
Abstract
Drug-resistant tuberculosis (TB) is emerging as a new and serious public health challenge. We present the first case with confirmed extensive drug-resistant TB in Tanzania in a patient who had prior exposure to anti-TB drugs and a history of imprisonment in South Africa. The addition of bedaquiline to the treatment regime resulted in positive to negative sputum conversion. After a total of 30 months on treatment he was declared cured, remaining clinically stable and culture-negative throughout the follow-up. Close monitoring is important in managing drug-resistant TB cases, and good surveillance is required to detect drug-resistant TB to prevent further transmission.
Introduction
Extensively drug-resistant tuberculosis (XDR-TB) is defined as TB resistant to any fluoroquinolone, and at least one of the three second-line injectable drugs (capreomycin, kanamycin and amikacin), in addition to multidrug resistance. 1 The disease has recently become a matter of public health importance as the prevalence continues to rise despite raised awareness and preventive measures put in place. In 2017, the World Health Organization (WHO) reported 160,684 cases of multi-drug resistant/rifampicin-resistant tuberculosis (MDR/RR-TB) notified in 2017, among whom an estimated 8.5% had XDR-TB. 1
Tanzania is one of 30 high-burden TB countries globally with a documented increasing trend of detected drug-resistant TB cases. 1 In 2017, its incidence was estimated at 29 per million population. 2 It accounts for 0.9% of all new TB patients seen and 4.7% of previously treated TB cases; among notified pulmonary TB patients in 2017, some 640 have been duly recorded. 1
The treatment for drug-resistant TB is very complicated and expensive, and requires a prolonged duration of treatment, which has higher rates of toxicity. 2 Following WHO approval of bedaquiline, Tanzania started its use in 2015. We report the first XDR-TB patient and describe both his management approach and outcome.
Case report
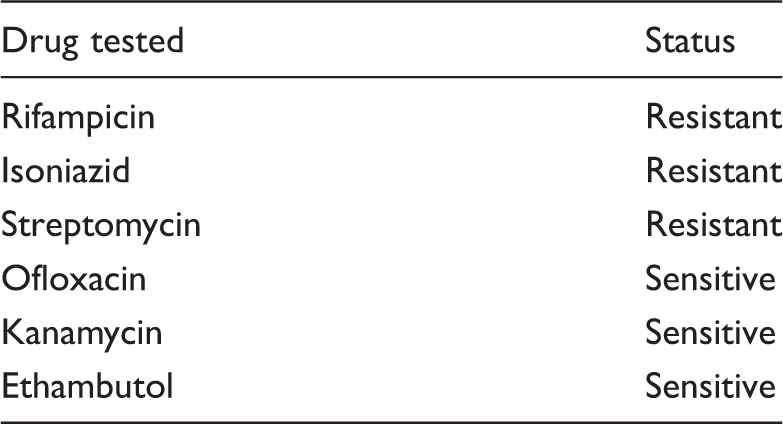
Drug susceptibility results at the time of MDR-TB diagnosis.
Drug susceptibility results during MDR-TB follow-up at month 8.

Our patient was started in October 2014 on capreomycin 1G once daily (o.d. × 5/week), levofloxacin-1G, isoniazid 600 mg, clofazimine 300 mg, cycloserine 500 mg, pyrazinamide 1.5 G, para-aminosalicylic acid (PAS) 8 G and vitamin B6 200 mg once daily. This treatment was a salvage plan while waiting for bedaquiline and linezolid to be introduced once available.
The chest radiograph at this stage showed increased hilar opacification. Despite radiological improvement, he remained smear positive after one month. However, the next month, he reverted to being culture-negative; in the subsequent month, as well as three and six months later, cultures were again positive. Unfortunately, cultures for other months were not available.
In November 2015, bedaquiline at 400 mg o.d. was eventually introduced for two weeks and subsequently at 200 mg o.d. (×3/week) for 22 weeks, as well as linezolid 600 mg, ethambutol 1.2 G, levofloxacin 1 G, PAS 8 G and amoxicillin-clavulanic acid 2.6 G daily for 18 months.
Culture became negative one month following the introduction of this new medication and remained so till the end of the treatment period, except for one result in March 2016 which was later disregarded as it was presumed to be a laboratory error due to contamination. The chest radiograph at one year of treatment showed signs of healing with an increase in fibrotic changes especially in the left upper lung.
He completed treatment in July 2017, thus having undergone 30 months of medications (12 months on a salvage regime plus 18 months on the strengthened regime with bedaquiline and linezolid, both having been given for six months).
He was declared cured as >11 sputum cultures were negative over the final 18 months. He did not develop any severe adverse drug reaction, despite close monitoring. He remained stable, progressing normally with his daily activities. Monthly follow-up for two years confirmed his weight as remaining stable and all cultures negative.
A written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review from the Editor-in-Chief of this journal.
Discussion
In this report, we document the first case of XDR-TB in Tanzania. The patient had interrupted treatment, a documented risk for developing drug resistance. South Africa, where he was incarcerated, has a higher burden of MDR-/XDR-TB than Tanzania. 4 His first drug sensitivity test was sensitive to fluoroquinolones and second-line injectables which makes the possibility of initial infection with a drug-resistant TB strain unlikely. However, he had a history of poor adherence to treatment and therefore was susceptible of acquiring drug-resistant TB.
Ours is the first patient to use bedaquiline in Tanzania. The case report highlights some of the challenges of managing MDR-TB and the very costly long duration of treatment necessary. Fortunately, there were no severe adverse events which could have further complicated his management.
Addition of bedaquiline and linezolid after 12 months of initial salvage regimen led to quick sputum conversion in our patient. A similar experience was had in Singapore. 5 Bedaquiline appears to be associated with more rapid sputum conversion and higher cure rates than many other medications for drug-resistant TB. Similarly, good treatment outcomes were achieved in Kyrgyzstan and Mali. 6
Treatment for XDR-TB is often, however, associated with poor outcomes including treatment failure and mortality, worse than with MDR-TB.7,8 It seems that later generation quinolones improve treatment outcomes, even in those with resistance to quinolones.9,10
Nutritional support was given to our patient throughout his treatment; this may improve chances of treatment success by 50%.11,12 As has been shown to improve the odds of treatment success by 69% in one meta-analysis, 13 directly observed therapy was the approach used in the management of our patient.
The major concern with drug-resistant TB treatment is adverse drug reactions, usually resulting in at least one adverse event. 14
Footnotes
Acknowledgements
The authors thank all the people who were involved in the management of this patient in one way or another; their recommendable contributions are sincerely appreciated. In particular, the team thank Vishnu Mahamba, Willy Mbawala, Tristan Bayly and Inge Kopperlaar for their endless support in writing this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.