
Abstract
This retrospective cohort study was aimed at evaluating the factors associated with the resumption of sexual intercourse (SI) before the six-week postpartum visit and was carried out between 1 January and 15 February 2014. The main variables studied included maternal age, number of living children, mode of delivery, complications observed at delivery and resumption or not of SI. Data from women who resumed SI were compared to those of women who did not. Fisher’s exact test and t-test were used for comparison. We recruited 120 women, among whom 95 (79.1%) resumed SI. Of these, 65/95 (68.4%) did not attend the postpartum visit while 30 (31.6%) did (P = 0.321). The factors associated with early resumption of SI were maternal age of 20–34 years (P < 0.001), women with one child (P < 0.004) and who had had an uncomplicated vaginal delivery (P < 0.001). Our conclusion is that nursing mothers should receive postpartum contraception before leaving the hospital.
Introduction
Short inter-pregnancy interval is associated with poor maternal, fetal and neonatal health (preterm birth and low birth weight) as well as poor infant health.1,2 A worldwide increase in postponing, spacing and limiting pregnancies is the most important single factor for significantly reducing the mortality of mothers. 3 Concerning women with scarred uterus, a delivery < 16 months after Caesarean section (CS) increases the risk of complete uterine rupture. 4 With regards to infant health, compared with infants born three years after a previous birth, infants born < 2 years after the previous birth have a high under-five year mortality rate. 5 Hence, postpartum contraception should be offered to women to help them space their pregnancies. Several cultures in Africa have taught the symbiotic relationship between mother and child, with acceptable periods of abstinence being used to space pregnancies. 6
Traditionally, postpartum contraception was only offered to women at the end of the puerperal period, i.e. at the 42nd day after delivery. The reason for this was the belief that ovulation reoccurs 45 days after delivery in non-lactating women. 7 This explains why check-ups were scheduled at the sixth week postpartum.
During this six-week postpartum check-up, it is expected that pregnancy-induced diseases have disappeared. Screening for cervical cancer, immunisation of both the mother (anti-tetanus vaccine to be continued) and the child are done as well as the provision of a contraceptive method to those who did not receive tubal ligation. While waiting for this check-up, women are asked not to resume SI.
Recent studies found that ovulation may resume in some women just 39 days after delivery. 8 A minority of women might even ovulate before this time. 8 Consequently, these women might carry unwanted pregnancies should they have SI while not lactating within the six weeks after delivery, i.e. before provision of a contraceptive method. Unwanted pregnancies are associated with higher rate of induced abortion. In countries where abortion is illegal, it is frequently carried out clandestinely, with numerous complications including maternal death.
We therefore enquired whether nursing mothers regularly resume SI before the 42nd day postpartum. We then studied the factors associated with such resumption as well as the contraceptive method used by these nursing mothers, if any.
Methods
This retrospective cohort study was carried out between 1 January and 15 February 2014. Files of all women who delivered between 15 November and 31 December 2013, whose six-week postpartum check-ups were supposed to be between 1 January and 15 February 2014, were retrieved from archives on 1 March 2014 and reviewed.
In our unit, women admitted in labour are informed of their progression and possible outcomes and their consent is obtained for any surgical procedure. If tubal ligation is to be done, it is carried out during CS or one day after vaginal delivery by mini-laparotomy, under general or local anaesthesia. After delivery, nursing mothers are examined by the resident or obstetrician. Treatment (if required) is given and an appointment for the six-week visit arranged. Counselling is given on the non-resumption of SI during the first six weeks after delivery, especially if tubal ligation was not done.
The variables studied included maternal age, marital status, number of living children, mode of delivery, complications observed at delivery, the recommendation of the six-week postpartum care, the resumption of sexual activity and the method of contraception, if any, being used and the attendance of the six-week postpartum visit.
All women who failed to attend the postpartum visit were successfully contacted by telephone, some after many attempts. The aim of the study was explained and a verbal informed consent was obtained from each. Additional information obtained included name and age (for purposes of identification) and the reason for non-attendance at the postpartum visit. We queried about the resumption of sexual activity, the method of contraception used and the main reason for non-attendance.
The variables were chosen because we assumed that married and younger women, those with few children and those who had uncomplicated vaginal delivery might resume SI earlier. This research has adhered to the STROBE guidelines for observational studies. Our study was approved by the institutional ethics committee.
The necessary sample size was calculated to be at least 81 women, using the formula 9 for cross-sectional descriptive study N = P(1-P) Zα 2 /D2, where Zα = 1.96 corresponds to a confidence level of 0.05, D = 0.1 is the degree of precision, assuming that the prevalence of women who resume intercourse before the sixth postpartum week visit (P) might be 70%. Our data were analysed using SPSS version 20.0. Data of women who resumed SI were compared to those of women who did not. Fisher’s exact test was used to compare categorical variables and t-test to compare continuous variables. P < 0.05 was considered statistically significant. The results are presented as mean ± standard deviation (SD) for quantitative data and frequencies for qualitative data.
Results
We recruited 120 women during the study period, among whom 95 (79.1%) resumed SI within the first six weeks postpartum. Of the 120 women, 85 (70.8%) did not attend the six-week postpartum visit, while 35 women (29.2%) did. Of the former 85, all were contacted by telephone; 65 (76.5%) were found to have resumed SI. Moreover, 30 of the latter 35 (85.7%) had also resumed SI before this visit.
Demographic and obstetrical characteristics of nursing mothers.
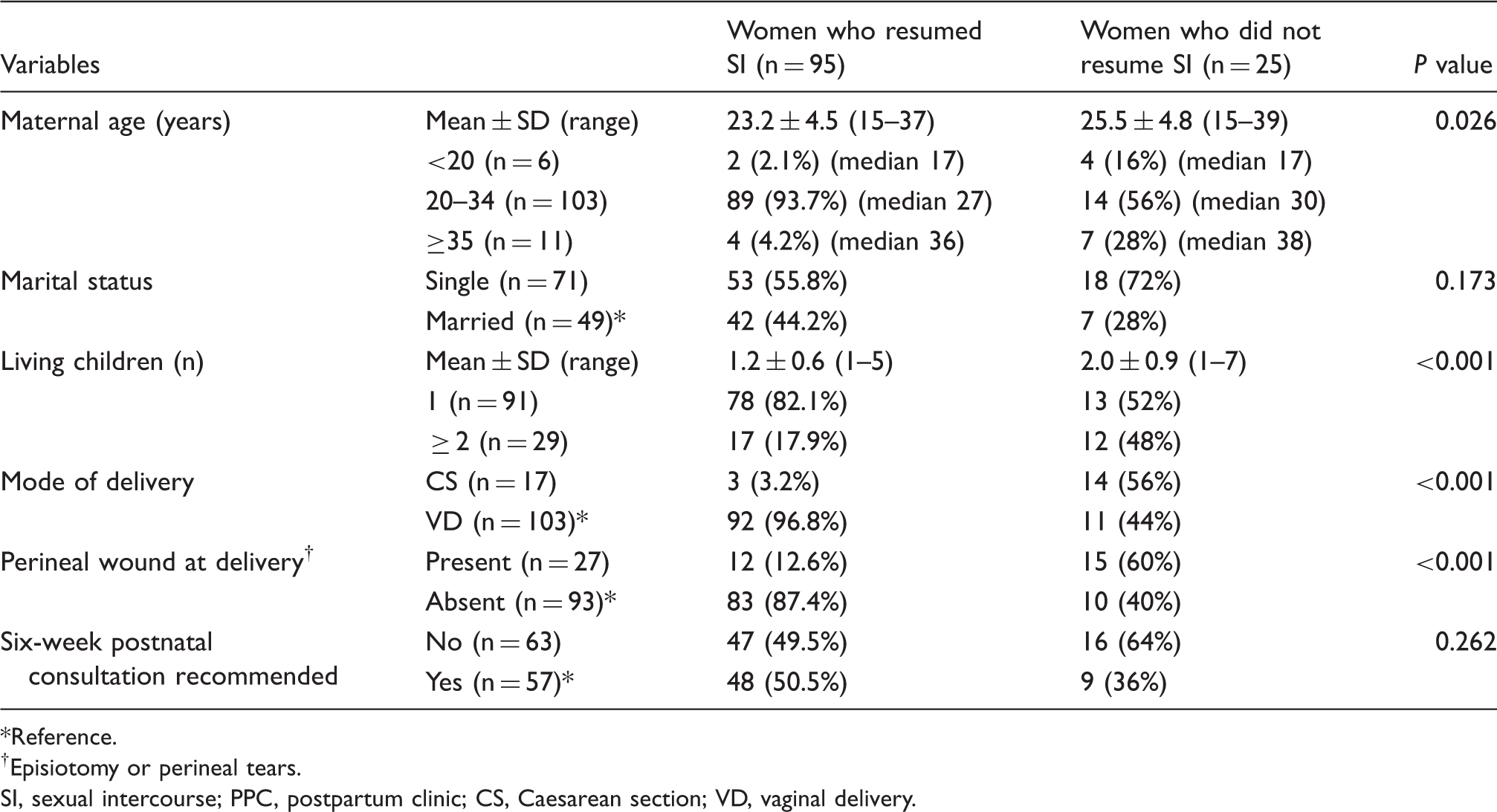
Reference.
Episiotomy or perineal tears.
SI, sexual intercourse; PPC, postpartum clinic; CS, Caesarean section; VD, vaginal delivery.
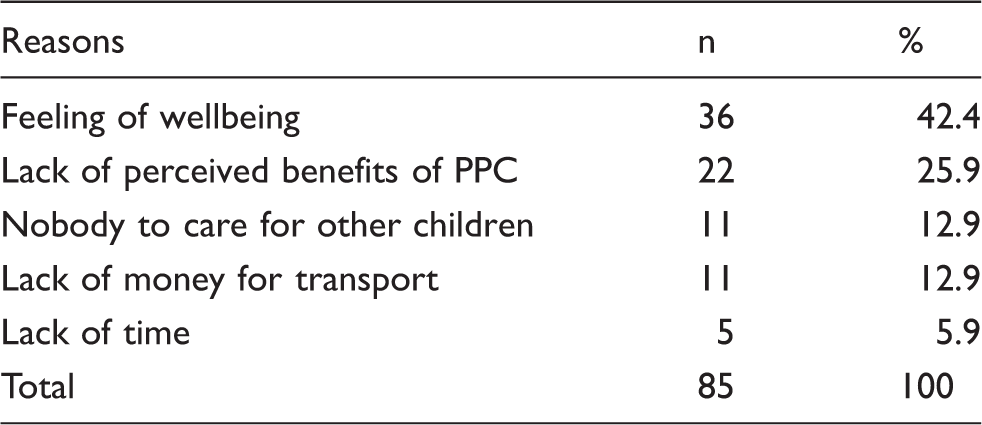
Reasons for non-attendance of the six-week postpartum clinic (PPC).
Women presenting for postpartum care were significantly more likely to have undergone CS, experienced perineal trauma during delivery (episiotomy or perineal lacerations) and received recommendation to attend the six-week postpartum visit.
There was no significant difference among those who resumed SI, whether or not they attended the postpartum visit (P = 0.321). Women aged 20–34 years resumed SI more than those aged < 20 years or ≥ 35 years (89/95 or 93.7% vs. 14/25 or 56%, P < 0.001).
As regards the number of living children, 5/6 women aged < 20 years (83.3%) had only one child while 10/11 (90.9%) women aged ≥ 35 years had at least two children. Concerning women aged 20–34 years, 85/103 (82.5%) had one child while 18 (17.5%) had ≥ 2 children. Resumption of SI before the six-week visit was more frequent among women who had only one living child (78/91 or 85.7%) than among those with two or more children (17/29 or 58.6%) (P < 0.004).
Of the 95 women who resumed SI, 12 (12.6%) had perineal trauma at delivery (eight tears and four episiotomies) while 15/25 (60%) who did not resume SI had perineal trauma (13 tears and two episiotomies). Among the 21 perineal tears, 20 were first-degree and second-degree tears. Four of the six adolescents (66.6%) had perineal trauma. One woman aged 18 years with a third-degree perineal tear did not resume SI. Two women aged 19–23 years who had forceps delivery for acute fetal distress and prolonged second stage of labour, respectively, did not resume SI. Resumption of SI before the six-week visit was more frequent among women who had delivered vaginally (P < 0.001) and had an uncomplicated delivery (P < 0.001) (Table 1).
Married women were more prone to have SI before the six-week postpartum visit than single women (42/49 or 85.7% vs. 53/71 or 74.6%), but the difference was not statistically significant (P = 0.173) (Table 1). Unsurprisingly, women who did not have perineal trauma at delivery (genital lacerations or episiotomy) were more prone to resume precocious SI than those who did (P < 0.0001).
Methods of contraception used by the 95 sexually active women.

PPC, postpartum clinic; LAM, lactational amenorrhoea method.
During the period under study, no tubal ligation was carried out whether during CS or in the early postpartum period.
One major limitation of our study is our inability to verify the veracity of all answers obtained over the telephone.
Discussion
A majority of women resuming SI within the first six weeks postpartum is obviously much higher than the rate of 21.6% observed in Uganda. 10
In our country, many women, including grand multiparous women, prefer reversible contraception. Furthermore, they have to pay the extra cost for tubal ligation, even if performed during CS. This might explain why no tubal ligation was performed. Such women would probably have accepted sterilisation if it was free of charge. Studies should be carried out in our country to explain the non-compliance of women to sterilisation. Tubal ligation also offers some benefits by protecting against ovarian and tubal cancers. 11
It is therefore inappropriate to offer a contraceptive method six weeks after delivery. A contraceptive method should be offered before the nursing mother is discharged from the hospital. This point of view is shared by many other authors. 12 Nonetheless, LAM, when well-conducted, has a 98% protection rate over the first six months. 13
Women who did not resume SI included adolescents as 66.6% of them had perineal trauma; as some were single, they suffered no pressure from the presence of a partner. Furthermore, the advent of an unintended pregnancy may reduce early sexual desire. The care of > 2 children have reduced the propensity for SI for those aged > 35 years.
Furthermore, those who had a vaginal delivery reported greater wellbeing than those who had undergone CS, presumably still suffering with pelvic pain. Those who had had perineal repairs usually waited for confirmation of complete perineal or vaginal healing by their physician before starting SI. Such attitudes are by no means universal.
Contraceptive methods and/or LAM should therefore be discussed at the time of discharge, as attendance at follow-up is unreliable. Home visits should be encouraged in our country given that they have been associated with better maternal and neonatal care elsewhere.14,15
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.