
Abstract
This study aimed to determine the utility of coeliac serology for monitoring dietary adherence in coeliac disease. Serum anti-tTg IgA and anti-DGP IgG levels of 42 newly diagnosed patients were measured at diagnosis and at intervals of three, six and 12 months after starting a gluten-free diet. Both anti-tTg and anti-DGP antibodies decreased in all patients. The decline in the former was significantly greater at 3–12 months throughout, while in the latter the decline was seen only at three months but not subsequently. Serial measurement of coeliac serology may help in monitoring adherence to a gluten-free diet.
Introduction
Coeliac disease (CD), also known as coeliac sprue or gluten-sensitive enteropathy, is an auto-immune gastro-enteropathy, triggered by the ingestion of gluten present in wheat, barley and rye in genetically susceptible individuals. In the last two decades, CD has been increasingly reported from various countries, including India.1–4
The immunological sequel of CD starts with the intake of gluten and a predisposing genetic makeup of HLA molecules of class II DQ2 or DQ8.4–7 Tissue transglutaminase (tTg) enzyme causes deamidation of glutamic acid residues of gliadin molecules which are then recognised by specific intestinal T cells leading to damage of enterocytes with flattening of intestinal villi and consequent malabsorption.8–10
At present, a lifelong gluten-free diet (GFD) is the only recommended option available for CD. Dietary adherence is essential for symptomatic improvement, proper growth and preventing long-term complications such as osteoporosis and malignancy.11,12 Non-compliance is a major problem, especially in children and adolescents. 13 The reported adherence is in the range of 32–95%.14–17
Various methods exist to assess dietary adherence, but these remain controversial and challenging for clinicians.18,19 Dietary assessment by a skilled dietician and demonstration of normalisation of histological changes are considered the gold standard for monitoring dietary adherence. However, such skilled personnel are not readily available and simple clinical assessment lacks the sensitivity and predictive value for detecting partial adherence.20,21
Recently, anti-tTg and anti-DGP antibody level monitoring has emerged as a tool for assessing such adherence. Several studies have reported rises in coeliac-specific antibodies where patients, after starting a GFD, have reverted to gluten. However, there are conflicting reports about the reliability of such measurements in both adult and paediatric populations.22–25
With this background, we evaluated the utility of anti-tTg IgA and anti-DGP IgG antibodies to monitor the first year of dietary adherence in children with CD having committed to a GFD.
Methods
All patients (aged <18 years) who came to our paediatric gastroenterology clinic with clinical manifestations of CD and positive celiac serology between November 2014 and March 2016 underwent upper gastrointestinal endoscopic duodenal biopsy. Any gross abnormality such as mucosal erythema, and scalloping or blunting of villi, were noted. The diagnosis of CD was made on the basis of the modified European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) criteria, 26 i.e. suggestive clinical manifestations, a positive serological test and suggestive histology.
Patients diagnosed with CD, who had never previously received a GFD, were enrolled in this prospective observational study, after informed and written consent was obtained from their parents.
Demographic data, clinical features, anthropometry and examination findings including age, gender, duration and types of symptoms (abdominal pain, diarrhoea, vomiting, constipation, lethargy) as well as height, weight and pallor were recorded on a pre-structured proforma. Patients were followed for one year (monthly for the first three months and quarterly thereafter) at our clinic. Serological tests were performed on the day of endoscopy and again at three months (±7 days), six months (±7 days) and one year (±7 days) of starting a GFD.
Kits used for tests were: (1) tTg IgA ELISA Kit ref. 7044 (reference cut-off: negative if < 8 IU, equivocal if 8–12 IU and positive if > 12 IU); and (2) DGP IgG ELISA EIA-5080 (reference cut-off: negative if < 15 IU, equivocal if 15–30 IU and positive if > 30 IU).
At each visit, all patients were independently assessed by a skilled dietician for GFD transgressions and evaluated by senior consultant for clinical improvement. All patients were counselled regarding their dietary adherence and its importance during follow-up after assessment.
Dietary assessment by the dietician included assessment by a pre-structured questionnaire consisting of a list of both gluten-free and gluten-containing items. Parents were asked to itemise the frequency of gluten intake classified as none, occasional (items 1–2 times/month) or gross (items >2 times/month).
Improvement in symptoms (decrease in frequency of stools, weight and height gain, and lessening in pallor) were recorded at each follow-up visit. At the end of the follow-up period, patients were classified as on the basis of both dietary assessment and clinical evaluation as either adherent, having no dietary transgression and clinical improvement, or non-adherent (gross or occasional) with or without clinical improvement.
Data were entered on an Excel spreadsheet and analysed for the mean anti-tTG IgA and anti-DGP IgG antibody levels and the mean decline in values from baseline and at three, six and 12 months was compared using Student’s t-test. Receiver operating characteristic (ROC) curves were drawn for anti-TG IgA and anti-DGP IgG antibodies to determine the level which indicated non-adherence.
Results
Among 58 children (26 boys; age range = 2–15 years) enrolled, chronic diarrhoea was the most common presenting complaint (84.5%) followed by growth failure (77.5%), abdominal pain (67.2%) and abdominal distension (62%). Atypical presentations of CD, such as poor weight gain and anaemia without any gastrointestinal manifestations, were seen in five children (8.6%). Two had silent CD (3.4%), diagnosed as a part of a screening programme. A total of 22 (37.9%) were wasted and seven (12%) were severely so (Z score <−3 SD); 43 (74%) were stunted at the time of diagnosis (28, 48.2%, severely so). Some 42 (72.4%) were anaemic at the time of diagnosis.
Only 42 patients who were followed up regularly and were consistently adherent or non-adherent throughout the year were included in the study. Of these 42 patients, 26 (62%) were adherent (group A) and 16 (38%) were not (group N).
Mean anti-tTg IgA and anti-DGP IgG levels at baseline, three and six months and one year in the two groups.
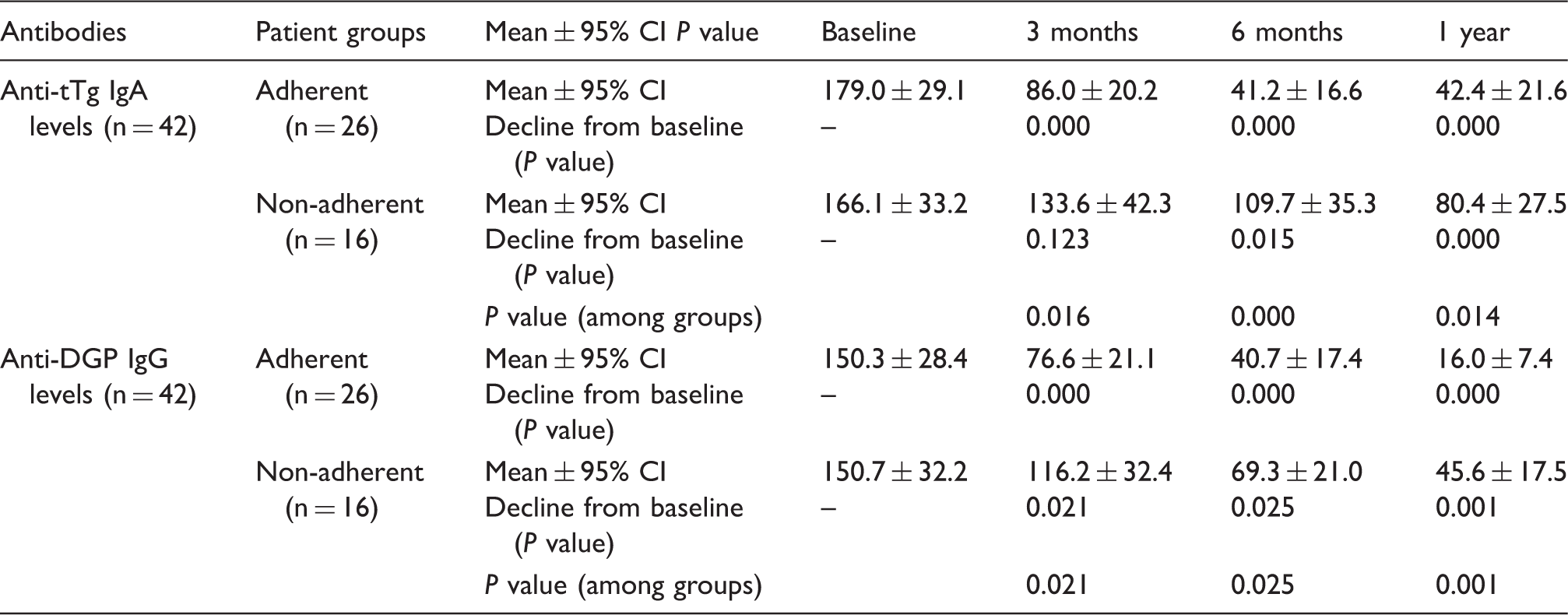
The decline in mean antibody levels with respect to baseline in adherent and non-adherent patients are shown at three and six months and one year, respectively (Table 1). The levels of both antibodies declined significantly in both groups. However, the mean decline of anti-tTg IgA levels was significantly more in adherent patients compared to non-adherent patients (P = 0.008, 0.000 and 0.020) at three, six and 12 months, respectively, while the decline in mean anti-DGP IgG levels was significantly more in adherent patients only at three months (P = 0.008), but not later (P = 0.122 and 0.120). The decline of antibody levels (Fig. 1) show that at one year of starting a GFD, the gap between adherent and non-adherent patients for anti-tTg IgA is wider compared with anti-DGP IgG levels.
Decline in mean anti-tTg IgA and anti-DGP IgG levels in the two groups during the first year of follow-up.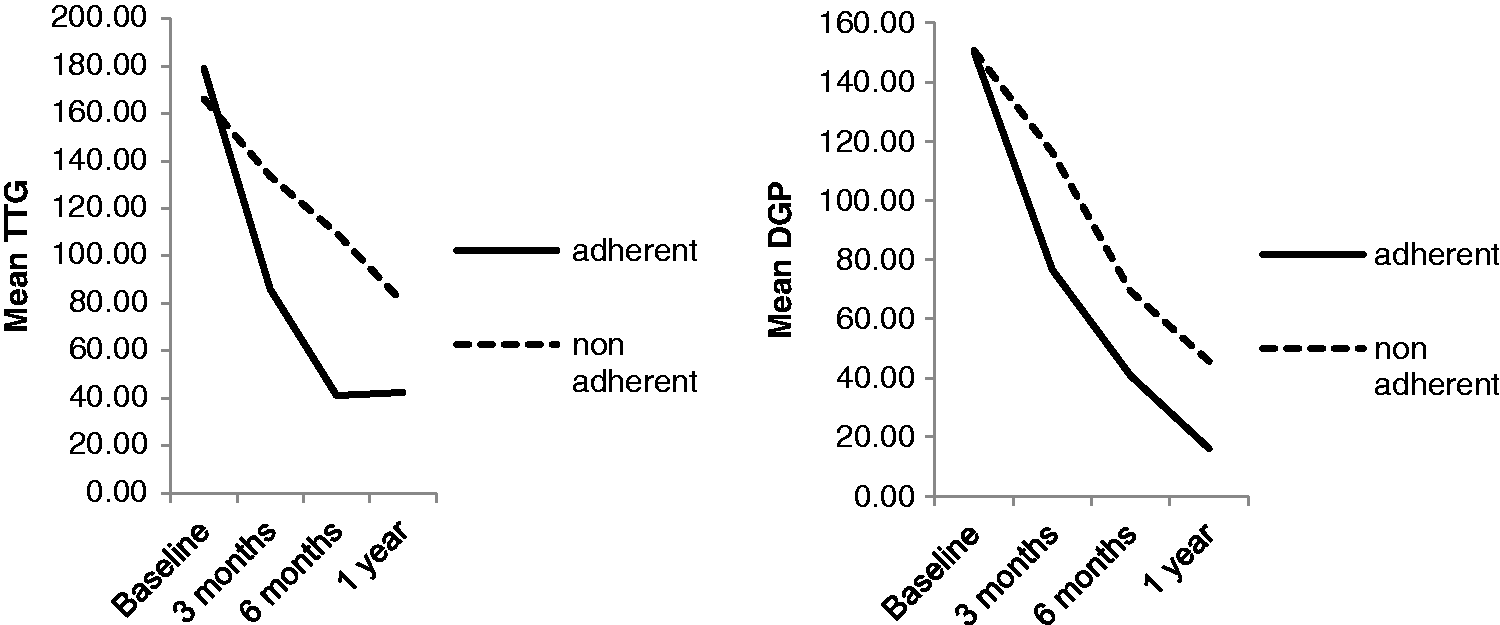
Compliance cut-off values, calculated from the ROC curve, are 90.3, 57.9 and 48.1 for anti-tTg IgA 81.8, 45.5 and 21.5 and anti-DGP IgG at three, six and 12 months, respectively. After one year, in 69% and 77% of adherent patients, respectively, anti-tTg IgA levels and anti-DGP IgG were found below compliance cut-off values. Normalisation was seen in 38–73% of adherent patients at the end of one year, according to the diagnostic cut-off levels. The sensitivity of compliance cut-off values of both tests to detect non-adherence was in the range of 68–75% at one year.
Discussion
A lifelong GFD is the only treatment available for CD; hence, monitoring of dietary adherence is vital for its management. Our study explores the long-term dynamics of CD-related serological tests after starting a GFD and the performance of these tests in monitoring dietary adherence in children with CD.
Our results showed that after starting a GFD, mean anti-tTg IgA levels decreased with time in all patients. However, this decline was inversely correlated to the degree of dietary adherence. Among adherent patients, it was significantly steeper than in non-adherent patients, as reported earlier.22,23 Higher levels of anti-tTg IgA in non-compliant or partially compliant adult patients24,25 have been reported
As already shown, serum levels of anti-DGP IgG were likewise higher in non-adherent patients compared to adherent patients, 25 but we demonstrated that this decline remained higher in adherent patients only at three months but not later, because anti-DGP IgG levels did not correlate well with the degree of adherence later in the year, as also previously attested. 23
To see if the level of antibodies could correctly categorise children as either adherent and non-adherent, by calculating the compliance cut-off for anti-tTg IgA and anti-DGP IgG from the ROC curve, we were able to show an adequate sensitivity and specificity for both antibodies. However, patients who have lower levels of anti-tTg IgA levels at the time of diagnosis (but above the diagnostic cut-off) will show a decline, but compliance cut-off values will not be able to categorise them correctly. Therefore, the use of compliance cut-off values is unreliable in clinical practice to assess dietary adherence. Instead, the change in serial antibody levels in individual patients is much more reliable for follow-up and monitoring.
Conclusions
Our findings support the significant impact of dietary adherence on CD-related serological antibody levels during follow-up. The persistence of higher levels of antibodies can help in identifying the patients with dietary transgressions. Both types of antibodies decreased after starting a GFD but anti-tTg IgA levels correlated well with dietary adherence throughout the year while anti-DGP IgG did not. Testing antibody levels serially is therefore a much better indicator of dietary adherence rather than measuring a compliance cut-off value at any single point of time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.