
Abstract
Tuberculosis (TB) is a common opportunistic infection which may be reactivated in immunocompromised patients. The incidence of hepatocellular carcinoma (HCC) is on the rise with healthcare resulting in increased longevity of people. Reactivation of TB has been reported with liver-directed therapies for HCC like transarterial chemoembolisation (TACE) and transarterial radio-embolisation (TARE). However, the co-occurrence of both TB and HCC in the same patient without any such history is rarely found. Only three isolated case reports have been published previously. We report the case of an elderly hepatitis C virus-related chronic liver disease patient who developed two different nodular liver lesions with multiple intra-abdominal lymphadenopathy, one such nodule being confirmed as HCC and another as TB along with nodal TB.
Background
Tuberculosis (TB) is endemic in India and therefore exists as a virtually universal differential diagnosis. The reactivation of TB is a well-known phenomenon, occurring mostly in the setting of an immunocompromised state. 1 TB reactivation is difficult to treat and requires more aggressive management. TB reactivation is frequently seen in haematological malignancies, immunocompromised patients, and after TACE and TARE for hepatocellular carcinoma (HCC).2–4 Cirrhosis from any aetiology puts a patient at increased risk of HCC. With the availability of newer and potent antiviral drugs for hepatitis C, the natural history of these infections may be favourably altered and further progression to cirrhosis, end-stage liver disease and HCC may be halted. The simultaneous occurrence of TB with HCC on the background of hepatitis C virus (HCV) has been rarely reported owing to potent anti-tubercular treatment nowadays.5–7 We hereby report such a case.
Case report
A 70-year-old man, known to have diabetes mellitus and systemic hypertension, was diagnosed as having hepatitis C genotype 3 related chronic liver disease in April 2018 with a HCV RNA load of 715,600 IU/mL. After 12 weeks of sofosbuvir + velpatasvir treatment, repeat HCV RNA in August 2018 was undetectable. On regular follow-up, he was progressing well until September 2018.
Laboratory investigation on patient.
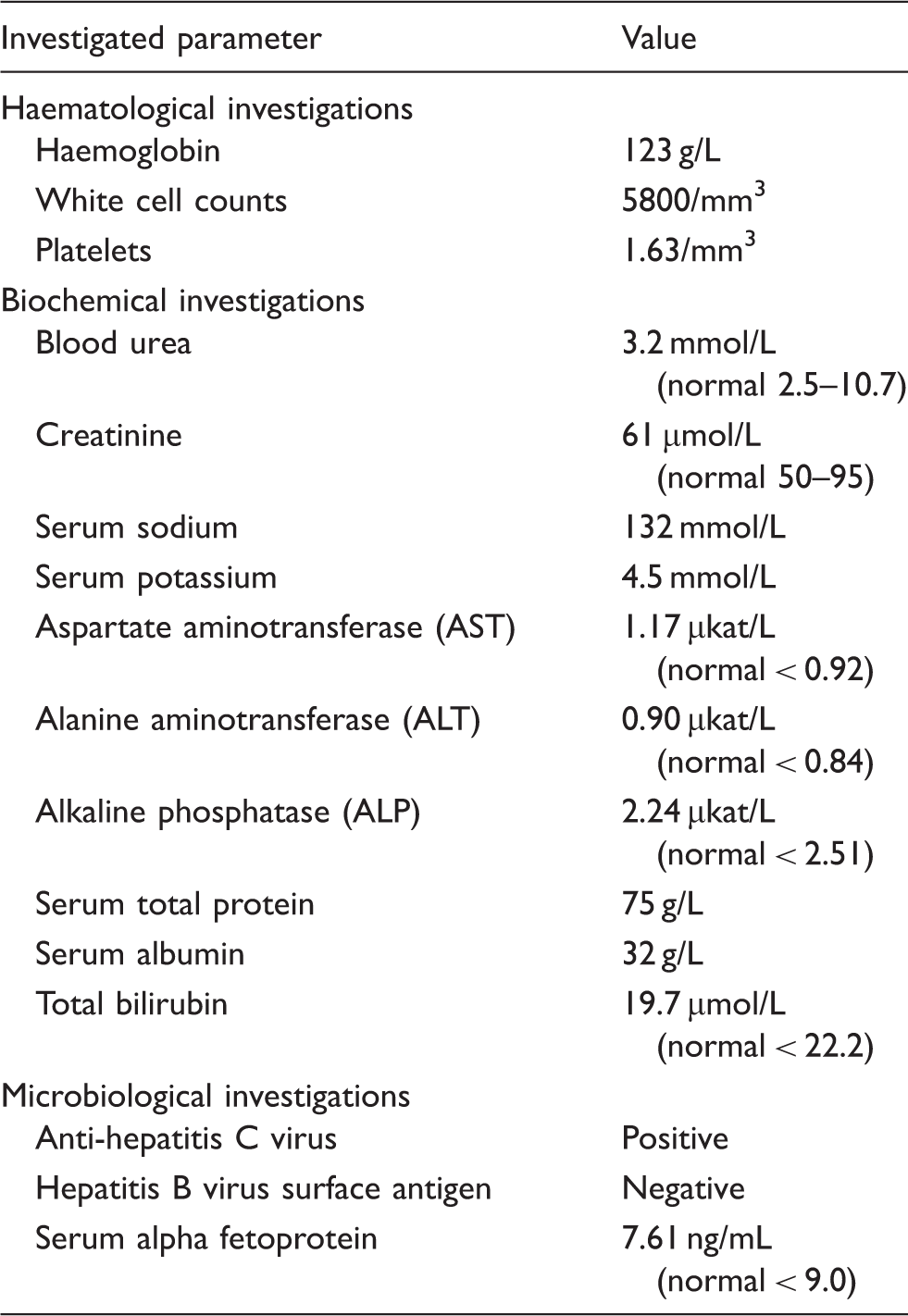
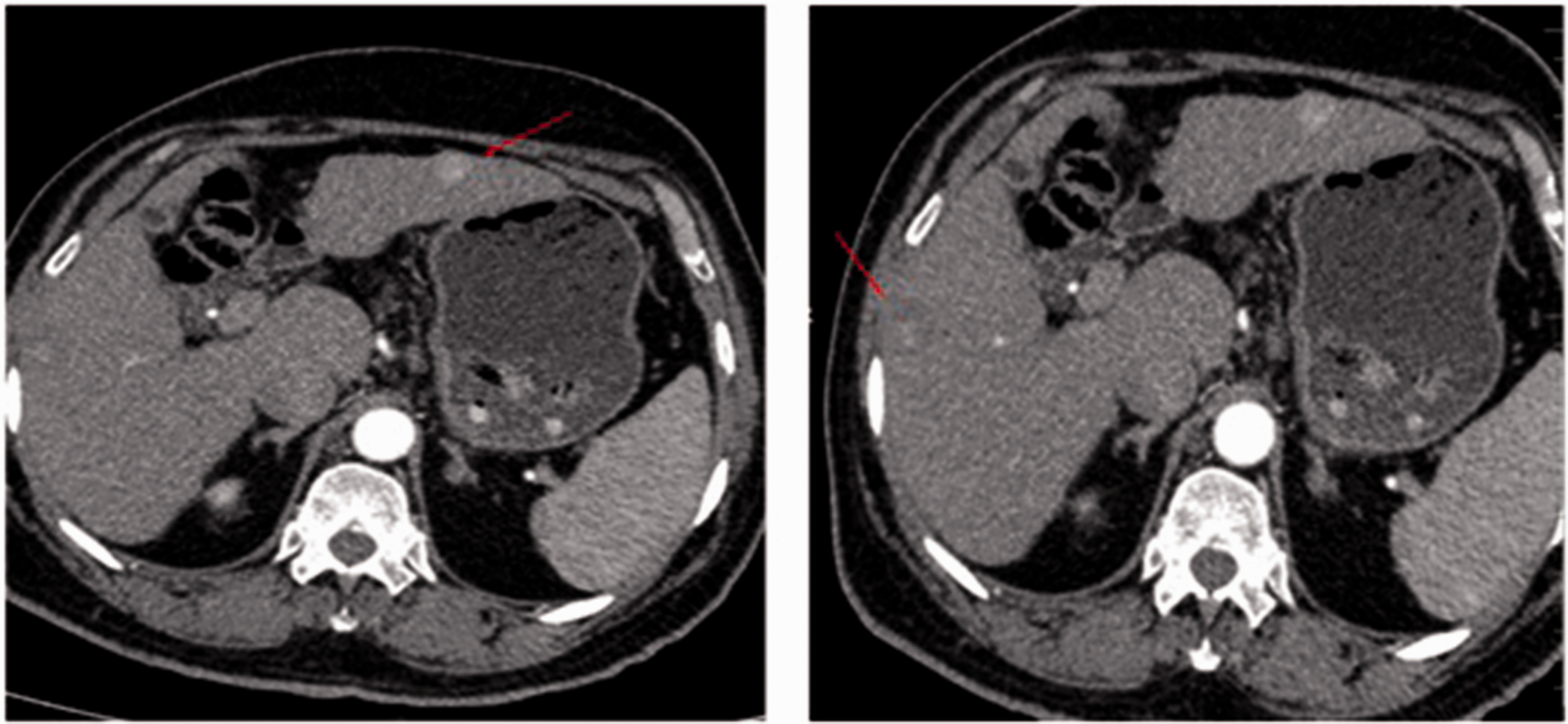
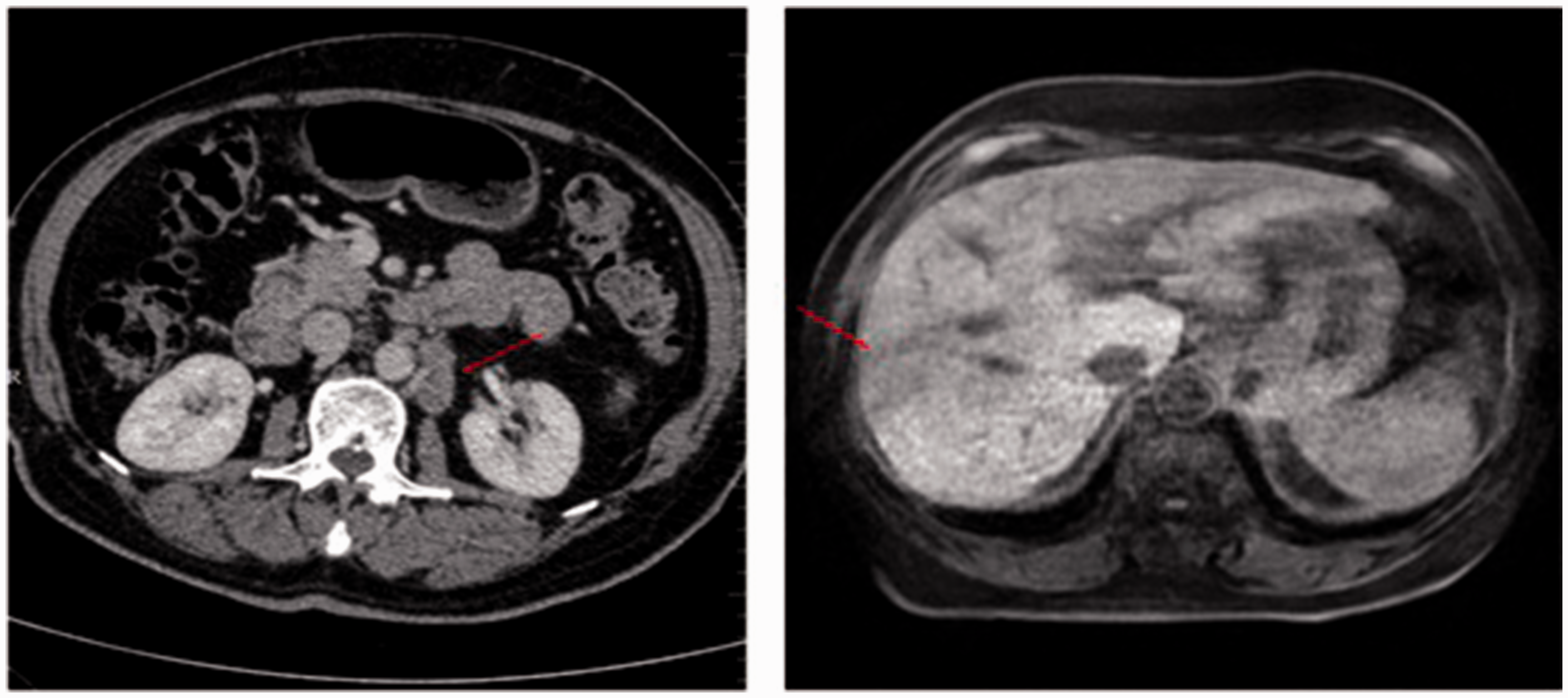
The normal serum alpha fetoprotein warranted further evaluation; so triple phase CT scan was done which showed a well-defined heterogeneous lesion of 2.0 × 1.6 cm in size in liver segment III then with arterial hyper-enhancement and heterogenous enhancement in the venous phase. (Figures 1 and 2), also a well-defined suspicious heterogeneous non-enhancing lesion, 2.0 × 1.6 cm in size, was noted in segment V with caudate lobe hypertrophy of a hypertrophied liver; para-aortic, aortocaval, bilateral external iliac and common iliac lymphadenopathy were seen (Figure 3). Core needle biopsy of segment 3 nodule showed periportal to intralobular chronic inflammation with cores of a tumour arranged as nests, with surrounding necrosis, trabeculae and closely packed pseudoglandular structures lined by polygonal cells with enlarged, vesicular nuclei, prominent nucleoli and abundant granular cytoplasm, with paucity of reticulin within atypical cell foci, all suggestive of well-differentiated HCC on a background of cirrhosis (Figure 4a and 4b).
Left- USG abdomen showing liver surface nodularity and caudate lobe. Left-nodule in segment 3 with hyper-enhancement on arterial phase. Right- a heterogenous non enhancing lesion in segment V with hypertrophy of caudate lobe. Right-enlarged para aortic lymph node. Left-non enhancing lesion in segment V. (a) Cirrhotic background surrounding areas of infiltrating tumor cells. (b) HCC in the background of cirrhosis. (c) caseous granuloma of segment V of liver. (d, e) caseous granuloma of para aortic LN.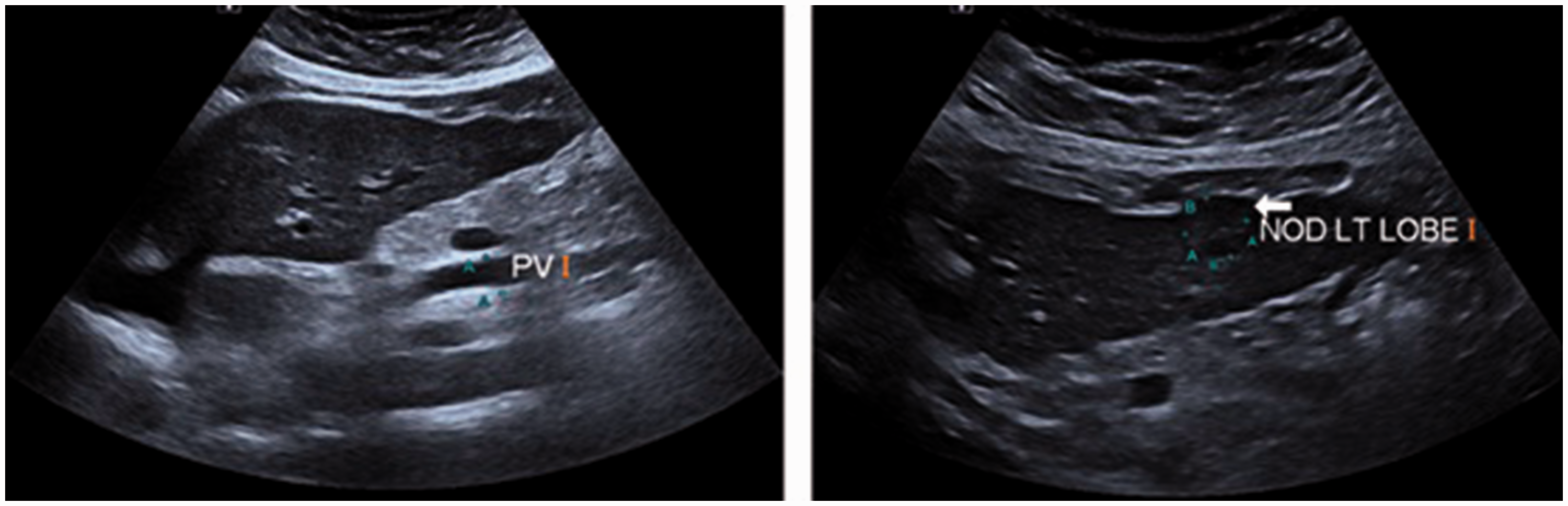
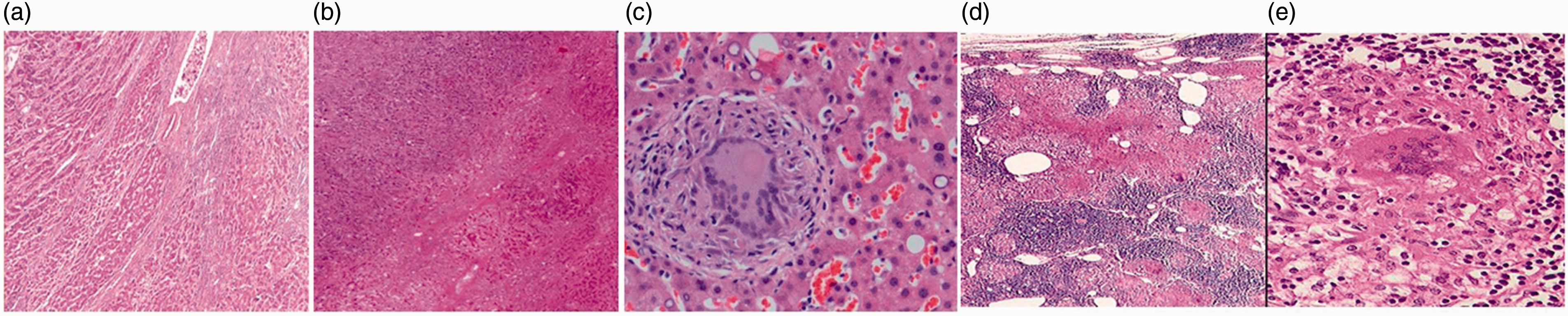
Biopsy from the segment V liver nodule showed multiple granulomas, coalesced into a conglomerate tubercle, with central caseation of epithelioid and Langerhans giant cells, suggestive of TB (Figure 4c). Core left para-aortic needle biopsy showed necrotising granulomatous inflammation with multinucleated giant cells of Langhans type and moderate lymphocytic infiltrate with few histiocytes with no evidence of malignancy (Figure 4d and 4f).
Treatment with radiofrequency ablation of the segment 3 nodule was carried out. Subsequent first line anti-tubercular treatment with isoniazid (300 mg), rifampicin (450 mg), pyrazinamide (750 mg) and ethambutol (800 mg) was continued for two months with consolidation treatment using the first two drugs for a further four months. After the treatment was initiated, the patient’s appetite improved and weight loss was reduced. Blood parameters in February 2019 returned to normal.
Discussion
The moral of our case is that clinicians should not refrain from taking biopsies whenever the clinical, imaging and laboratory investigations do not match. Aggressive treatment of both diseases simultaneously provides a good outcome. Even in the presence of cirrhosis, provided normal baseline liver function pertains, routine first-line anti-tubercular treatment can be safely administered.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.