
Abstract
The diagnosis of disseminated tuberculosis (TB) in advanced HIV infection is often delayed because of difficulty in obtaining suitable specimens for culture. A total of 32 such patients from South India with positive mycobacterial blood cultures were studied over ten years. Almost all (90%) had a febrile illness and the majority (68.7%) had clinical lung involvement, but only 27.3% had positive sputum smears. Liver biopsy yielded a positive diagnosis in only 1/7. Cytopenia was almost universal (96.9%). Bone marrow cultures were, however, positive in 54.8%, of whom one-quarter grew atypical mycobacteria. Mycobacterial blood culture is therefore a useful adjunct test to diagnose TB in advanced HIV.
Introduction
The number of cases of tuberculosis (TB) has escalated enormously, principally on account of the HIV epidemic. In advanced HIV infection, the disease is usually already disseminated which betrays a high mortality. Even at this stage, the diagnosis is often delayed because of the difficulty in obtaining suitable specimens for analysis. Our study was carried out to evaluate the usefulness of positive mycobacterial blood cultures in TB diagnosis in advanced HIV infection.
Materials and methods
Ours was a descriptive retrospective study from a review of patient records between 2005 and 2015. A total of 32 HIV-infected patients who had positive blood cultures for mycobacteria were collected from a large tertiary care referral centre in South India. All had been admitted with pyrexia of unknown origin. Blood for mycobacterial cultures were processed in Kirchner selective medium. Growth detected was subject to microscopy and subcultures were performed onto a modified Lowenstein Jensen medium to aid identification.
Details about patient demographics, clinical symptoms and signs, duration of symptoms, haematological and biochemical parameters, radiological findings, biopsies and cultures of sampled tissues and body fluids, CD4 count, HIV viral load, use of anti-retroviral therapy (ART) and species of mycobacteria identified on blood cultures were examined. Data are reported as frequencies and percentages of categorical variables and compared for significance using Pearson’s Chi-square test.
The study was approved by the Institutional review board of the Christian Medical College, Vellore on 19 April 2017.
Results
Baseline characteristics.
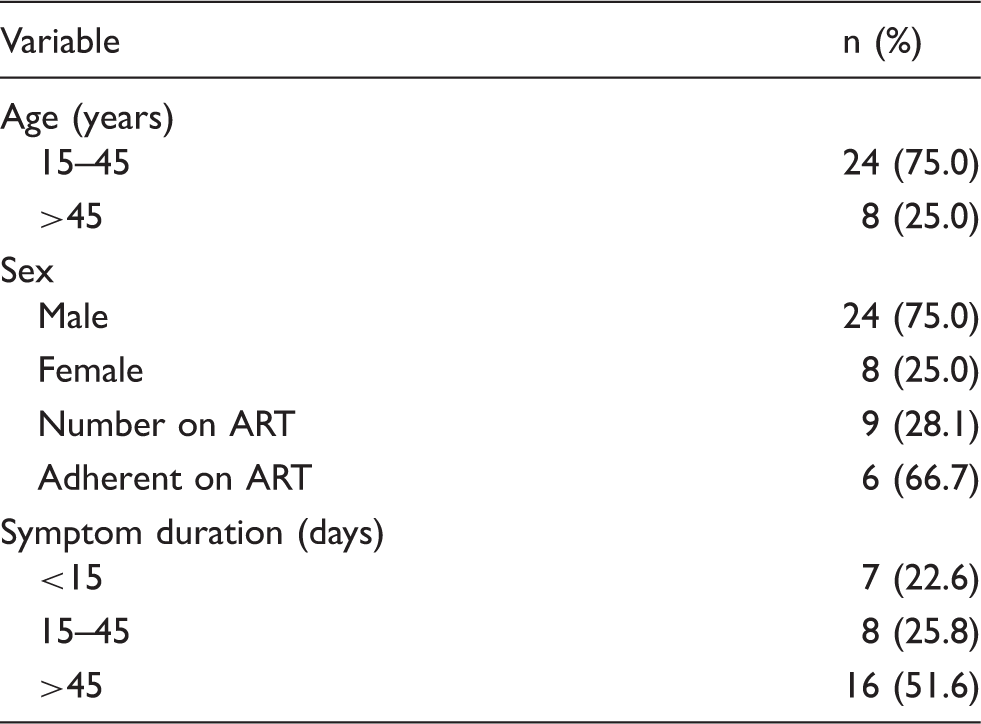
ART, anti-retroviral therapy.
ART had already been commenced in nine patients (28.12%) at the time of diagnosis of mycobacteraemia. A past history of TB was mentioned in seven patients (21.8%), and of these five (15.6%) died.
Organs involved clinically and diagnosis obtained by appropriate sampling of organ system.
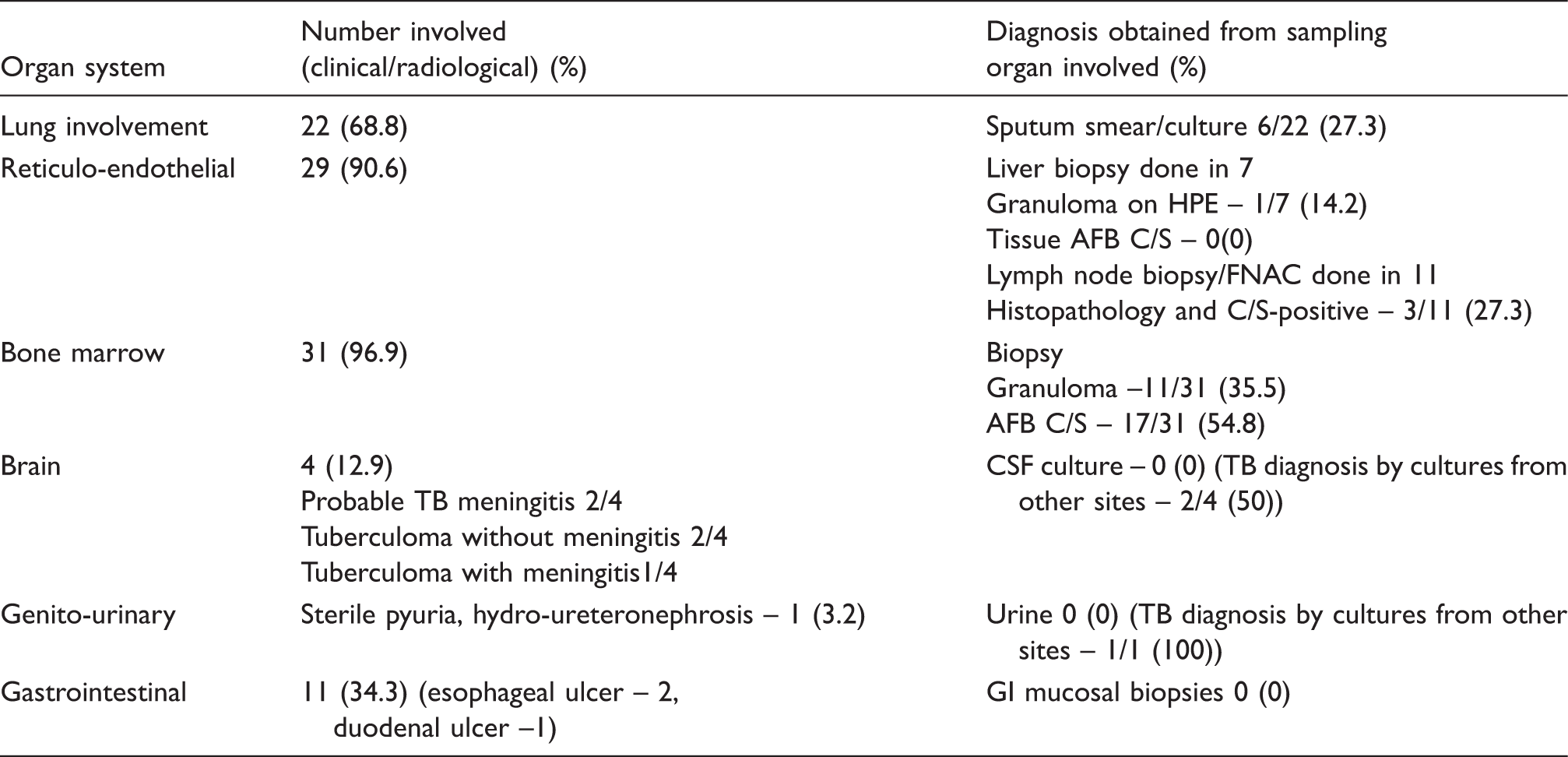
AFB, acid-fast bacilli; C/S, culture and sensitivity; CSF, cerebrospinal fluid; FNAC, fine needle aspiration cytology; GI, gastrointestinal; HPE, histopathological examination
Mycobacterial blood cultures grew Myco. tuberculosis in 13 patients (40.6%), and 19 (61.2%) had atypical mycobacteria (probably Myco. avium intercellulare in 14, Myco. simiae in one and Myco. fortuitum in four). Only one of the isolates was multi-drug resistant.
In 12 (37.5%), mycobacterial blood cultures were the only test that yielded a positive diagnosis although other sites had been sampled. Mycobacterial blood cultures as the sole diagnostic test contributed proportionately more to the diagnosis of atypical mycobacteria (10 vs. 2 cultures, P = 0.03).
The mean turnaround time for this method of culture was 55.6 days (range = 24–83 days).
Discussion
Mycobacteraemia is found in approximately 10–20%1,2 of adult patients with HIV infection. Predictors of are a low CD4 count, male gender and anaemia.1,2. TB mortality rates in the presence of HIV infection are high (17.9 vs. 3.8 per 100 person-years without TB). 3 Therefore, it is crucial to identify this pathology and initiate prompt treatment for both TB and HIV. In disseminated TB, invasive sampling is needed if involved tissue is likely to be accessed. This is a problem in a resource constrained setting; thus, empirical anti-tuberculous therapy (ATT) is usually commenced without such intervention.
The yield of mycobacterial blood cultures remains modest (14.5–30%).4–6 However, cultures are a useful adjunct especially when the yield from other tissues are poor.
The method of culture used here until recently required growth in a liquid-selective medium with subsequent subcultures onto solid media. The turnaround time was therefore high. Recently, however, with automated liquid cultures such as the mycobacterial growth indicator tube (MGIT) this has been shortened to approximately two to three weeks. The only precaution to be followed is to ensure collection of blood before the start of ATT or at least within one week of its initiation.
Given the design of the study we were unable to provide data on sensitivity and the negative predictive value of mycobacterial blood cultures for the diagnosis of TB.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.