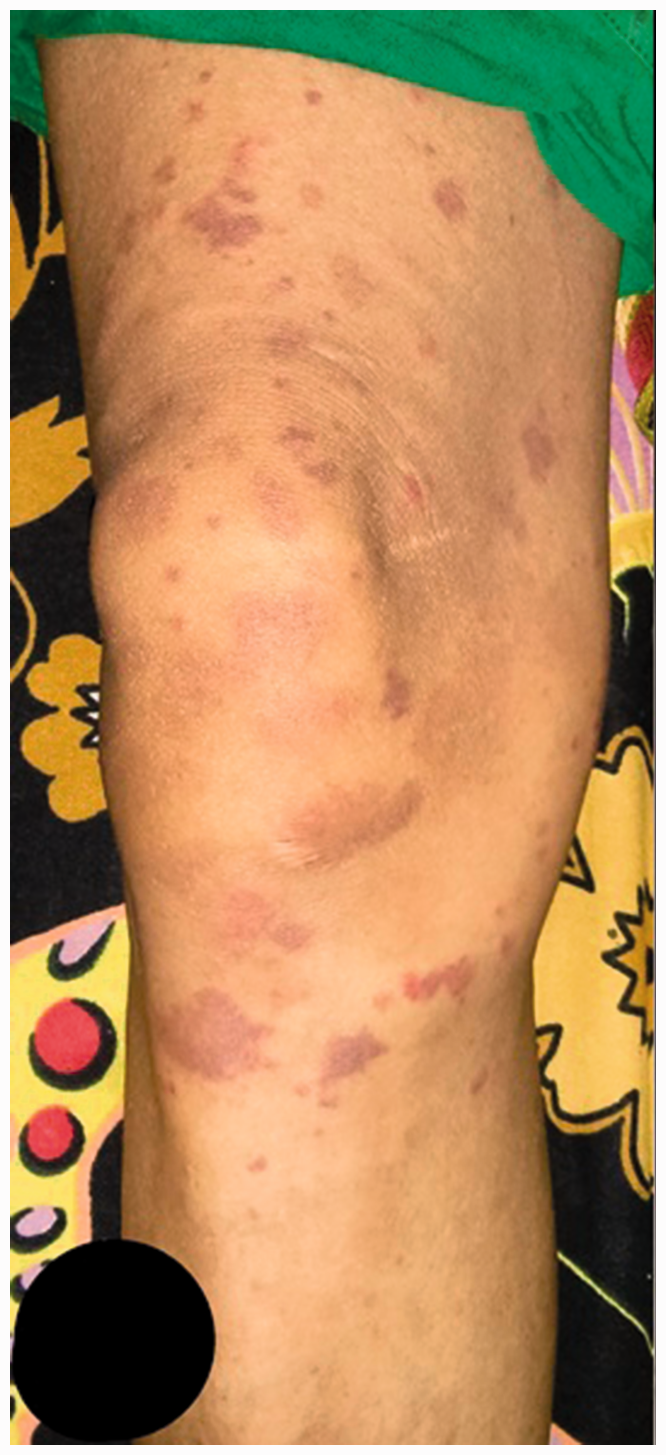
A diagnosis of cutaneous leukocytoclastic vasculitis, associated with VL, was made. Treatment with a single dose of liposomal amphotericin-B was given. The fever subsided and the rash disappeared after five days, leaving hyper-pigmented areas over the legs (Figure 2). On follow-up four months later, there was no LD-body in a repeat splenic aspirate. After eight months of treatment, both the spleen and the liver had reduced to 3 cm and 2 cm from the left and right costal margins, respectively, and there was no reappearance of purpura.
Healed lesions with areas of post-inflammatory hyperpigmentation.
Discussion
The Chapel Hill Consensus Conference defines CLA as an isolated cutaneous leucocytoclastic vasculitis, in the absence of systemic vasculitis. Small vessel vasculitis manifests usually on skin as purpura, erythema, urticaria, vesiculo-bullous lesion, superficial ulcers and splinter hemorrhages. 2 Palpable purpura, caused by extravasation of erythrocytes over the lower extremities, associated with pruritus, stinging, tenderness and burning, improves rapidly, sometimes completely, after bed rest. Areas of echymoses and hyperpigmentation are seen as the lesions resolve.2,3 Although infections have long been suspected to be trigger factors for many types of vasculitis, their causal relation is only firmly established in polyarteritis nodosa and cryoglobulinaemia in Hepatitis B and C virus infection, respectively. 4
Several mechanisms may be involved in vasculitis related to infection, viz. cell mediated hypersensitivity, abnormal immune regulation, production of cytokines such as TNF and various ILs from direct stimulation of infectious agent, type III immune complex reaction and direct endothelial cell invasion. 4 Human VL has been described in association with mixed cryoglobulenaemia and generalised autoimmune activation. 5 Type II cryoglobulinaemia has already been described in association with VL caused by Leishmania infantum. 6 Cryoglobulenaemic vasculitis is frequently associated with low complement levels, particularly C4, and visceral involvement such as neuropathy, glomerulonephritis, immunglobulin and complement rich vasculitis, which were not present in our patient.3,7 The mechanism of vasculitis in Leishmania donovani is still not well defined. The microvascular pathology in affected organs in VL has been described as sub-endothelial oedema, hyalinosis and intimal proliferation due to immune complexes. In addition, diminished nitric oxide production in vitro in VL affect microvascular function. 5 Purpura in VL by LD body due to mechanical impairment of blood vessels by the parasites has also been described as a probable aetiology. 8 As, in our patient, no immune complex in vessel wall or organism could not be isolated, any one of the abovementioned mechanisms, except type III immune complex and direct endothelial invasion, is possible.
Autoantibodies found in sera from patients with Leishmaniasis include RF (as found in our patient), anti-Sm, anti-RNP, anti-SSA and anti-SSB. The productions of antibodies against ribonucleo-proteins are induced by molecular mimicry with parasitic antigens. 6
Conclusion
It is important to remember that a cutaneous vasculitis may be the presenting manifestation of non-vasculitic disease and infection should be one of the important considerations. The treatment should be directed towards the infection, not the vasculitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.