
Abstract
Malnutrition continues to be a major killer of children, predominantly in low- and middle-income countries such as India. An ecological study was undertaken to correlate different demographic factors with the prevalence of underweight children. Based on findings from the National Family Health Survey 4 (2015–2016), 81 districts were analysed from three states in the eastern part of India. The findings suggest that female literacy (r = −0.556) and improved sanitation (r = −0.741) reduces the burden of malnutrition. Regarding childbirth, four antenatal visits (ANC), institutional deliveries, full immunisation, early breast feeding and adequate diet also reduce the degree of malnutrition among children. For preventing malnutrition, emphasis should be laid on improving social determinants and maternal health awareness.
Introduction
Undernutrition has been a persistent global health challenge for decades. It has been linked with 45% of child deaths in 2011 and is linked with mental retardation and cerebral palsy.1,2 Worldwide, 17.3 million children are suffering from severe wasting. 3 The World Health Assembly in 2012 planned to reduce the global burden of malnourishment in children aged <5 years by 40% by 2025 from a pool of 171 million in 2010. 4 Sustainable Development Goals (SDG) aim to end all forms of malnutrition by 2030. 5
India, which has >30% of all global stunted children aged <5 years, managed to reduce the prevalence of malnutrition from 42.5% to 35.7% over the last decade.6,7 Improved socioeconomic conditions, a reduced burden of infectious diseases, and changes in treatment modalities and their approach were the key factors. In spite of this continuing progress, the country still carries the burden of 8.1 million children suffering from severe acute malnutrition. 8 Poor sanitation, the practice of open defecation and repeated infections (diarrhoea, pneumonia, malaria and worm infestations) have been implicated as the cause of such a high proportion of malnutrition.9,10 The late introduction of solid food and faulty feeding practices including pre-lacteal feeding and inadequate exclusive breast feeding were also suggested as being associated with the persistence of malnutrition over the years.11–13
With this in mind, an analysis of three states in the eastern part of India was undertaken, district by district, to correlate different socioeconomic conditions with the prevalence of underweight children, a commonly used parameter for malnutrition.
Methods
Data were retrieved from the National Family Health Survey (NFHS) 4 (2015–2016). 7 NFHS collected data for the most recent births in the five years before survey. Three states from east India, namely Bihar, Jharkhand and West Bengal (WB), were evaluated. These three states are neighbours, though there are differences in certain demographic features. For example, the female literacy rate in Bihar, WB and Jharkhand are 49.6%, 70.9% and 59%, respectively. A total of 81 districts were taken for ecological analysis from these states. Among different demographic factors, female literacy, households with improved sanitation and children getting adequate diet were evaluated. Other factors known to have an effect on childhood malnutrition regarding childbirth, such as four antenatal check-ups (ANC), institutional deliveries (ID), full immunisation, breast feeding within 1 h of birth and exclusive breast feeding (EBF) were assessed in terms of good practice. All these factors, or absence of them, were examined for a possible association with the prevalence of underweight children.
To assess literacy, the respondent was asked to read from a card in her own language, carried by the interviewer. 14 Improved sanitation is indicated by a flush to piped sewer system, flush to septic tank, flush to pit latrine, ventilated improved pit (VIP)/biogas latrine, pit latrine with slab, twin pit/composting toilet, which is not shared with any other household. These details could be accessed from methodology for NFHS 4. Full immunisation refers to BCG, measles and three doses each of polio and DPT. Early breastfeeding was assessed by asking about children aged <3 years. EBF was assessed by asking about the youngest child living with the mother. Adequate diet refers to breastfed children receiving ≥4 food groups and a minimum meal frequency, non-breastfed children receiving ≥3 Infant and Young Child Feeding (IYCF) practices (other milk or milk products ≥2 times a day, a minimum meal frequency receiving solid or semi-solid food at least twice a day for breastfed infants aged 6–8 months and at least thrice a day for breastfed children aged 9–23 months, and solid or semi-solid foods from at least four food groups not including the milk or milk products food group).
Association was measured between malnutrition and different demographic variables and health-seeking behaviour by the Pearson correlation coefficient. Multivariate linear regression was used for finding predictors for underweight children. Multi-collinearity was assessed using Variance Inflation Factor. SPSS for Windows software (Version 19.0; SPSS Inc., Chicago, IL, USA) was used.
Results
State level comparison of indicators from NFHS 4 from east Indian states.

ANC, antenatal check-up.
District level indicators from NFHS 4 and its correlation with under-nutrition for three east Indian states.

Range is expressed as minimum and maximum value.
District level factors associated with under-nutrition in three east Indian states.
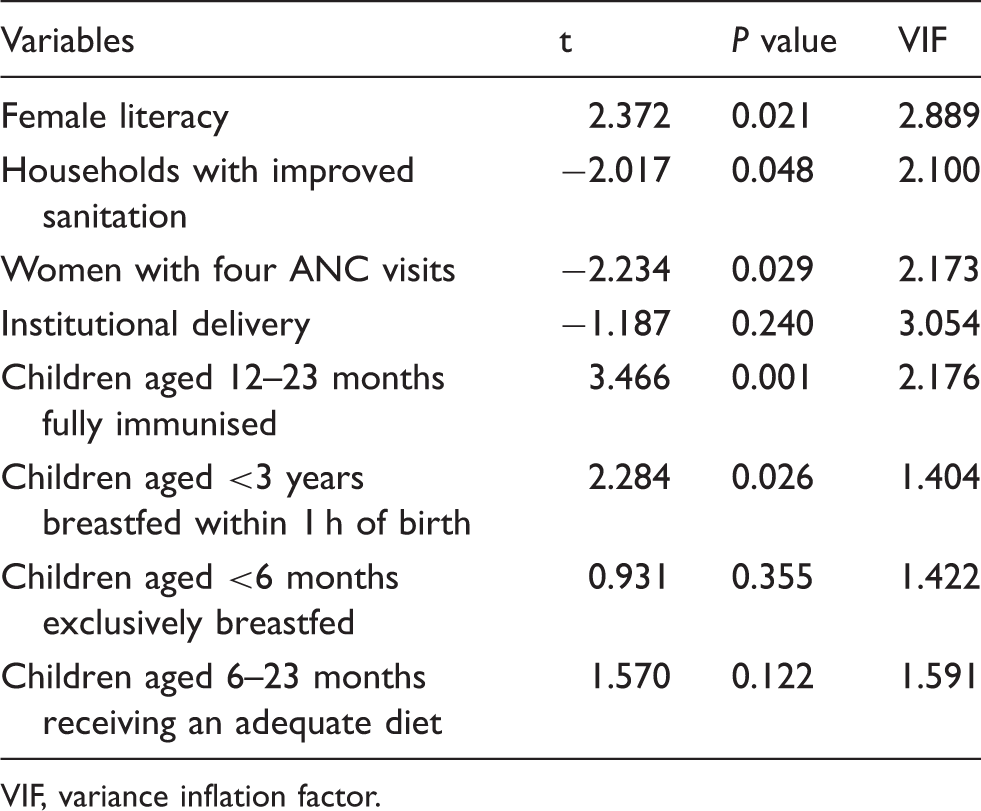
VIF, variance inflation factor.
Discussion
The results suggest that demographic factors and health-related behaviour influence the prevalence of underweight children. The risk of malnutrition decreases with increase in female literacy, as found previously.15–17 Education empowers mothers not only about hygiene and nutrition, but motivates them to seek care when required. 18 Education and independence confer autonomy and paves the way for child nutrition. 19 It also helps them follow dietary advices received from ASHA, ANM or doctors more accurately.
A strong negative relationship was seen between the presence of household sanitation and malnutrition. Sanitation, thus, proves its role for ensuring better nutrition in children.15,20 Lack of improved sanitation, by promoting open defecation, is known to spread water-borne diseases. 15 Exposure to unhygienic conditions leads to environmental enteropathy, leading to malnutrition. 21 In India, improvement in sanitation after the introduction of Swachh Bharat Abhiyan, a nation-wide drive for promoting cleanliness with focus on abolishing open defecation, is expected to lift the nutritional status of our children in the long run. For yielding optimal results, we need to keep up emphasis on generating mass awareness and maintaining momentum.
Maternal use of ANC services has been documented to reduce malnutrition elsewhere. 22 The quality of ANC also plays a vital role in determining long-term outcome. Micronutrient supplementation and a longer association with a health facility during the last ANC visit ensure better outcome of delivery and subsequent nutritional status of children. 23 Institutional delivery probably reflects general poverty.
Full immunisation protects children from some deadly diseases including measles, implicated as one of the greatest killers of children, particularly when malnutrition is present. Breastfeeding within 1 h makes it likely that the newborn child will continue the same for at least the next six months. The timing of initiation of breastfeeding is considered as a strong predictor for malnutrition. 15 An early start is also important for preventing any prelacteal feeding. The benefits of breastfeeding, particularly by prevention of infections and enhanced bonding, still need to be conveyed to the mother. It has been demonstrated that even during infections, breastfed children could maintain their required energy intake. 24 On the other hand, delayed commencement of breast feeding has been identified as an area requiring intervention for improving nutritional status in children. 25
Adequate diet obviously has a direct effect on reducing malnutrition. Previous research claimed that inadequate breast feeding was responsible for malnutrition.19,26 Even when a child gets breast milk, the timely initiation of complementary feeding and gradual increase in its amount is required for optimal growth. The importance of the family pot as the source of diet has been pointed out repeatedly. 27
EBF does not have any effect on underweight children, as is evident from the study. This is in sharp contradiction to previous finding. 28 In fact, EBF followed by complementary feeding (CF) paves the way for better nutrition. Since the problem of bottle feeding is widely prevalent in the country even today, there is need to put focus on both EBF and CF. A recent study found the problem to the extent of 68%. 29 In absence of timely complementary feed, the benefit of EBF could be washed away. Findings from the present study might be a reflection of that particular fact.
In this context, it may be mentioned that Anganwadi workers, a dedicated group of personnel under the Ministry of Women and Child Development, involved in providing complementary nutrition of mothers and children, help Accredited Social Health Activist and Auxillary Nurse Midwives, two cadres of front-line health workers, to ensure maternal and child health nutrition and provide supplementary feeding. Their integration plays a crucial role in deciding the health status of children, particularly at the early ages. Considering the magnitude of the burden of malnutrition on child health in India, all three cadres of workers should cooperate.
The study suffers from certain limitations. The lack of a temporal relationship, being an ecological study and the absence of any socioeconomic condition are major ones. Though improved sanitation was taken into account, it is not a replacement for economic status. On the other hand, inclusion of representatives from 228 million populations from eastern part of India is the greatest strength of the present study. Most studies on malnutrition are limited to a specific study site.
In conclusion, the study points to the influence of some socioeconomic variables on nutritional status. To tackle the problem of malnutrition, Nutrition Rehabilitation Centres are arising across the country. However, we need to focus on preventive aspects. Developing mass awareness about perinatal care behaviour, improved sanitation and breastfeeding is one of them. Care should start at the very beginning of a pregnancy. Primary prevention will bring long-lasting success, particularly in the context of an impoverished population. Furthermore, a participatory approach would inculcate confidence. Future research should highlight the long-term effect of empowering society on childhood nutrition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.