
Abstract
Libman-Sacks endocarditis (LSE) is one of the most characteristic cardiac lesions in systemic lupus erythematosus (SLE). Patients may remain asymptomatic, while symptomatic patients often suffer with systemic emboli. These commonly test positive for anti-phospholipid antibody (aPA). The association of LSE with an overlap of rheumatoid arthritis (RA) and lupus (also known as ‘rhupus’) is rare. We report such a patient, who had been diagnosed as having RA seven years before and had suffered an acute ischaemic stroke one year previously and had echocardiographic evidence of LSE found during routine evaluation. However, she tested negative for aPA.
Introduction
In Libman-Sacks endocarditis (LSE), the mitral and aortic valves are commonly involved, but any valve as well as endocardial surfaces may be affected. 1 Asymptomatic cases may be discovered at routine echocardiography. Treatment is directed towards the underlying cause, preventing embolism and may require surgery.1,2
Case report
A 34-year-old Bangladeshi woman, diagnosed with rheumatoid arthritis (RA), who had a previous cerebral infarction (Figure 1), was referred for echocardiography. During evaluation at our centre, she had no specific complaints. She was not taking contraceptive medications nor recreational drugs. She had no adverse pregnancy outcomes nor thrombotic episodes; she had no known valvular heart disease or family history of such.
Computed tomography scan of the head showing right cerebral infarction.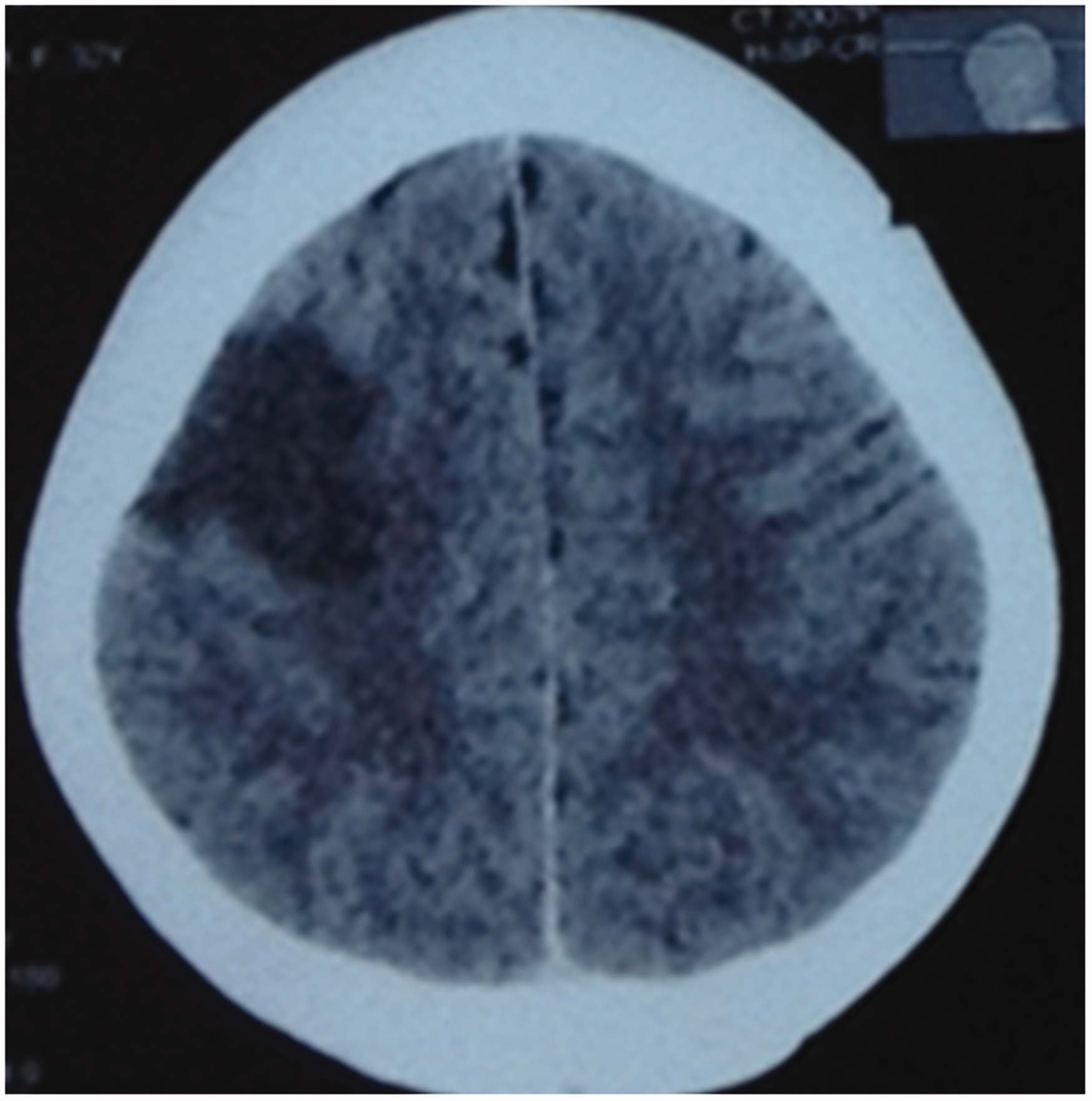
On examination she was pale with evidence of left hemi-paresis. She had grade 3/5 tenderness in all metacarpo-phalangeal and proximal inter-phalangeal joints. Precordial findings were essentially normal.
Investigations revealed a low haemoglobin (Hb = 10.5 g), normal white cell counts and slightly reduced platelet count (130 × 109/L). Erythrocyte sedimentation rate (ESR) was 30 mm/1st h and C-reactive protein (CRP) was 6 mg/L, neither being significant.
Electrocardiography and postero-anterior chest radiography were normal. Transthoracic echocardiogram revealed an intra-cardiac mass in the right ventricle arising from the inter-ventricular septum (Figure 2) without any pedicular structure or valvular involvement. Transoesophageal echocardiogram confirmed the presence of the mass but excluded any shunting (Figure 3). As non-infectious endocarditis was considered, she was evaluated in more detail.
Transthoracic echocardiogram revealed a mass in the right ventricle arising from inter-ventricular septum. Transoesophageal echocardiogram confirmed right ventricular mass.

Relevant test reports of the patient with rhupus.

ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; CCP, cyclic citrullinated peptide; ANA, anti-nuclear antibody.
Thus, a diagnosis of rhupus complicated by LSE that had provoked a previous cerebral infarction with left sided hemi-paresis was made. Treatment included aspirin, hydroxychloroquine and atorvastatin; the patient was regularly followed up.
Discussion
Rhupus is an uncommon clinical condition; some authors consider it as a subset of systemic lupus erythematosus (SLE) while others consider it as an overlap of RA and SLE. Up to 20% of patients with RA may have positive ANA, 17% of SLE patients may have positive RF but only 1.3–2% fulfil the criteria for rhupus.3,4 In most cases, RA precedes the manifestation of SLE by several years, but not always, and simultaneous onset of both RA and SLE may occur; organ involvement in rhupus is less common and less severe than SLE.3,4
Central nervous system (CNS) involvement in rhupus may occur in 7% cases and includes venous sinus thrombosis, CNS vasculitis, thromboembolic stroke and cerebritis.2,4 Thrombosis and emboli are usually associated with positive aPA. Embolic events may result from Libman-Sacks vegetations. 2
Absence of fever and stigmata of infective endocarditis, negative blood cultures, underlying rhupus and the echocardiographic characteristics of a cardiac mass suggested LSE in our case. The exact cause for cerebral infarction in our patient was not determined; this may be result of thrombosis, vasculitis or cardiac embolisation.
Rheumatological diseases evolve over time and every new feature should be taken into account during evaluation and follow-up, as management and prognosis vary with each different diagnosis.3,4 Every patient with connective tissue disease merits cardiac evaluation including echocardiography 5 which may unveil LSE. Measures may then be taken to prevent life-threatening systemic or pulmonary embolism.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Informed written consent was taken from the patient regarding use of her clinical and laboratory data and any accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.