
Abstract
Gallbladder cancer (GBC) is a rare gastrointestinal tumour. It occurs in women with pre-existing cholelithiasis. These tumours pose therapeutic as well as diagnostic challenges to treating clinicians. Early suspicion and optimal surgery for suspected GBC results in the best outcome. We describe two cases of metastatic GBC initially treated by simple cholecystectomy for gallstone despite disease pointers towards a malignant pathology. Subsequent presentation was with histopathologically proven metastatic GBC. In an area of high gallsone prevalence, a high index of suspicion and correct management of patients with suspicion of GBC is mandatory.
Introduction
Gallbladder cancer (GBC) has, in general, a dismal prognosis. These tumours are rare in the western world,1,2 but are not uncommon in the Indo-Gangetic belt in Northern India which is an endemic zone for gallstones.1,2 GBC commonly involves the female patient. 2 Neglected gallstones are virtually ubiquitously found and are the most common predisposing aetiology. Unfortunately, GBC is usually diagnosed at a late stage, 3 but readily available ultrasound has increased the pickup rate, especially of early tumours. Both surgeons and radiologists should have a high index of suspicion for their early detection. This means being aware of subtle findings of the imagery. If unsuspected, and a patient is subjected to simple cholecystectomy 4 rather than a more oncologically appropriate radical procedure, postoperative spread of cancer is inevitable. 5
Case reports
Patient 1
A 70-year-old woman presented with complaints of a swelling in the epigastric region present for eight months (Figure 1). This started as a small nodule and progressively increased in size. She had undergone a laparoscopic cholecystectomy at a distant centre. On examination, she was icteric and had an epigastric mass which was 5 × 5 cm in size, infiltrating underlying muscle, hard in consistency and immobile. There was an epigastric laparoscopic port scar in the skin. Review of the patient’s preoperative ultrasonogram revealed multiple calculi in a gallbladder with irregular thickening of its wall. Histopathology of the specimen had confirmed a well-differentiated adenocarcinoma infiltrating into muscle.
Clinical photograph of the port site swelling.
At our institute, a contrast-enhanced computed tomography (CECT) scan of the abdomen was performed, which revealed an extensive tumour in the gallbladder fossa with encasement of the common hepatic artery and portal vein. There was bilateral intrahepatic bile duct dilation, with multiple nodules in the anterior abdominal wall at the port site (Figure 2). There were also extensive metastases in the omentum, mesentery and peritoneum (Figure 3). All these findings confirmed extensive metastatic disease. All we could offer was palliative care after biliary drainage.
CECT of the patient showing the nodule along with the metastasis. CECT showing the mesenteric and omental deposits.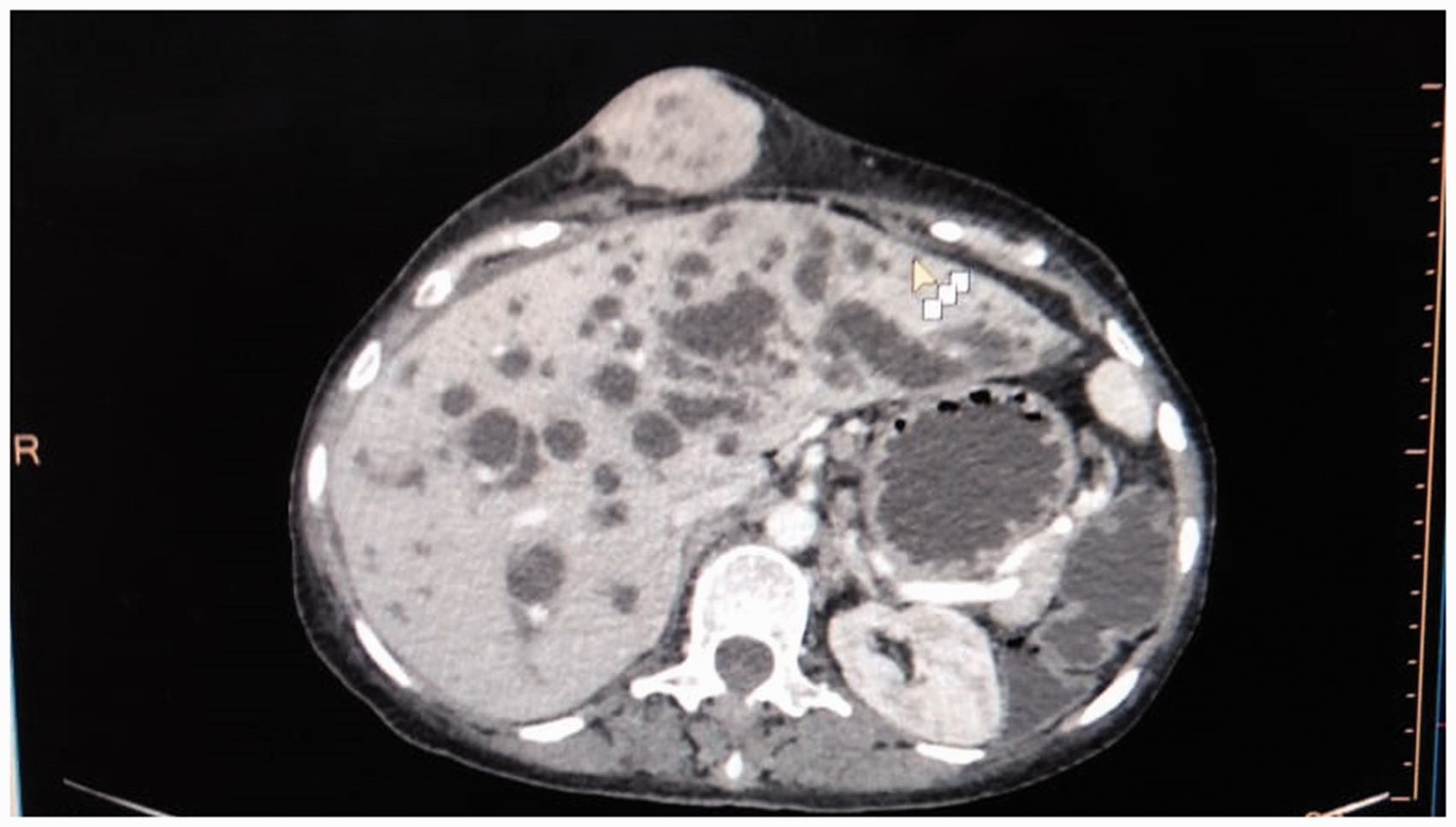

Patient 2
A 67-year-old woman presented to a peripheral centre with abdominal pain and vomiting. Evaluation by ultrasound showed a mass in the gallbladder fossa along with stones. A CECT scan confirmed the mass in the gallbladder fossa, but found no portal or periportal lymphadenopathy, no ascites, omental nor peritoneal deposits suggesting metastases. A laparoscopic cholecystectomy was carried out and histopathology confirmed a muscle invasive T2 GBC. She was then referred to our centre one month later. A repeat abdominal CECT scan revealed multiple omental, peritoneal and port site deposits (Figure 4). She was likewise counselled and offered palliative care.
CECT of the patient showing the metastatic deposits.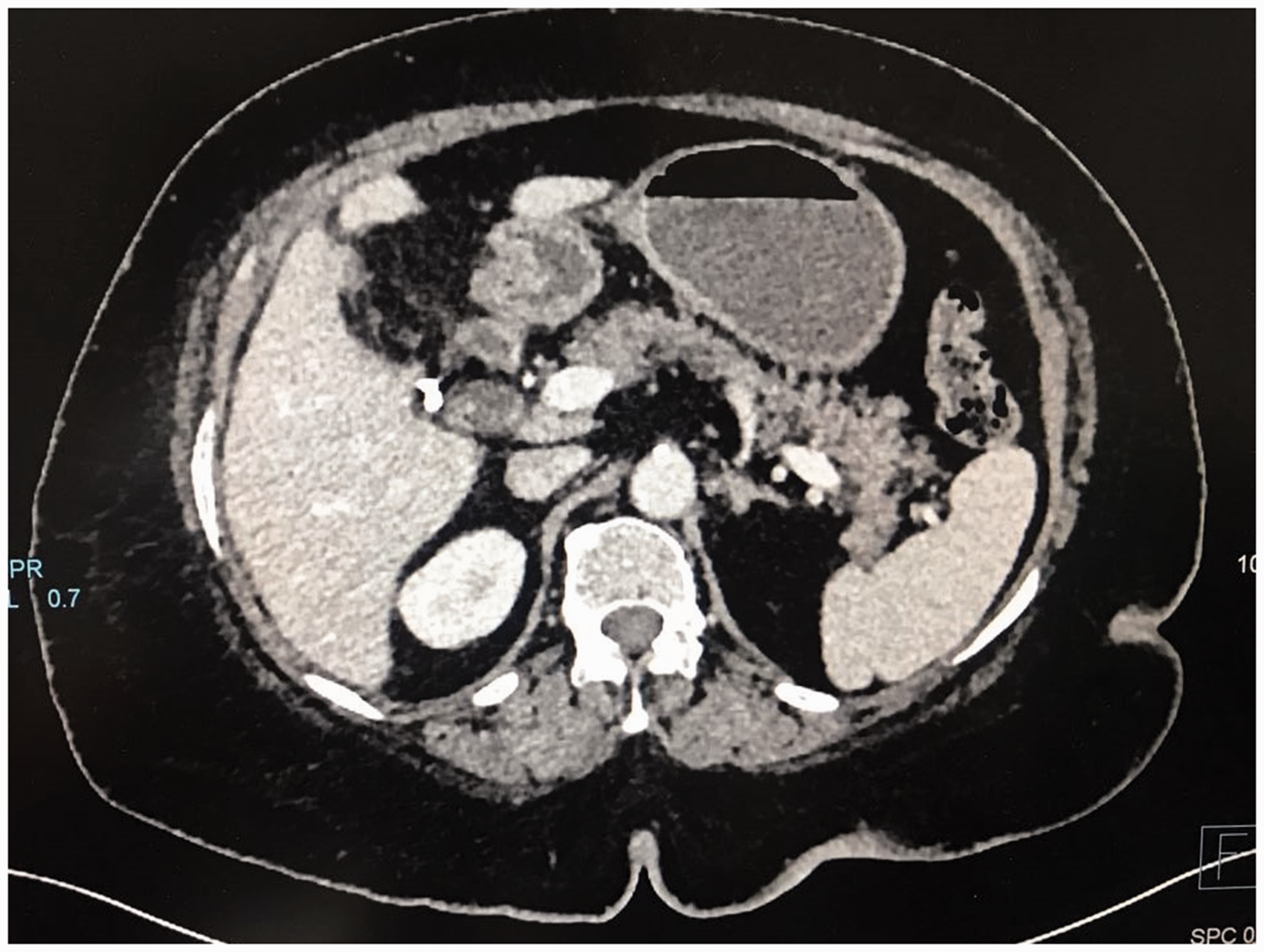
Discussion
GBC is a pathology involving the extrahepatic biliary system. 1 It is rare but a high incidence is reported from Chile, Japan and Northern India along the Indo-Gangetic belt.1,2 GBC carries a high mortality rate as most patients are diagnosed late. 3 Large gallstones have been implicated as the most common association. Chronic irritation is proposed as leading to atypical hyperplasia and then carcinoma. 6 Other aetiology proposed includes typhoid carriage, porcelain gallbladder, an anamolous pancreato-biliary junction, choledochal cyst and oriental cholangio-hepatitis.2,7 Many of these are neglected conditions in the Asian subcontinent.
GBC usually presents as right upper quadrant pain with weight and appetite loss. 4 These features are also associated with non-malignant conditions such as gallbladder tuberculosis, xanthogranulomatous cholecystitis as well as chronic repeated cholecystitis. 8 A non-malignant aetiology is far more common than cancer. This biases the treating physician into omitting to search for clinical signs such as ascites, a blummer shelf and the presence of a Virchow’s node. 8 These though are advanced signs of GBC.
Nonetheless, practically every patient with right upper quadrant abdominal pain is subjected to an abdominal ultrasonogram. The presence of gallstones, a uniformly thickened gallbladder wall and surrounding fluid establish the diagnosis of acute cholecystitis. Subtle findings such as irregular wall thickening, the presence of a mass, infiltration into the adjacent liver and the presence of hepatoduodenal lymph nodes should alert the surgeon to the diagnosis of underlying malignancy. 9 The presence of ascites along with non-contiguous liver metastases make the diagnosis of metastatic disease more obvious. 8 All patients with a suspicion of GBC should be offered CECT scanning 3 which can more accurately describe the extent of the cancer.
Positron emission tomography CT (PET scan) sensitivity in picking up residual GBC was 78% 10 and extrahepatic metastasis 50%. It has a low sensitivity for picking up a small extahepatic carcinoma, thus a diagnostic laparoscopy may be indicated as small peritoneal metastasis or liver nodules are often missed on cross-sectional imaging 11 and may prevent an unnecessary laparotomy in 33% of patients. 12
A patient suspected of having GBC should not undergo laparoscopic cholecystectomy, as it has an iatrogenic threat of tumour dissemination. 5 The chimney effect of laparoscopic ports has been implicated as inducing tumour dissemination and port site metastasis. Moreover, simple cholecystectomy, when performed on a patient with GBC, violates standard oncological practice. 13
Preoperative biopsy of GBC may cause rapid needle seed tracking and peritoneal dissemination. Radical extended cholecystectomy (resection of the liver wedge along with lymphadenectomy) offers the only chance of cure. 13 A more radical procedure in the form of hepatopancreatoduodenectomy may be performed when the pancreatic and retropancreatic lymph nodes are not resectable. 14 The role of surgery in patients of positive aortocaval nodes is highly debatable. Many studies were unable to find any survival benefit in patients with aortocaval positive disease. 15
Further management of truly incidental GBC detected after cholecystectomy will depend upon the T staging of the tumour. For T1a and Tis, simple cholecystectomy should suffice and no further surgery is required. However, T1b and above mandate a radical procedure. 13
Both of our patients had T2 disease so radical surgery was always required. All patients without any evidence of systemic metastasis should be offered a chance of possible resection. The strategy in these patients should be a diagnostic laparoscopy followed by open extended cholecystectomy. 3 Incomplete excision without adequate lymphadenectomy will result in early recurrence and a dismal prognosis. N2 lymph nodes along the coeliac axis should be removed in T2 disease but resection offers no benefit in T3/T4 disease. 15
The survival rates in patients with GBC depend upon the T staging of the tumour. Reported five-year survival rates are 100% for pT1, 49% for pT2 and 0% for pT3/T4 disease. 15 Both our patients had stage pT2 disease on histopathology, so a five-year survival rate of 50% was expected for them, had they been correctly managed.
Neoadjuvant chemotherapy (NACT) in the form of gemcitabine and platinum-based compounds increase the resectability rate of GBC. The response of tumours to NACT is 67%, and survival rates were better in those who underwent surgery compared to those who did not. 16
Conclusion
GBC is a disease with high mortality. A high index of suspicion, especially in an area of very high gallstone incidence, is required. Every suspicious ultrasound image should be followed by CT imaging. NACT and radical surgery in a patient with suspected GBC offers the best chance of cure for suitable T stages. Neglected GBC has, alas, of late become an important cause of mortality in the northern states of India.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.