
Abstract

Introduction
While Type 1 reaction is seen in leprosy patients, in up to 30% 1 of patients, late reaction is uncommon and is seen in the first two years of release from treatment (RFT). 2 It is believed that these reactions are consequent to dead bacilli and the World Health Organization (WHO) recommends treatment with steroids without multidrug therapy (MDT; with the proviso of adding clofazimine only when steroid therapy exceeds four months duration). 3 A few studies, though, have noted live bacilli present in reversal reactions and hence recommending concomitant MDT.1,4 We report a case of resistant bacilli in a late reaction and discuss the implications of this finding.
Case report
A 60-year-old man, diagnosed as having lepromatous leprosy based on clinical and histopathological findings, completed 12 months of MDT with complete clearance of skin lesions and remained free of symptoms for two years after RFT. He presented with sudden onset of painful, red, raised lesions over the trunk, upper and lower limbs associated with mild malaise. These were erythematous annular mildly tender lesions not associated with new sensory loss (Figure 1) or neuritis.
Erythematous annular mildly tender lesions over the trunk.
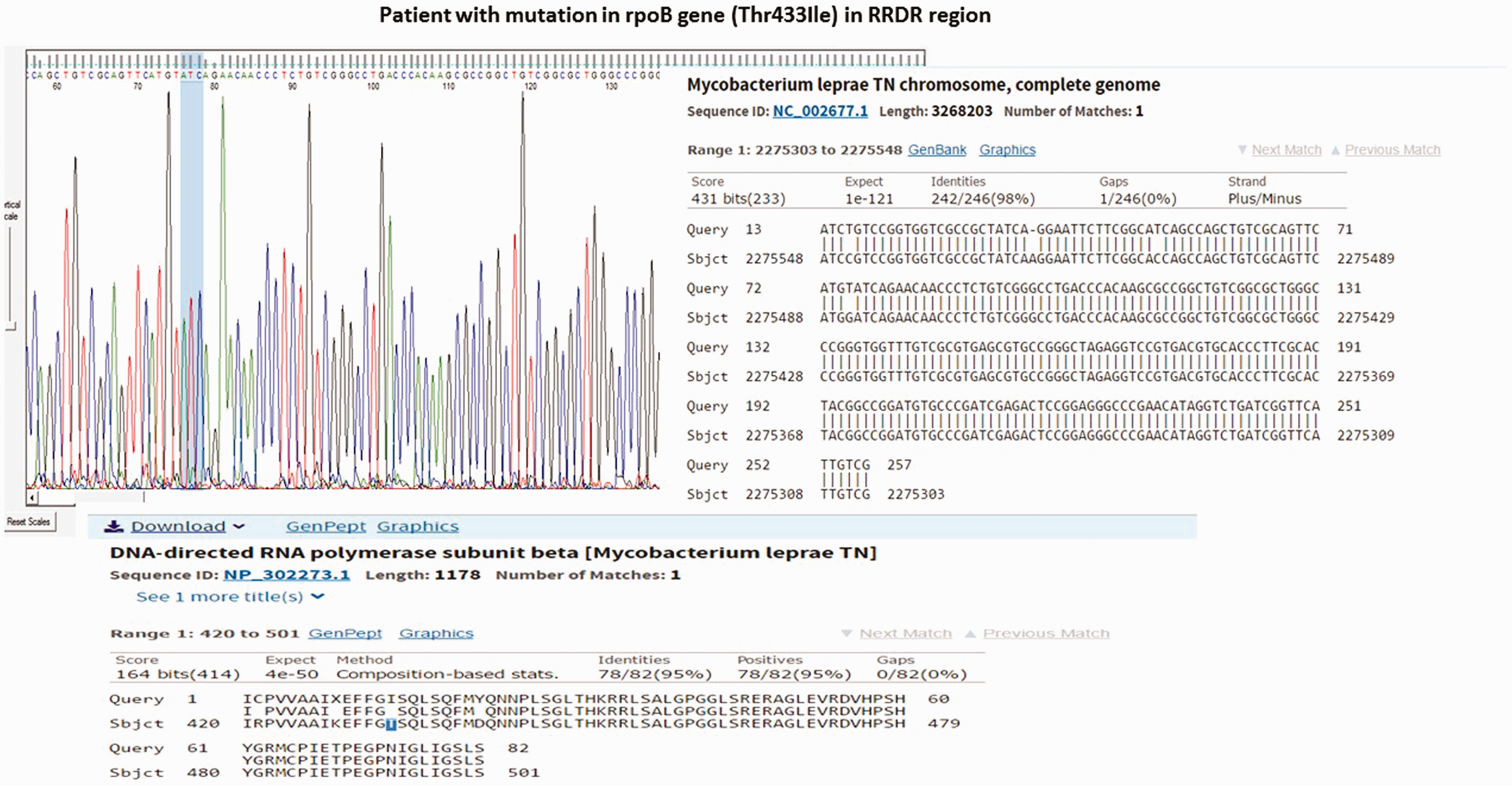
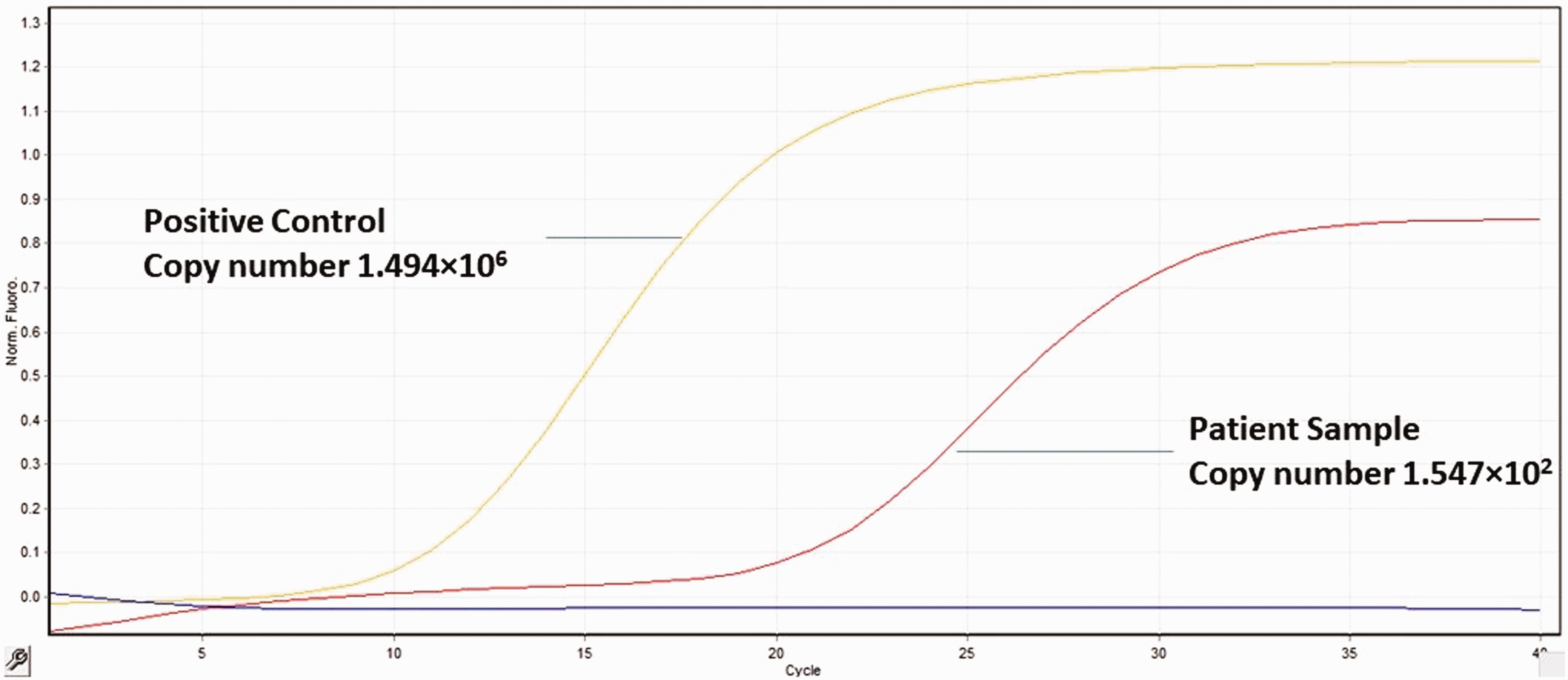
Slit skin smear revealed a Bacillary Index (BI) of 3+ and Morphological Index (MI) of 0. As the clinical picture was suggestive of a late reaction, prednisolone 40 mg was commenced with a gradual tapering of the dose over four weeks. All lesions settled with post-inflammatory hyperpigmentation within 10 days (Figure 2). Histopathology revealed oedema superimposed on a mild-to-moderate perivascular foam cell infiltrate. The resistance report revealed mutation in rpoB gene with a change in amino acid threonine to isoleucine at codon position 433 (Thre433Ile) indicating rifampicin resistance (Figure 3). A viability-based assay targeting the 16 S rRNA gene region using real-time polymerase chain reaction (PCR)
5
showed viable bacilli (1.54 × 102) (Figure 4). Consequently, second line drugs
6
(clofazimine 50 mg, ofloxacin 400 mg and minocycline 100 mg daily) were commenced for six months, followed by clofazimine and ofloxacin for a further 18 months.
All the lesions settled with PIH on prednisolone within 10 days. Mutation in rpoB gene (Thr433Ile). Amplification of the 16rRNA region using real-time PCR.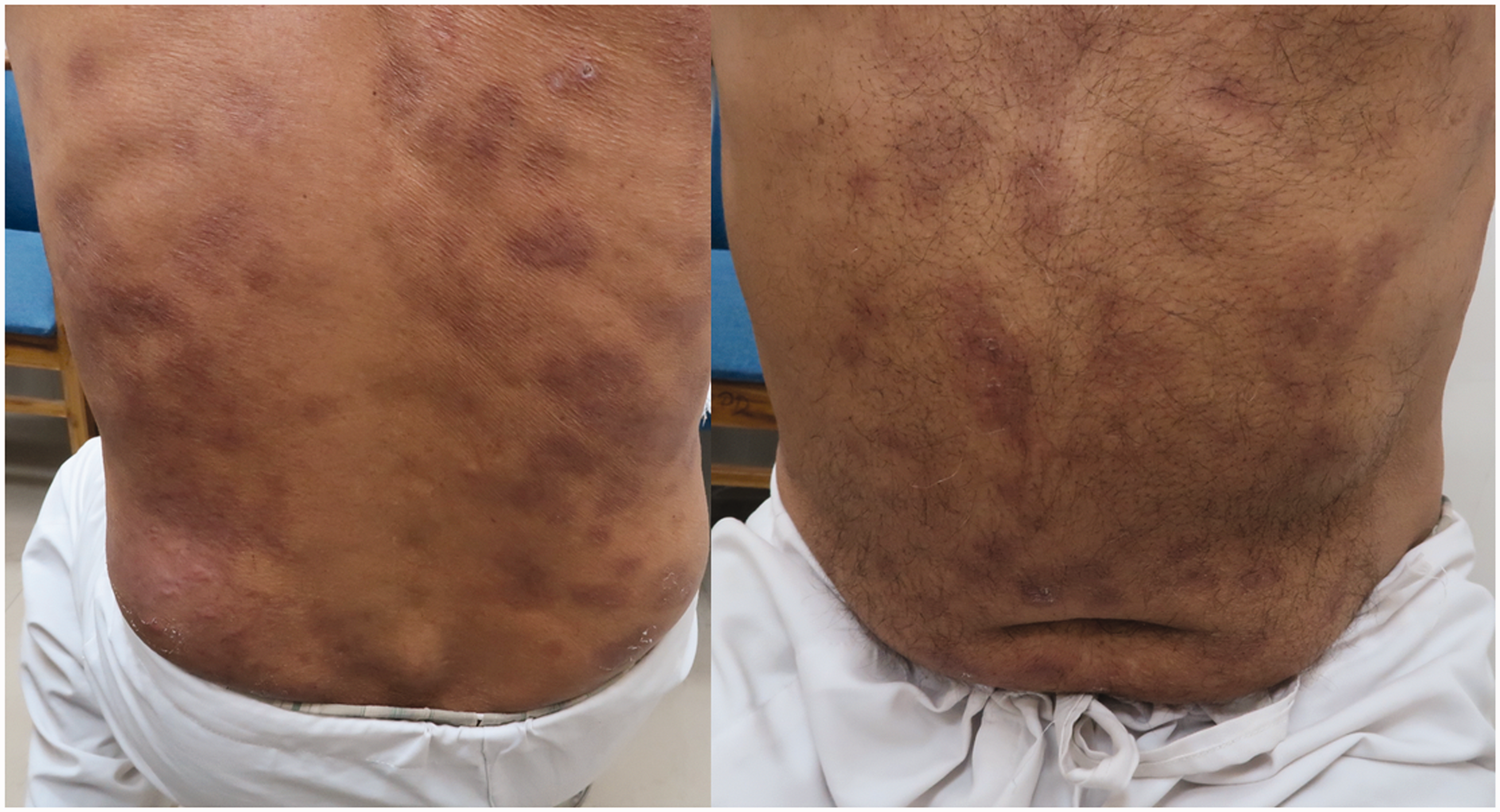
Discussion
Late type 1 reaction was believed to be an immunological response to dead bacilli. This was thought to precede or follow relapse and the role of bacilli, live or dead, was suggested as a possible trigger.7,8 This presupposes the fact that a reversal reaction may occur owing to re-multiplication of Mycobacterium leprae, thus increasing the antigenic load. Further, whether an upgrading or downgrading reaction occurs, depends upon the type of antigenic determinants against which immunity has developed, as well as T-cell subsets, profile and individual genetic makeup.9,10 Our case demonstrates that, in a case of late type 1 reaction, the role of viable and resistant bacilli has important therapeutic implications.
The clinical morphology, onset within two years of RFT, MI = 0 and a dramatic response to steroids, are suggestive of a late reaction. While viable bacilli have been demonstrated in a Type 1 reaction, the two studies that detailed this finding1,4 could not enunciate a plausible reason for viable bacilli even after completion of MDT, though the presence of persisting bacilli may be a plausible explanation. We feel that the presence of viable bacilli in a late reaction may be explained by resistance which was not documented in previous studies, although we confirmed it (Figure 3) in our case. While a mouse foot inoculation would be ideal to confirm viable bacilli, we do not have this facility.
While the rifampicin resistance in our patient could either be primary or secondary, we are inclined to believe that the latter is correct The rationale of the combination of drugs is based on the fact that while rifampicin kills > 99% of organisms present at the start of treatment (equal to 3–6 months of daily treatment with the combination of dapsone and clofazimine), mutants resistant to dapsone and clofazimine are fully susceptible to rifampin and are killed by the first dose, whereas it takes a much longer duration of daily dapsone and clofazimine to get rid of rifampin-resistant mutants. 11 Furthermore, Grosset et al. 12 have suggested that to select out rifampicin-resistant mutants, more than six doses, and possibly as many as 50 doses, of rifampicin need to be administered. Thus, if there was primary resistance, the patient would have shown signs of deterioration while on therapy (two years of MDT) or early reactivation. In our case, not only was the patient discharged with subsidence of the lesion, the presentation after two years makes primary resistance unlikely. Whether these bacilli were persisters remains unproven and there is no method of confirming this premise.
The therapeutic intervention recommended by WHO in late reaction3 of administering steroids is based on the premise that it would suppress a reversal reaction and prevent or ameliorate any associated nerve damage, whereas this treatment would only partially and temporarily suppress a reaction due to viable bacteria (and the latter would continue to multiply during this period of steroid immunosuppression, so that acid fast bacteria might be more easily detected in smears). Thus, if a lesion subsides and remains so after stopping steroids, the presumptive diagnosis is a reversal reaction. On the other hand, if the lesion does not subside, or reappears during the period of observation, it is most probably a relapse needing anti-leprosy treatment. 13 The logic of steroid treatment alone is based on the finding that a tapered steroid regime over 12 weeks did not prejudice the clearance of M. leprae. 14
In our case, there was no evidence of activity of disease after reducing steroid therapy, thus revalidating our diagnosis of late reaction, but we nevertheless initiated second line drug on receiving the report of resistance according to WHO guidelines. 6 The rationale of this combination was based on the seminal studies that showed that ofloxacin, in a daily dose of 400 mg, killed > 99.99% of viable M. leprae after only four weeks of therapy while minocycline 100 mg took eight weeks to do the same. Moreover, a single pulse of both ofloxacin 400 mg and minocycline 100 mg was able to kill 68–98% of viable M. leprae.6,15
The practice of administering steroids without cover of MDT is prevalent, even though two papers have documented via mouse foot pad inoculation studies and viability markers that are viable as opposed to dead bacilli that play a role in reactions.1,4 Furthermore, these bacilli have been documented even in smear-negative with reaction cases with reaction. The WHO recommends that clofazimine, 50 mg daily, should be given as a prophylactic measure only if the duration of corticosteroid therapy is expected to exceed four months. 3 The need for MDT along with steroids may be unnecessary if, as has been shown, tapering steroid treatment does not prejudice the clearance of M. leprae. However, the advantage of giving MDT with steroids is that there is still a small risk of relapse in patients only on steroids since they are known to accelerate the multiplication of organisms located in dormant foci, which may cause disseminated reactivation. In addition, the presence of resistant bacilli hitherto unreported in reaction may perpetuate the disease.
Thus, recommendations 3 may need to be revisited in a case with resistant bacilli. Our case raises the larger issue of testing for resistance in certain cases of chronic, recurrent or delayed reactions in leprosy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.