
Abstract
Dengue fever is an acute febrile illness with a duration of 2–12 days. Our observational study observed the 24-h continuous tympanic temperature pattern of 15 patients with dengue fever and compared this with 26 others with fever due to a non-dengue aetiology.
A tri-phasic fever pattern was seen among two-thirds of dengue fever patients, but in only one with an inflammatory disease. One-third of dengue fever patients exhibited a single peak temperature. Continuous temperature monitoring and temperature pattern analysis in clinical settings can aid in the early differentiation of dengue fever from non-dengue aetiology.
Introduction
Dengue fever is a mosquito-borne viral disease associated with acute febrile illness, joint pain, headache, nausea and vomiting. 1 The duration of fever in dengue infections lasts for 2–12 days. 2 In the initial stages, symptoms mimic other acute febrile illnesses such as malaria, leptospirosis and measles. 3
Usually, body temperature in healthcare settings is recorded every 6–8 h. Missing intermittent temperature recording may obscure a significant phasic response in dengue fever.4–6 We therefore obtained, by continuous temperature recording, a 24-h pattern and compared this with fever due to other causes.
Materials and methods
Ours was an observational study, conducted in a tertiary care hospital (Kasturba Medical College and Hospital, Mangaluru). From the temperature database of 87 non-dengue cases, 26 cases (five of tuberculosis, eight of bacterial infections, seven of inflammatory and six of neoplastic diseases) were randomly selected. These were compared with 15 cases of dengue fever, selected consecutively. Thus, a total of 41 patients were screened with 24-h continuous tympanic temperature, and patterns were recorded and analysed. Individuals with a history of hyperthermia, hypo- or hyperthyroidism, non-intact tympanic membrane or other ear-related problems, treatment with antipyretics or tepid sponging were excluded.
Continuous 24-h recording was performed by a tympanic thermistor probe (Mono-a-Therm Tympanic Temperature Probe, Mallinckrodt), gently inserted into the external auditory canal projecting towards the tympanic membrane and connected to a temperature monitoring device (TherCom, Innovatecsc). 5 Recordings were taken every minute and stored in a data log for 24 h. Stored temperature readings were downloaded and were filtered using a Savitzky–Golay filter, which smoothens the signals using MATLAB software (version R2015b).
The age, height, weight, blood pressure and pulse of each patient, and number of days of fever were noted before each temperature recording. Informed consent was taken after explaining the detailed procedure of the study and risks associated. The study was approved by our institutional ethics committee.
A triple peak was defined as three separate temperature peaks, each characterized by a difference of ≥ 0.5℃ between the baseline and the peak point, observed over a period of 24 h.
Data were expressed as mean ± SD. Descriptive statistics were made using Statistical Package for Social Sciences (SPSS; version 16, Chicago, IL, USA).
Results
Summary of the demographic details of patients with different group of diseases.
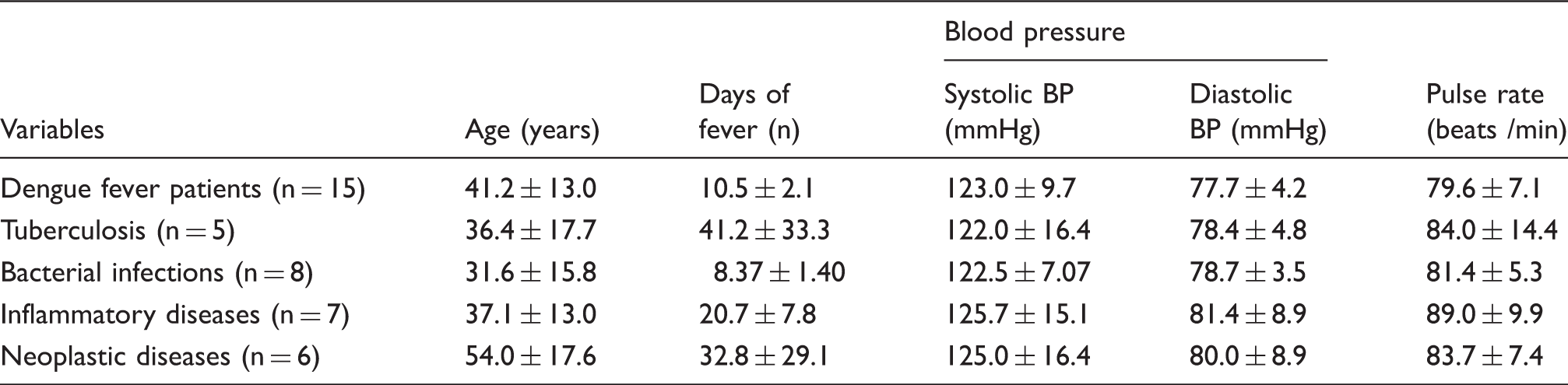
SBP, systolic blood pressure; DBP, diastolic blood pressure.
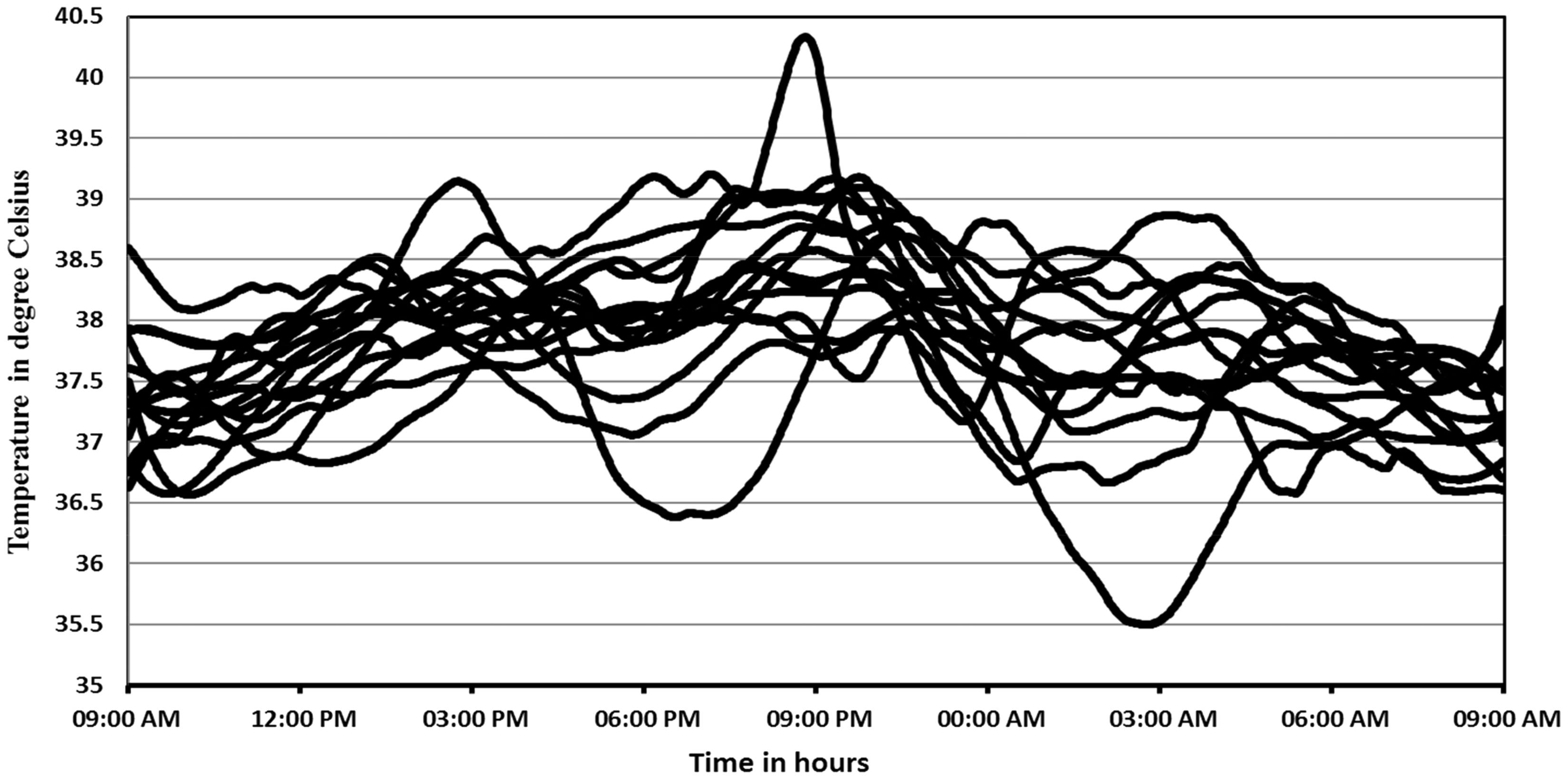
Individual temperature pattern of dengue fever cases (n = 15).
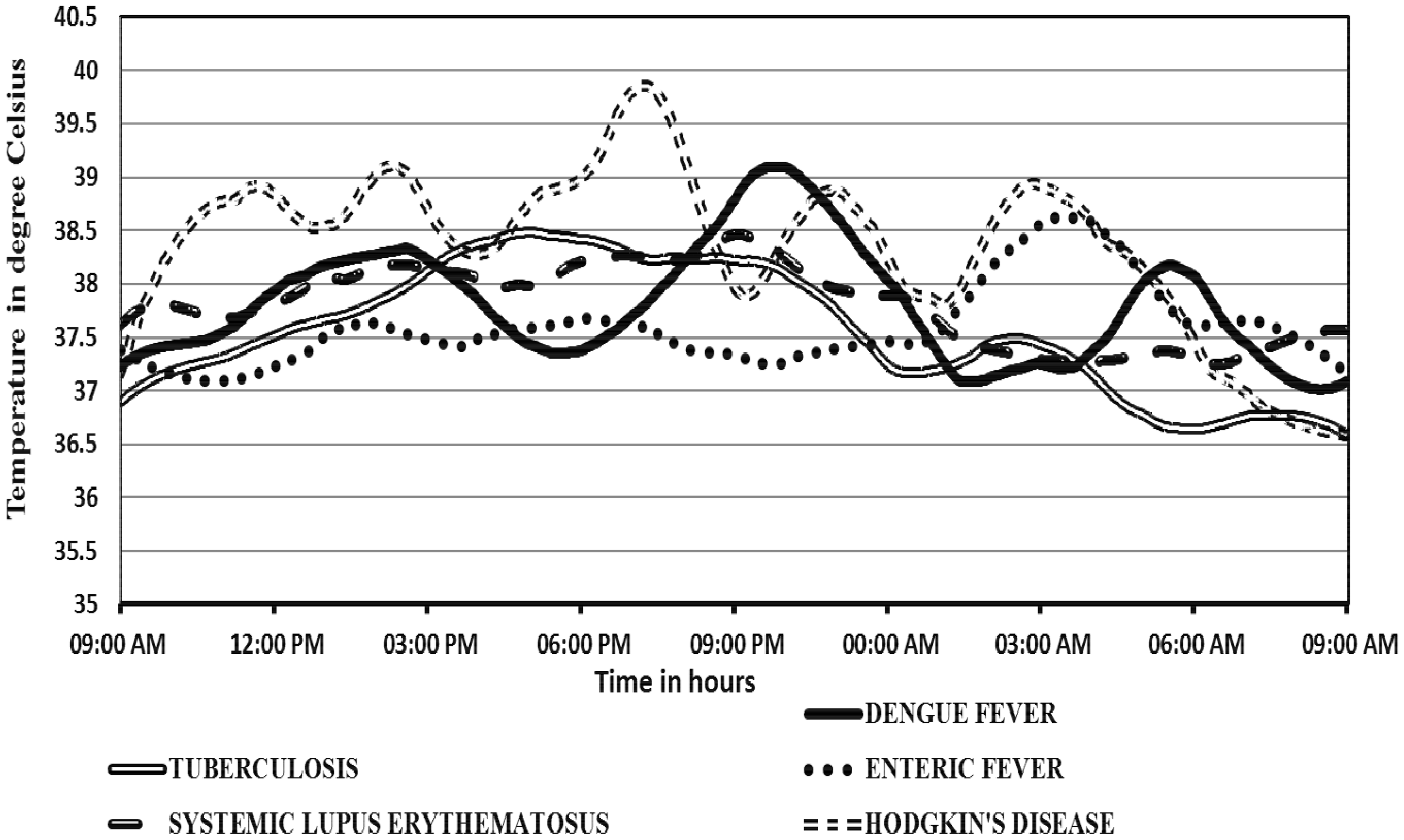
Continuous temperature patterns of individual cases over 24 h.
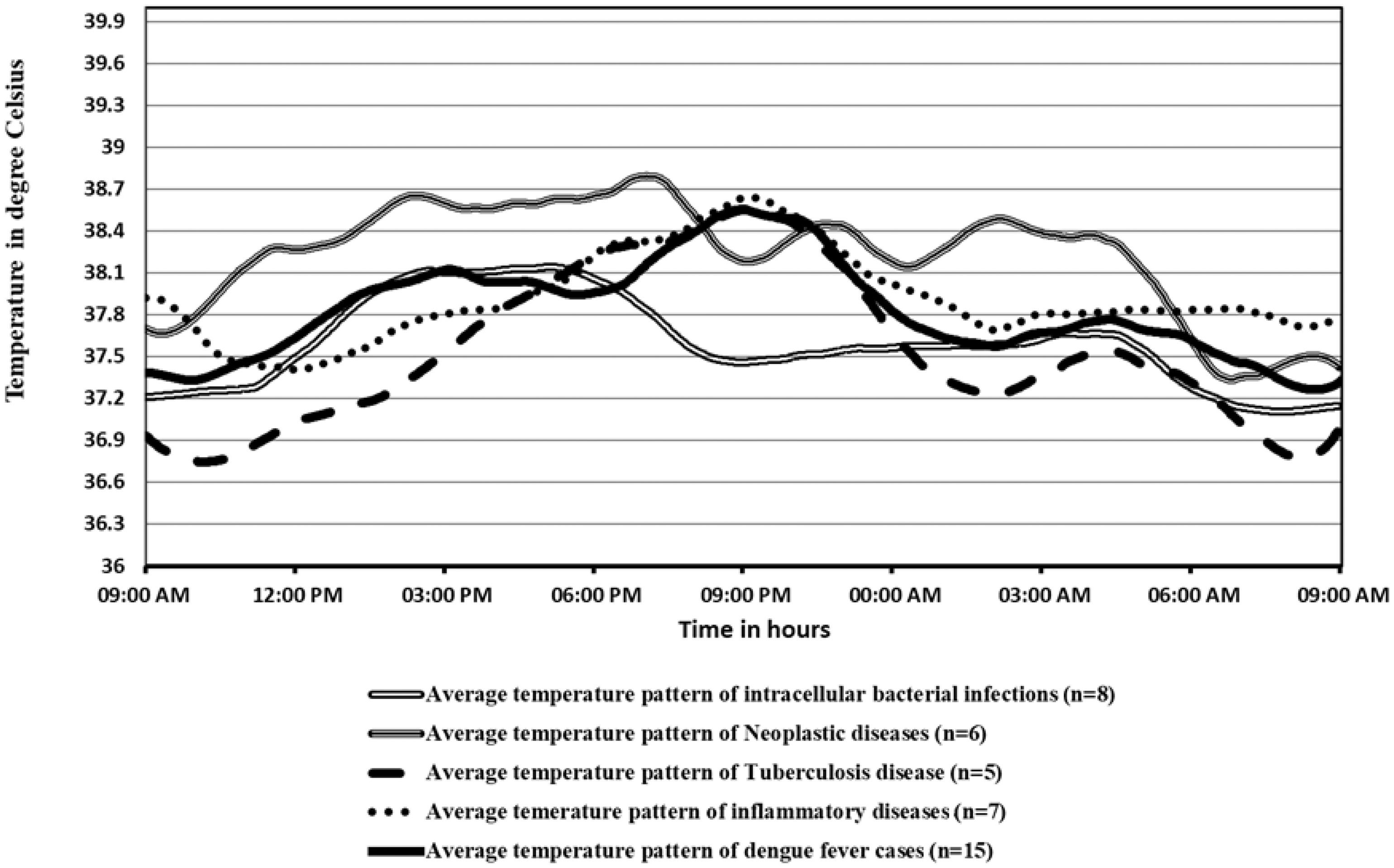
Average 24-h continuous temperature patterns in the five major categories of diseases.
Among dengue fever cases, the first mean temperature peak was 38.0℃ at 15:00, the second and third were 38.5℃ and 37.85℃ at 21:00 and 04:30, respectively. The highest temperature (38.5℃) was always the second peak.
Discussion
We observed a characteristic temperature pattern in dengue fever cases based on temperature elevation, fluctuations and number of peaks over a period of 24 h. Our study suggests that there is typically a triple peak, which is undetected by conventional monitoring methods. Detecting triple peak temperature patterns may be an adjunct for diagnosis of dengue fever.
A biphasic pattern with or without relative bradycardia has been reported in dengue fever, but is rarely considered as diagnostic.2,7 Diagnosis of dengue fever is usually made by IgM ELISA tests, which to reduce costs, are usually pooled in batches analysed once or twice a week. The resultant delay in getting confirmation may thus be offset by noting the typical triple peak temperature pattern seen.
Body temperature monitoring is simple and can give specific clues to diagnosis.5,8 Such observations have been noted ages ago,9,10 but their value may have been forgotten. Now, with the help of improved and accurate monitoring devices, there is a need to look at such cardinal signs more closely and to apply their utility in suggesting a diagnosis more carefully.
A major limitation of our study is its small sample size and another drawback is the feature extraction, which was performed visually. Appropriate computer-aided analytical tools might improve the validity and reliability of the temperature patterns seen. Further, research on dengue fever patterns may demonstrate more specific fever patterns over several 24-h periods.
Footnotes
Acknowledgements
The authors thank Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Mangaluru, for supporting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.