
Abstract
Cirrhotic patients with ascites are at high risk of developing spontaneous bacterial peritonitis (SBP). After exclusion of patients with acute kidney injury (AKI) or other infections, urinary neutrophil gelatinase-associated lipocalin (NGAL) levels were compared between two matched groups of Egyptian cirrhotic patients with ascites, mostly secondary to hepatitis C infection (98%). Group 1 had SBP (n = 41) and group 2 did not (n = 45). By univariate analysis, urinary-NGAL, high total bilirubin, serum creatinine, international normalised ratio and the Model of End-Stage Liver Disease (MELD) score and low platelet count were all significantly correlated with the presence of SBP, but only urinary-NGAL could independently predict development of SBP (P = 0.001). Urinary-NGAL at a cut-off value of 1225 pg/mL, showed a sensitivity of 95% and a specificity of 76%, and is therefore a most useful tool.
Introduction
In hospitalised patients, the prevalence of spontaneous bacterial peritonitis (SBP) in patients with ascites from end-stage liver disease is in the range of 10–30%.1–3 It is considered one of the leading cause of death in this category of patients, with mortality rates of 20–40%.4,5 According to the standard available guidelines,6,7 SBP is diagnosed if the ascitic neutrophil count (ANC) ≥ 250/mm3 after exclusion of any finding suggestive of secondary peritonitis, regardless of ascitic fluid culture. A non-invasive test is therefore needed to diagnose SBP easily and efficiently in an outpatient setting for those asymptomatic patients with cirrhotic ascites, as SBP may be found in at least 3.5% in this patient group. 8
Lipocalins are a group of > 20 binding proteins attaching to different molecules, such as retinoids, arachidonic acid, prostaglandins, fatty acids, steroids and iron. 9 A prominent member of this group is neutrophil gelatinase-associated lipocalin (NGAL, also known as lipocalin-2) which, since its first isolation in 1992, 10 attained great attention as a bacteriostatic agent by depleting intracellular iron stores. 11 It represents an important component of the innate immunity to bacterial infections, as shown in NGAL-deficient mice which developed Gram-negative bacterial infection more significantly than non-deficient mice. 12
Increased NGAL levels in plasma and ascitic fluid have showed significant correlation with SBP, but still requires an invasive sampling technique. 13 Urinary-NGAL measurement is, however, simple and non-invasive. Although its level increases with AKI and urinary tract infections (UTI),14–16 the aim of our study was to correlate urinary-NGAL levels with predicting SBP.
Methods
Our study was prospectively designed with two groups, matched for age and sex, of consecutive adult patients admitted at the National Liver Institute Hospital, Menofia University, between March and December 2016 with ascites secondary to liver cirrhosis and portal hypertension. Group 1, the SBP group, included those diagnosed by a paracentesis sample of ANC ≥ 250 cells/mm3 and group 2, the non-SBP group, those admitted for any other reason rather than SBP, with ANC ≤ 250 cells/mm3. The study was approved from the ethical committee of our University.
In both groups, we excluded patients with any grade of renal impairment, those with any source of infection including not only UTI, but pulmonary infection, enteritis or skin infection, and those having taken recent antibiotics. We also excluded those patients with evidence of malignancy, secondary peritonitis or haemorrhagic ascites.
The diagnosis of liver cirrhosis was based on a combination of physical examination, laboratory and ultrasound findings. The Child-Pugh and the widely used MELD scores were used to assess the severity of every patient’s liver disease.
Urine samples were collected from all patients of the two groups, on the same day as the paracentesis samples, and the urinary NGAL levels were determined using a commercially available ELISA (Antibody Shop, Gentofte, Denmark). The limit of detection for this assay is in the range of 500–4000 pg/mL.
The two groups were statistically analysed using SPSS version 22 for windows. P values were considered statistically significant if < 0.05. For continuously distributed variables, independent samples Fisher’s t-test was used to examine the difference between the two groups, while χ 2 test was used for categorical variables. Significant factors were tested in a univariate binary logistic regression analysis and then only significant variables were entered in a stepwise multivariate logistic regression analysis to identify the independent predictors for the occurrence of SBP. Receiver operating characteristic (ROC) curves were calculated to determine the sensitivity and specificity of independent predictors.
Results
Patients’ demographics and characteristics with statistically significant differences between the two groups.
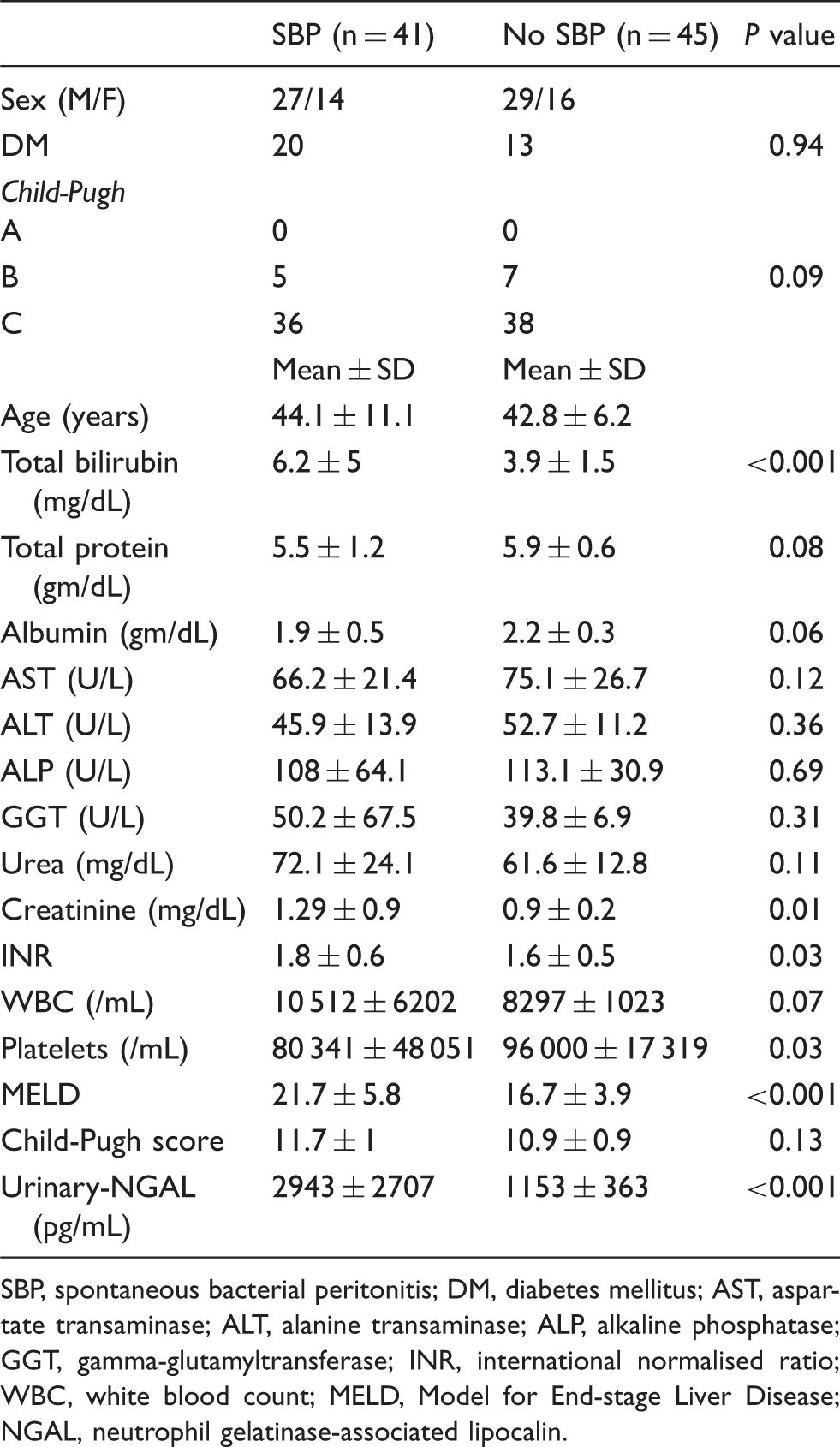
SBP, spontaneous bacterial peritonitis; DM, diabetes mellitus; AST, aspartate transaminase; ALT, alanine transaminase; ALP, alkaline phosphatase; GGT, gamma-glutamyltransferase; INR, international normalised ratio; WBC, white blood count; MELD, Model for End-stage Liver Disease; NGAL, neutrophil gelatinase-associated lipocalin.
By univariate analysis, six variables showed a significant statistical difference between the two groups. High serum total bilirubin, creatinine, international normalised ratio, MELD score and urinary-NGAL, beside low platelet count, were all associated with the development of SBP (P < 0.001, 0.01, 0.03, <0.001, <0.001 and 0.03, respectively). On the other hand, variables such as the presence or absence of diabetes mellitus, serum total protein, albumin, aspartate transaminase, alanine transaminase, alkaline phosphatase, gamma-glutamyl transferase, urea, white blood cell count and Child-Pugh score had no statistically significant difference. Table 1 also shows the statistical differences of the different variables between patients of the two groups.
Logistic regression analysis displaying independent predictors of the occurrence of SBP.
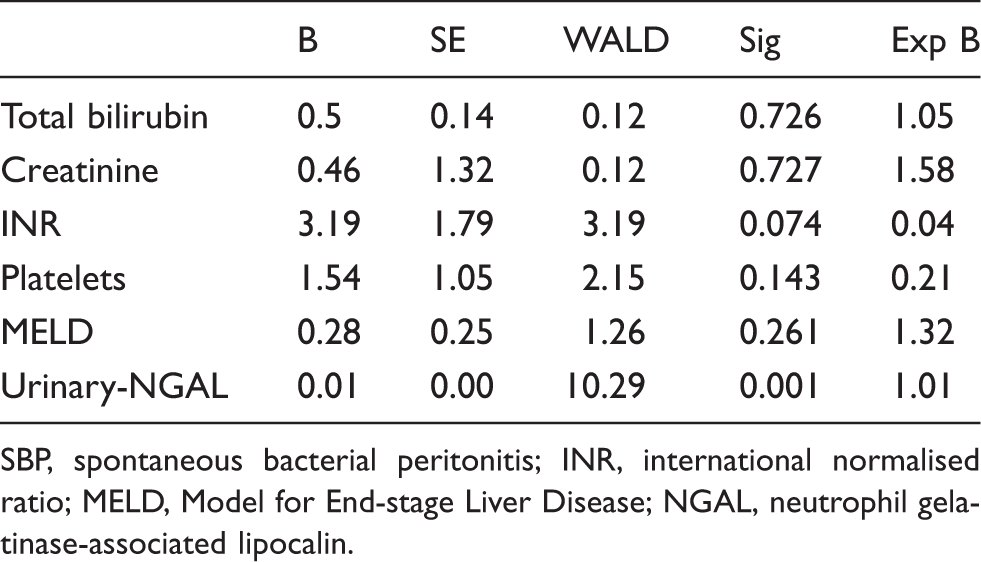
SBP, spontaneous bacterial peritonitis; INR, international normalised ratio; MELD, Model for End-stage Liver Disease; NGAL, neutrophil gelatinase-associated lipocalin.
By the ROC analysis, our results showed that urinary-NGAL significantly differentiates between patients of the two groups at cut-off points of ≥1225 pg/mL (sensitivity 95%; specificity 76%).
Although we excluded patients with any grade of renal impairment, we noticed later during our follow-up the development of a degree of renal impairment in some of those with urinary-NGAL levels >1225 pg/mL (8/39 patients in group 1 [20.5%] and 3/11 patients in group 2 [27.3%]).
Discussion
SBP in cirrhotic patients increases their morbidity and mortality with significant healthcare costs. Its high prevalence in asymptomatic patients explains the need for a non-invasive test as its diagnosis as early treatment is beneficial. Different variables were assessed before to find predictors for SBP and good correlation was shown with low platelet count,17,18 impaired prothrombin time, 19 increase serum creatinine, 19 beside worsening of liver disease scores such as Child-Pugh 18 and MELD. 20
NGAL is known to be elevated with bacterial infection and is a promising biomarker. 21 Although elevated plasma and peritoneal fluid NGAL may efficiently diagnose SBP,22,23 an invasive procedure is still required. Urinary-NGAL has not received enough attention in the diagnosis of SBP to date, as it was considered solely as an early predictor of AKI and UTI. Our univariate analysis results showed a highly significant correlation between the development of SBP and the level of urinary-NGAL, beside indices of liver failure. By multivariate analysis, only urinary-NGAL could independently predict SBP with a very high sensitivity and specificity at a cut-off value of 1225 pg/mL.
Although we did not test the urinary-NGAL in asymptomatic cirrhotic patients with ascites, we suggest that a urinary-NGAL level >1225 pg/mL could be used as a non-invasive outpatient or bedside test for any patient with suspected SBP or even as part of routine examination for asymptomatic patients with cirrhotic ascites. Diagnostic paracentesis and other laboratory tests could be limited for those patients needing more intense evaluation.
A major limitation of our study is the well-known relation between SBP and the development of renal impairment. 14 Although we excluded patients with any degree of renal impairment, a high urinary-NGAL level might still be an early predictor of AKI.15,16 Indeed, we found 20.5% and 27.3% of groups 1 and 2, respectively, developed some degree of renal impairment during their admission. However, owing to our high cut-off, a high sensitivity (95%), it remains a highly productive test if used for screening for SBP.
Our results also showed that liver cell failure parameters and scoring systems were not able to predict SBP independently, but urinary-NGAL could. Further work is needed to validate our results in asymptomatic patients with cirrhotic ascites.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.