
Abstract

Introduction
Schistosomiasis is an endemic infection in many areas of the world.1–3 It may present with haematuria, vaginal discharge, genital bleeding, ectopic pregnancy or decreased fertility, 2 whose symptoms mimic sexually transmitted infections. Smears may even be confused with cervical cancer. Furthermore, schistosomiasis is thought to be linked with an increased susceptibility to HIV infection and sexually transmitted diseases.2,4 In the human body, Schistosoma species live in the venous plexus and may migrate to atypical sites, where they trigger an intense inflammatory reaction that may be thought neoplastic.5,6 We report a case of ovarian schistosomiasis presenting as an abdominal mass mimicking a malignant tumour.
Case report
A 51-year-old postmenopausal woman was referred because of progressive abdominal pain and distension. Her medical history was unremarkable and she seemed not to have any problems with fertility as she had had eight children. On physical examination, the left lower abdominal wall was distended by a mass with regular contours extending from the pelvis. The initial ultrasonographic assessment was suspicious for malignancy and a computed tomography scan was performed. It showed a 10-cm-thick walled cystic left ovarian mass with heterogenous necrotic contents. The suspicion of malignancy in a postmenopausal patient led to surgical excision of the mass, biopsies of the great omentum, the contralateral ovary and the abdominal wall, as well as a cytological sampling of the peritoneal fluid. Intraoperative frozen section histology of the ovarian mass was also performed. Macroscopically, the resected mass measured 10 × 5 × 3 cm with a thick smooth fibrous wall and necrotic, haemorrhagic content. Histological examination reported the thick fibrous wall to have no epithelial tissue, but wide areas of haemorrhage and calcification. No evidence of malignancy having been confirmed, surgical excision was arrested at this stage.
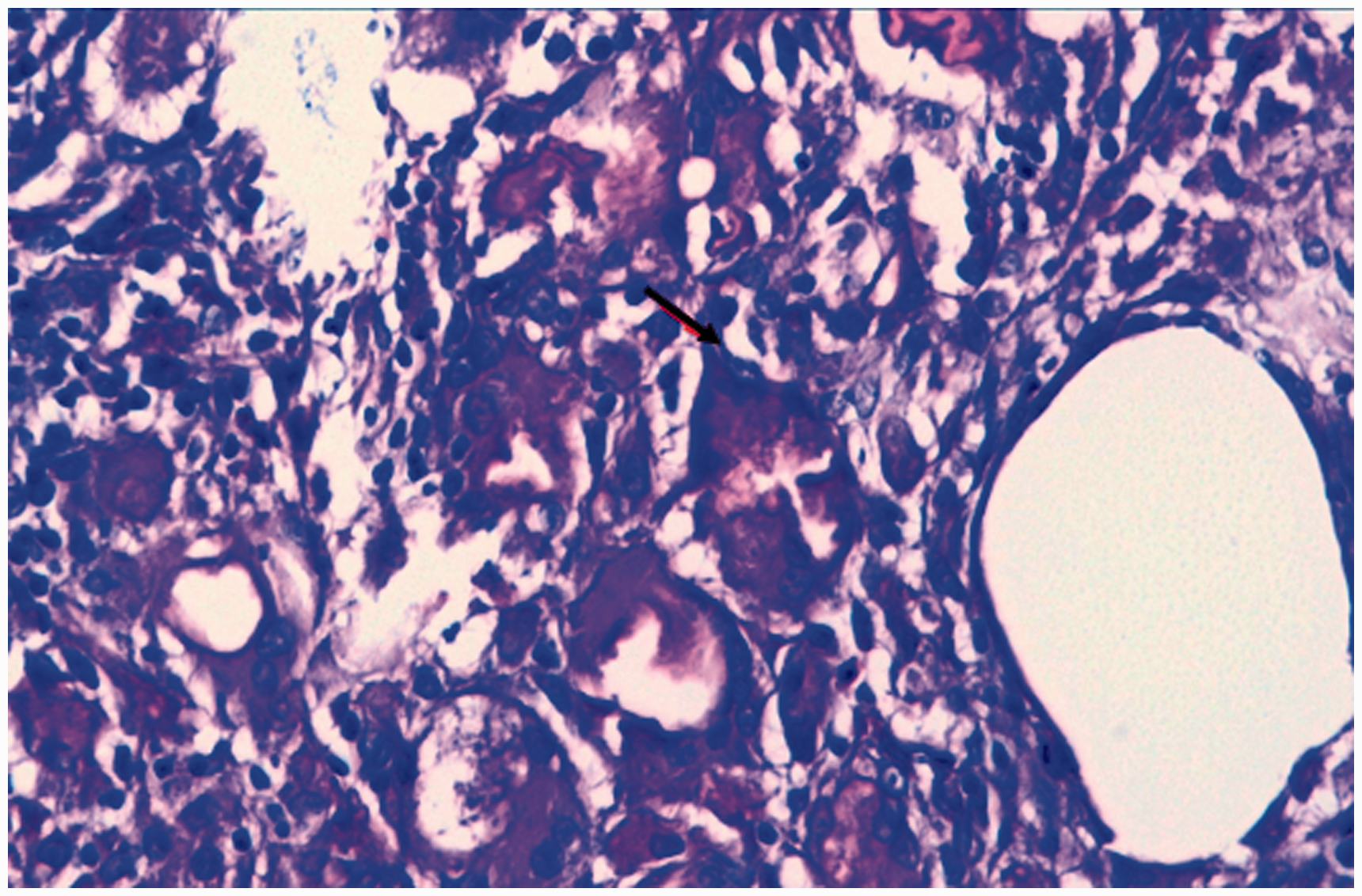
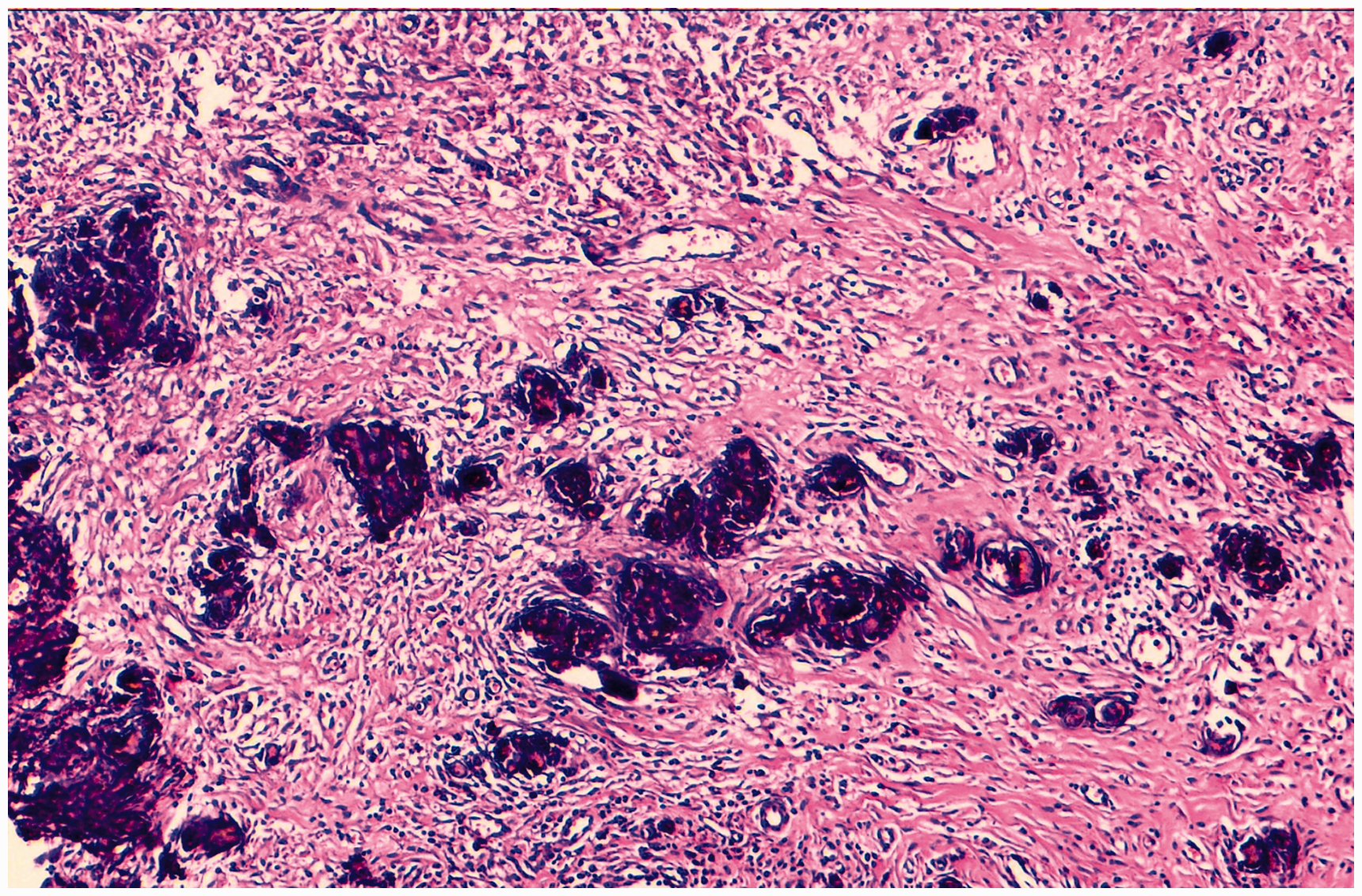
The definitive histology showed amorphous eosinophilic content within the wall, with numerous S. haematobium eggs having characteristic features (Figure 1). These eggs were predominantly found within vessels (Figure 2, black arrow) but some were calcified and surrounded by a dense inflammatory reaction (Figure 3).
The histological image of the resected specimen shows numerous Schistosoma haematobium viable eggs embedded in a thick fibrous wall with important inflammatory cells and haemorrhage (haematoxylin and eosin stain [H&E] ×200). A higher magnification showing a viable Schistosoma haematobium egg with its characteristic terminal spine (black arrow) (H&E ×400). The histological view showing multiple calcified eggs embedded in fibrous tissue and in vascular spaces (H&E ×200).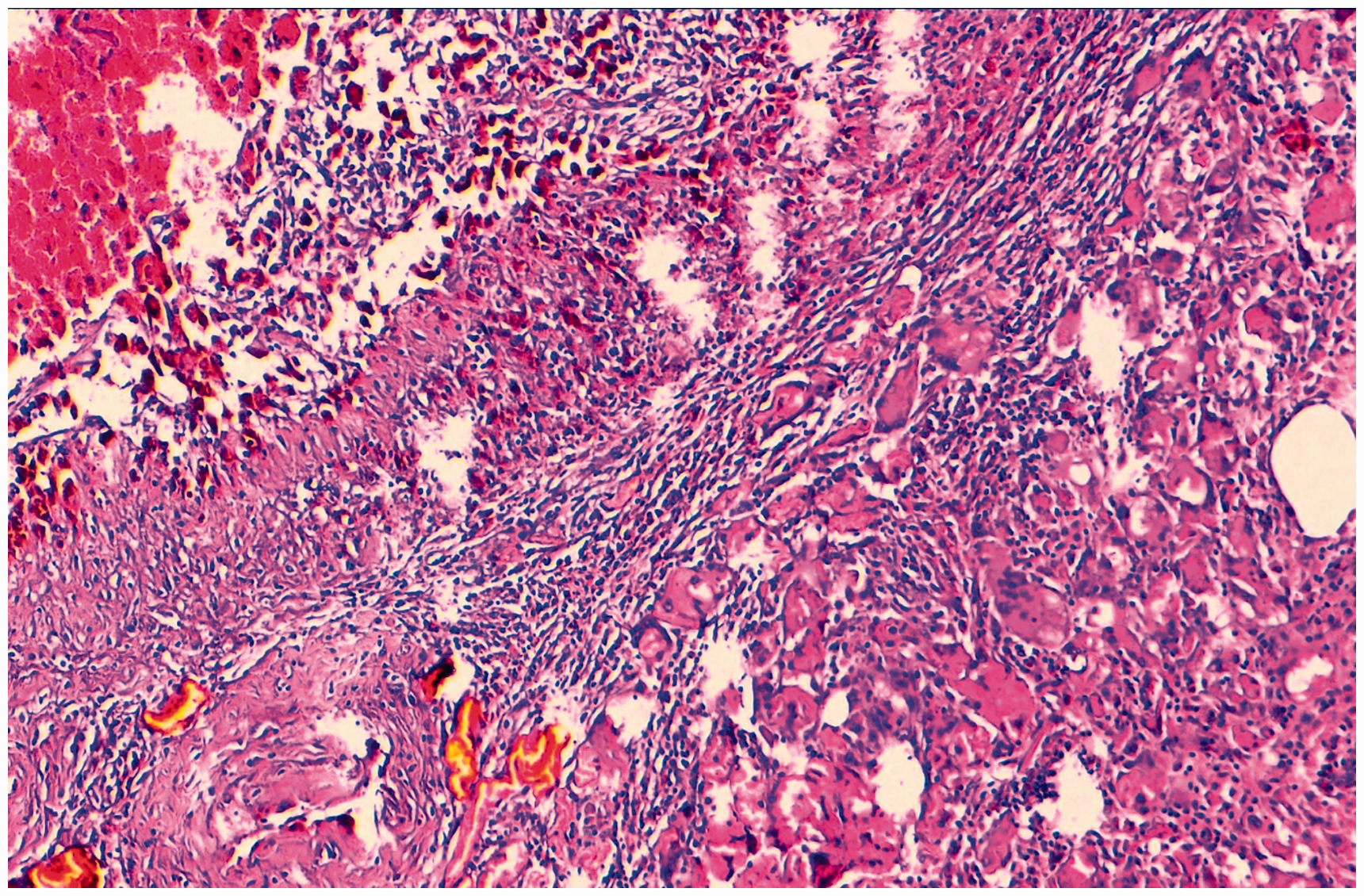
After the surgical treatment, the patient had no signs of disease and was discharged from the hospital before the definitive results of the histological diagnosis. Unfortunately, the patient has been lost to follow-up and information about her was not available after discharge.
Discussion
Despite apparent eradication of Schistosomiasis in Morocco by 2004,1,7,8 cases are still seen. While eggs are laid in the venous plexus, sometimes in the human, they penetrate deep into the tissue where they trigger an intense inflammatory reaction resulting in fibrosis and calcification. Clinical manifestations of aberrant schistosoma migration may present months to years after the initial infection.2,9 We may question whether the disease was really eradicated in Morocco, or whether it was reintroduced by an immigrant, or even whether snails might be (re)introduced by water birds.
Rare localisation of schistosomiasis often presents with misleading clinical symptoms.9–13 The only reliable diagnosis is through histological examination. 2 Confirmation can avoid inappropriately aggressive surgery for what may be thought to be a malignancy.
Despite treatment by oral praziquantel, this has no immediate direct effect on reactive inflammatory lesions surrounding the eggs. 2 These pursue their own evolutionary path and may result in neoplastic change.2,14
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.