
Abstract
We present an unusual case of fever of unknown origin with bilateral adrenal masses in a patient with compensated chronic liver disease (compensated) due to hepatitis C who had been treated elsewhere with four months of anti-tuberculous therapy for suspected disseminated tuberculosis (TB). At our institution, he underwent a CT-guided biopsy of the adrenal lesion which to our surprise did not reveal any evidence of TB but a close mimic.
Introduction
A familiar dictum in tropical countries is to consider the diagnosis of tuberculosis (TB) in a patient with fever of unknown origin until proven otherwise. Often, in resource-limited settings, a response to a trial of empiric anti-tuberculous therapy (ATT) is used as a means to prove TB. However, chronic granulomatous diseases such as invasive fungal infections and sarcoidosis have clinical features resembling disseminated TB. Thus, it is imperative that an attempt is made at a definite diagnosis.
Case report
A 38-year-old man from the state of Madhya Pradesh in central India, from a low socio-economic background, a clerk by occupation, presented in 2016 for chronic fatigue and malaise. He was then diagnosed with chronic liver disease related to hepatitis C with no features of hepatic decompensation. He achieved a sustained virologic remission having been treated with sofosbuvir and ledipasvir.
He later presented to our centre in April 2018 with a 6–7-month history of fever, loss of appetite and weight loss. He also reported a mild cough with scanty white mucoid sputum. Besides the compensated chronic liver disease owing to hepatitis C, there was no significant past medical history. He did not smoke or consume alcohol. There was no history of high-risk sexual behaviour or illicit drug use. There was no travel outside the state of Madhya Pradesh except to our hospital in Hyderabad. There was no contact with a case of TB. He had been started elsewhere on empiric ATT and had been on treatment for four months with no response.
On examination, he had hepatosplenomegaly. Respiratory examination was normal.
An HIV ELISA test was negative. Blood counts, renal and liver function tests were normal except for low serum albumin (28g/L). His chest radiography was normal. A computed chest tomography (CT) scan did not reveal any nodules or infiltrates, and pulmonary function testing revealed early small airway obstruction. Arterial blood gas analysis was normal with no hypoxia.
With a strong suspicion of TB, the patient underwent CT scanning of the abdomen which showed features of chronic liver disease with portal hypertension, a 6.4 × 4.6 × 4.5 cm mass in the left adrenal gland, a 2.3 × 1.7 × 1.2 cm mass in the right adrenal gland, cysts in both kidneys, splenomegaly and multiple pre-and para-aortic lymph nodes of 2.0 cm size.
There were no clinical features to suggest pheochromocytoma or Cushing’s syndrome including normal urine and serum catecholamine levels.
Biopsy of the adrenal lesion showed histiocytes loaded with intracytoplasmic encapsulated organisms with small basophilic bodies with clear halos (Figure 1, top left panel). The microorganisms were periodic-acid Schiff stain positive (Figure 1, top right) and Grocott-Gomori’s methenamine silver stain positive (Figure 1, bottom). These features are diagnostic of histoplasmosis.
Histiocytes loaded with intracytoplasmic encapsulated organisms seen as small basophilic bodies with clear halos around in the top-left panel (haematoxylin and eosin), periodic acid-Schiff stain (top right) and Grocott’s methenamine silver stain are positive (bottom).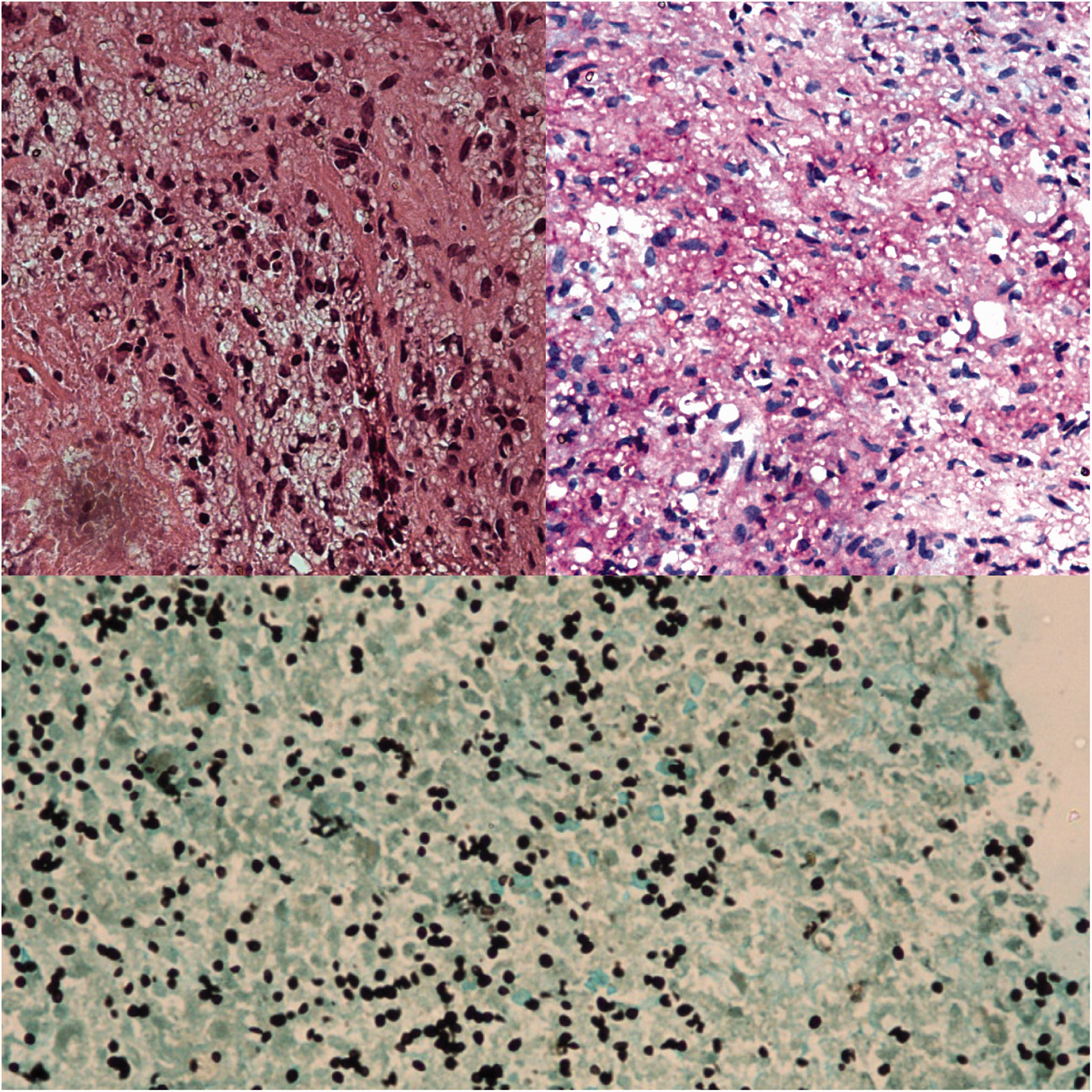
Serum galactomannan was positive. The patient received 300 mg of liposomal amphotericin B (5 mg/kg/day) daily for 10 days followed by itraconazole 200 mg twice daily. A short Synacthen test revealed adrenal insufficiency for which patient was started on prednisolone.
On follow-up, he was doing well with resolution of his symptoms; a limited PET-CT of the adrenal gland showed significant resolution of the lesions after three months of therapy.
Discussion
A study published in 1975 showed that histoplasmosis had been isolated from the soil in the West Bengal, but even in this area, only one out of 212 samples tested positive. 1 From the state of Madhya Pradesh, where our patient resided, a case of disseminated histoplasmosis initially suspected to be laryngeal carcinoma has been reported. 2
Worldwide, by far the most common manifestation in 90–95% of cases of histoplasmosis is an asymptomatic or a viral pneumonia syndrome. In India, histoplasmosis has been reported mostly in immunosuppressed patients with HIV and diabetes mellitus, with subacute progressive disseminated histoplasmosis being the most common form, as in our patient. 3 Bhansali et al. described an Indian case series of five cases of adrenal histoplasmosis (from non-endemic areas) with Addison’s disease. 4
It is interesting to note that our patient was neither infected with HIV nor suffering from diabetes mellitus. Bilateral adrenal histoplasmosis has been reported in an ‘immunocompetent’ man from Texas, USA, 5 but the patient described was hepatitis C-positive (as ours) and had a history of 40 pack-years of cigarette smoking (unlike ours).
Histoplasmosis has been infrequently reported in patients with hepatitis C. One patient with chronic hepatitis C was found to have gastrointestinal histoplasmosis. 6 A case of isolated nasal histoplasmosis in a patient with hepatitis C-related cirrhosis has been described. 7
Conclusion
Invariably, the disseminated form of histoplasmosis manifests similarly to TB. A high index of suspicion is required. Treatment for histoplasmosis is life-saving and patients respond well to antifungal therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.