
Abstract
Babies with ABO incompatibility are often advised frequent biochemical screening and prolonged hospital stay. Our primary objective of the study was to compare serum bilirubin levels at 48 h and 96 h of age in neonates with and without ABO incompatibility. Our prospective study included neonates with gestation ≥ 34 weeks, with or without ABO incompatibility (92 in each group). A direct Coombs test was performed on cord blood. The mean serum bilirubin and haematocrit levels in both groups at 48 h and 96 h were comparable. The mean reticulocyte count of babies with ABO incompatibility was, however, significantly higher. Late preterm and term neonates with and without ABO incompatibility have similar bilirubin levels and no increased risk of significant hyperbilirubinemia. Prolonged hospitalisation of these neonates appears to be unnecessary.
Introduction
Neonatal hyperbilirubinemia is the most common clinical condition requiring evaluation and treatment in neonates and is a frequent cause for readmission during the first postnatal week of life. ABO haemolytic disease has been recognised as a major risk factor.1,2 Although this occurs in 20–25% of pregnancies, only a small fraction of these babies require intervention, namely those with ABO haemolysis. 3
ABO incompatibility can present with a spectrum of completely asymptomatic disease to severe haemolysis. 4 Certain factors have been implicated in increasing the risk of hyperbilirubinemia: a positive direct Coombs test (DCT) being one, though with conflicting evidence.5,6 The American Academy of Pediatrics (AAP) recommends thorough clinical assessment and preferably a biochemical screening of all newborns for jaundice before discharge, especially if they are discharged before the age of 72–96 h. Furthermore, in babies with ABO incompatibility, AAP advises cord blood sampling for blood group typing and DCT before discharge. 7 The National Neonatology Forum (NNF) stresses a complete clinical assessment and, if feasible, biochemical testing for jaundice before discharge of all newborns. 8 In neonates with ABO incompatibility, adherence to these guidelines is even more strongly encouraged. However, in low-resource settings, this advice may not be appropriate.
In India, the government is making tremendous efforts in encouraging institutional deliveries through programmes such as Janani Suraksha Yojana (JSY). 9 The India Newborn Action Plan (INAP) aims to bring down neonatal mortality to single digits by 2030. 10 Implementation of these programmes will lead to increased bed occupancy in hospitals. Steps therefore need to be taken to reduce the burden on the health system without jeopardising neonatal health. Making mother–baby dyads with ABO incompatibility stay in hospital for a longer period and perform biochemical screening and frequent follow-up not only adds to the burden on the health system but also increases the cost of hospitalisation, putting extra pressure on hospital laboratories as well as added expenses for the parents. We therefore conducted this study to see if these babies are actually in need of intensive monitoring.
Participants and methods
Our prospective study was conducted in the Division of Neonatology, Department of Pediatrics of a tertiary care teaching hospital from April 2014 to March 2015. We compared mean serum bilirubin levels between neonates with and without ABO incompatibility in the early neonatal period. The primary objective was their comparison at the ages of 48 h and 96 h; the secondary objectives were to compare haematocrit, Coombs positivity, reticulocyte count, peripheral smear findings, number of babies requiring phototherapy and exchange transfusion.
Neonates with a gestation ≥34 weeks, born to mothers with O Rh positive blood group, were enrolled in the study. These babies were divided into two groups. Group1 included babies with blood group A or B and group 2 included babies with blood group O.
Babies with birth asphyxia (Apgar score ≤7), clinical sepsis, respiratory distress with Down’s score >2/10, clinical pallor, shock and bleeding from skin or mucosal membranes, direct hyperbilirubinemia, congenital anomalies and chromosomal disorders were excluded.
Blood group and DCT were performed on the cord blood of babies born to mothers with O Rh positive blood group. Serum bilirubin, haematocrit, peripheral smear examination and reticulocyte count were measured in all babies aged 48 ± 2 h. Serum bilirubin and haematocrit levels were repeated at the age of 96 ± 2 h. Babies were followed up during their hospital stay; serum bilirubin and haematocrit levels were repeated whenever they appeared clinically jaundiced. These babies were managed either with phototherapy or exchange transfusion according to AAP guidelines. 11
Serum bilirubin levels were measured using a photospectrometric microbilirubinometre. Haematocrit levels were measured in the red blood cell column in the centrifuged capillary. Reticulocyte count was performed using new methylene blue dye. A peripheral smear was prepared using Wright’s stain and was reported by our hospital pathologist.
Using the study by Yaseen et al., in which the mean bilirubin level in term ABO-incompatible neonates aged 96 h was reported as 188 ± 80 µmol/dL, 12 and assuming that babies without ABO incompatibility will have serum bilirubin levels 34 µmol/dL lower, to reach a power of 80% and level of significance 5%, the sample size was calculated to be 77 in each group. Considering attrition of 20% during the study, we determined to have 92 in each group.
Statistical analysis was done using SPSS software version 20.0. A P value <0.05 was considered significant. Unpaired Student’s t-test was used to compare serum bilirubin, haematocrit and reticulocyte count in both the groups.
Results
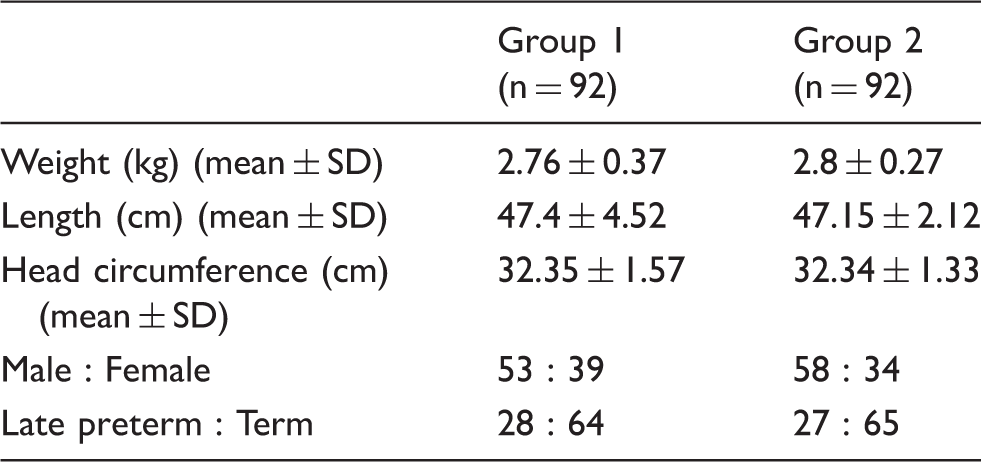
Baseline demographic profile of neonates with and without ABO incompatibility setting.
Serum bilirubin levels at 48 h and 96 h in two groups.
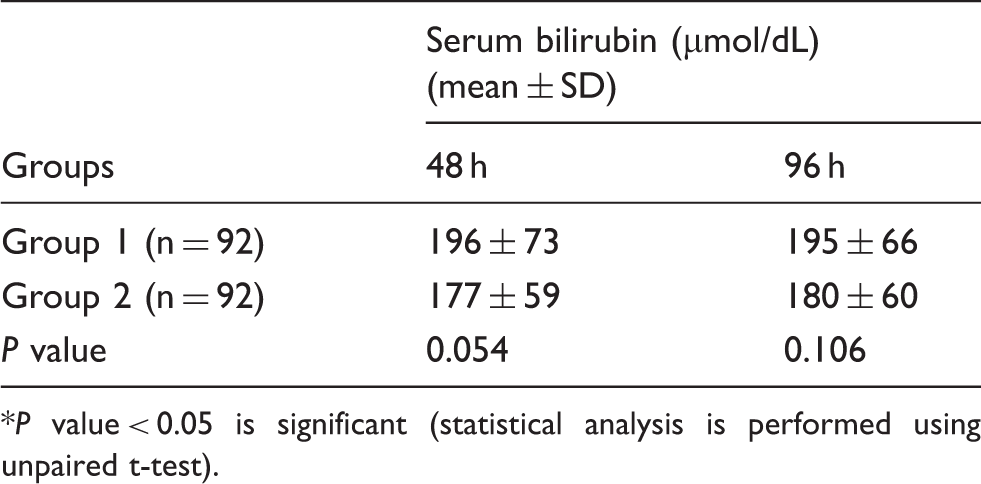
P value < 0.05 is significant (statistical analysis is performed using unpaired t-test).
Haematocrit and reticulocyte count (RC) in two groups.
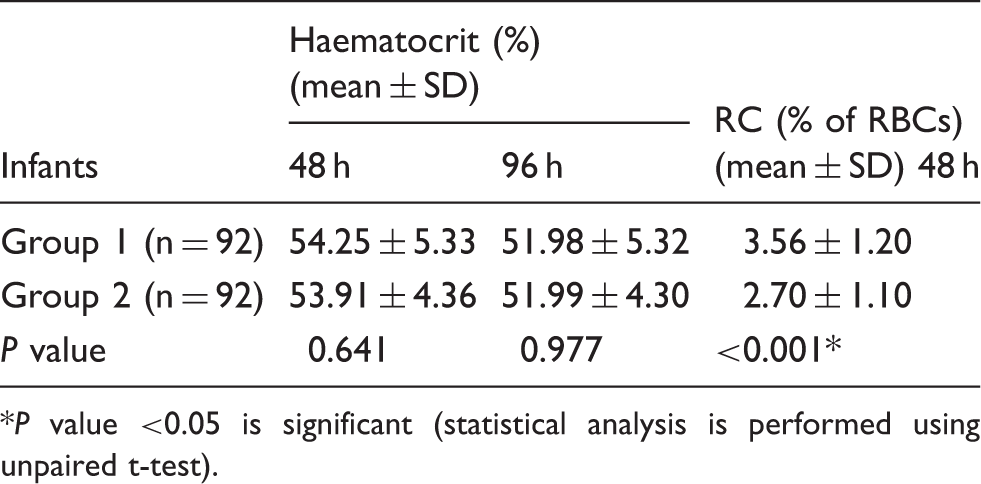
P value <0.05 is significant (statistical analysis is performed using unpaired t-test).
The number of babies who received phototherapy in both the groups did not show significant difference: 22 (23.9%) in group 1 and 16 (17.3%) babies in group 2 (P = 0.275). The mean pre-phototherapy serum bilirubin levels in babies who received phototherapy was also compared in both groups (311 ± 50 µmol/dL with ABO incompatibility and 253 ± 20 µmol/dL without) which was statistically significant. The mean age for starting phototherapy in group 1 was 57.8 ± 17.6 h and in group 2 57.0 ± 19.4 h (P = 0.895).
The DCT was positive in only two babies (0.02%); thus, a comparative statistical analysis of different variables could not be done. Both DCT positive babies underwent exchange transfusion at 48 h and 46 h of life, at serum bilirubin levels of 462 and 376 µmol/dL, respectively.
Discussion
The NNF recommends a thorough clinical assessment and if feasible, biochemical screening of all the neonates before discharge. However, data to support NNF protocols are lacking in India.12,13
We could not find many studies describing the trend of bilirubin levels in babies with ABO incompatibility and any risk factors predicting development of hyperbilirubinemia needing intervention in these babies. Furthermore, no clear guidelines on whether babies with ABO incompatibility should be subjected to a longer postnatal stay in hospital exist. Despite a report from 1996 that babies with ABO incompatibility are at twice the risk of needing intervention in the form of phototherapy compared to normal babies, 14 our results are contrary. Exchange transfusion was rarely needed, an observation similar to ours. 14
In contrast to previous studies, we did not find significant haemolysis, lower haemoglobin levels, lower haematocrit or red blood cell count.15–17 However, significant reticulocytosis was observed in ABO incompatibility as previously reported. 16 This may be explained by subclinical haemolysis, although bilirubin levels did not rise to levels requiring intervention.
Conflicting studies exist on the role of DCT in ABO incompatibility; we cannot really comment on this, although the only two babies whose bilirubin reached levels needing exchange transfusion had positive tests.
Conclusion
In a resource-poor country, the burden of expensive protocols must be weighed by their practicality and usefulness. Although further multicentric studies with larger sample size over wider ranges of population with varying ethnicity are required to modify the guidelines, our study suggest strict adherence to AAP guidelines is unjustified.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.