
Abstract
Organophosphorus compounds (OPC) are commonly used pesticides and suicidal ingestion is a common mode of poisoning. The manifestation of OPC poisoning and its severity depend upon the type, dose and potency of the OPC consumed. Neurological presentations are well defined clinical syndromes consisting of early, intermediate and delayed manifestations (rare), categorised on the basis of time elapsed since OPC exposure. We report a rare delayed manifestation of organophosphorus poisoning in the form of pure motor spastic paraparesis due to dorsal myelopathy. A possibility of delayed manifestations of toxicity should be considered in individuals presenting with features suggestive of myelopathy and a previous history of organophosphate exposure.
Keywords
Case report
A 21-year-old man presented with a history of having consumed 100 mL of pesticide (chlorpyriphos 50%) with suicidal intent 18 months previously, following which he developed altered sensorium. He was managed with gastric lavage, atropine infusion and symptomatic treatment. He improved over the following three weeks and was discharged with ability to carry out all activities of daily living. Two months later, he developed proximal followed by distal weakness of the lower limbs, which progressed over three days with difficulty in ambulation. He also developed stiffness of both lower limbs over the next month. At presentation, he had spasticity (modified Ashworth scale grade 2) with motor weakness (MRC grade 4/5) in both lower limbs. Lower limb deep tendon reflexes were brisk with extensor plantar responses. Motor examination in the upper limbs and the remaining neurological examination were normal.
Routine investigations including complete blood count, hepatic and renal function tests, thyroid function, vitamin B12 level, HIV serology and Venereal Disease Research Laboratory (VDRL) tests were all normal. Electrophysiological studies including nerve conduction studies of all four limbs, electromyography, visual and auditory evoked potentials were normal. Somatosensory evoked potentials (SSEP) were prolonged beyond the popliteal fossa in the lower limbs but normal in upper limbs. Magnetic resonance imaging (MRI) scan of the spine showed dorsal cord atrophy (Figure 1), but of the brain was normal.
MRI of the spine: (a) sagittal section: T2 sequence, red arrows exhibit dorsal cord atrophy; (b) axial section: T2 sequence, dorsal spine: exhibiting cord atrophy.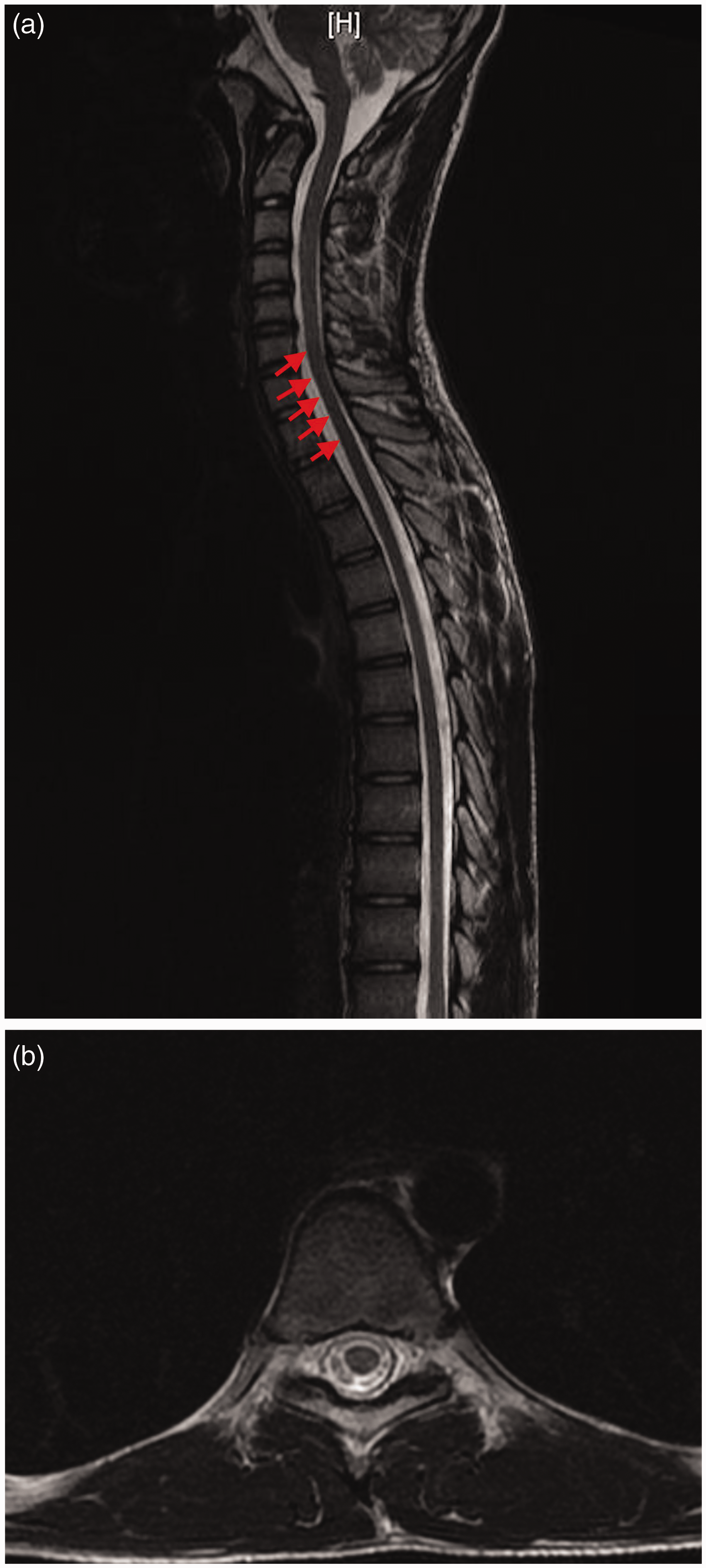
Discussion
OPCs are commonly used as pesticides, lubricants and petroleum additives. They can enter the human body through absorption from the skin, by being ingested or inhaled. 1 Suicidal ingestion is the most common mode of poisoning in India.2,3 The severity of poisoning depends upon the mode of ingestion, dose consumed, quality and type of organophosphate exposure. 3 Chlorpyriphos (diethyl 3, 5, 6-trichloro-2-pyridyphosphorothionate) is a broad spectrum OPC. 4 It is itself inactive but after oxidative desulfuration in the liver, is converted to chlorpyriphos oxon, which can inhibit both central and peripheral esterases producing neurotoxicity. Delayed myelopathy occurring 18 months after chlorpyrifos ingestion has been reported in four cases: (1) a young man with delayed onset spastic quadriparesis with bladder involvement with associated pure motor neuropathy, which developed six weeks after exposure to chlorpyriphos; 5 (2) a young woman with similar history; 6 (3) a young woman with spastic quadriparesis and sensory motor neuropathy developing 18 months after exposure to phosphamidon and mevinphos; 7 and (4) an adult with spastic quadriparesis with bladder involvement and sensory motor neuropathy developing two months after exposure to malathion. 8
Three clinical syndromes can result following OPC ingestion: Type I (acute muscarinic); Type II (intermediate nicotinic); and Type III (organophosphate-induced delayed neuropathy [OPIND]).
The acute muscarinic phase occurs as a result of the accumulation of acetylcholine due to the phosphorylation and inhibition of acetylcholinesterase, causing a depolarisation block at receptor sites. 9 These effects appear within minutes of consumption and induce excessive secretions, bradycardia and hypotension. 9 Neurological manifestations include seizures, tremors, restlessness, drowsiness and coma, and occur only with agents that can cross the blood–brain barrier. All these manifestations respond to atropine.
Our patient had also developed central nervous system (CNS) symptoms with altered sensorium a few hours after chlorpyriphos ingestion and responded initially to atropine and symptomatic treatment.
An intermediate syndrome occurs 1–4 days after exposure to OPC and can last up to three weeks.9–11 These nicotinic effects are sympathetic and include fasciculations, cramps, muscle (including bulbar and respiratory) weakness with depressed reflexes and reflect failure of transmission at the neuromuscular junction. Delayed manifestations are rare, occurring 2–8 weeks after exposure to OPC. 2 The mechanism of delayed toxicity is postulated to occur due to neuropathy target esterase (NTE) inhibition leading to a central and peripheral axonopathy with Wallerian degeneration. 12
Not all OPCs cause OPIND because significant inhibition is required for the same and OPCs differ in their anti-NTE activity. Delayed manifestations commonly occur in high dose exposures of potent agents 4 and occur over four phases: latent; progressive; stationary; and improvement. 12 The latent period occurs 2–3 weeks after exposure to OPC. This phase was slightly longer in our patient (approximately eight weeks), as reported previously. 13 The progressive phase is associated with rapidly advancing sensory or motor polyneuropathy, predominantly affecting the lower limbs. Common sensory symptoms include cramps and paraesthesia in the lower limbs and signs include ‘glove and stocking’ sensory loss. 14 The stationary phase is associated with stabilisation of symptoms for months to years. In the improvement phase, sensory symptoms disappear followed by improvement in motor weakness. However, this is frequently incomplete. 4 CNS damage is unmasked as the peripheral nervous system recovers slowly and manifests with spasticity and brisk reflexes as seen in our patient.
Our patient presented with a history of pure motor spastic paraparesis 18 months after acute toxicity with chlorpyrifos, which is consistent with acute and delayed manifestations of the same. This is a rare manifestation and usually occurs with high dose exposure to potent OPC and should be considered in patients with history of exposure and progressive myeloneuropathy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.