
Abstract
We investigated the accessibility of height- and weight-measurement tools and the awareness of one's own height and weight in a specific population in West New Britain Province (WNBP), Papua New Guinea, where obesity is prevalent. Of 558 participants (mean age 34.8 ± 14.0 years, 48.2% women, average body mass index =25.1 ± 4.83 kg/m2), >70% had limited access to measurement scales and 97.5% lacked accurate knowledge of their own height and weight. Our findings imply that increased access to measurement tools and awareness of personal height and weight is necessary to improve the feasibility and effectiveness of weight-management interventions in areas such as WNBP.
Introduction
Papua New Guinea (PNG) is one of numerous countries facing the challenges of non-communicable diseases (NCDs), which are responsible for 56% of deaths in this country. 1 Excess body weight is a risk factor for NCDs, 1 and the percentage of people in PNG who are overweight or obese is approximately 30%. 2 Thus, weight management represents an urgent public health challenge. 3
According to several literature reviews,4–7 regular self-monitoring of body weight is a promising weight-management method when implemented as part of multi-component regulation strategies (MRSs), which comprise self-monitoring (dietary intake and physical activity) and behavioural-change intervention. Regular and frequent self-weighing can increase personal awareness of current weight as well as weight patterns; such awareness must surely be mandatory for self-evaluation and self-adjustment in relation to weight. 7
Some researchers, however, have noted that weighing scales are not available in some low- and middle-income countries (LMIC).8,9 Because of such restrictions, individuals have limited knowledge, or even total unawareness, of their own weight and body mass index (BMI). This must impede MRSs.
Residents of PNG, which is categorised as a LMIC, 10 appear to face similar weight-monitoring challenges. The present study examined a sample of community-dwelling people in West New Britain Province (WNBP), PNG, seeking to investigate this assumption. We had two specific aims: (1) to clarify the availability of scales for measuring height and weight and participants' experience regarding taking measurements; and (2) to examine participants' knowledge of their own height and weight, and the accuracy of this knowledge.
Ours was a cross-sectional questionnaire-based survey. Data collection was conducted in a single local community in WNBP from 29 November to 19 December 2019. The clinical service directorate of Kimbe Provincial Hospital approved this study. Informed consent was obtained from all participants.
Researchers established a temporary survey site at Kimbe, a downtown area located in central WNBP. Participant recruitment was conducted using a convenience-sampling method. Individuals at the survey site were approached by the researchers and asked to participate in this survey. The inclusion criteria were: healthy community-dwelling adult or child; of any sex, age, race or religion; and the ability to walk independently around town. We excluded participants who could not communicate effectively in English.
Descriptive analysis results presented in terms of age group.
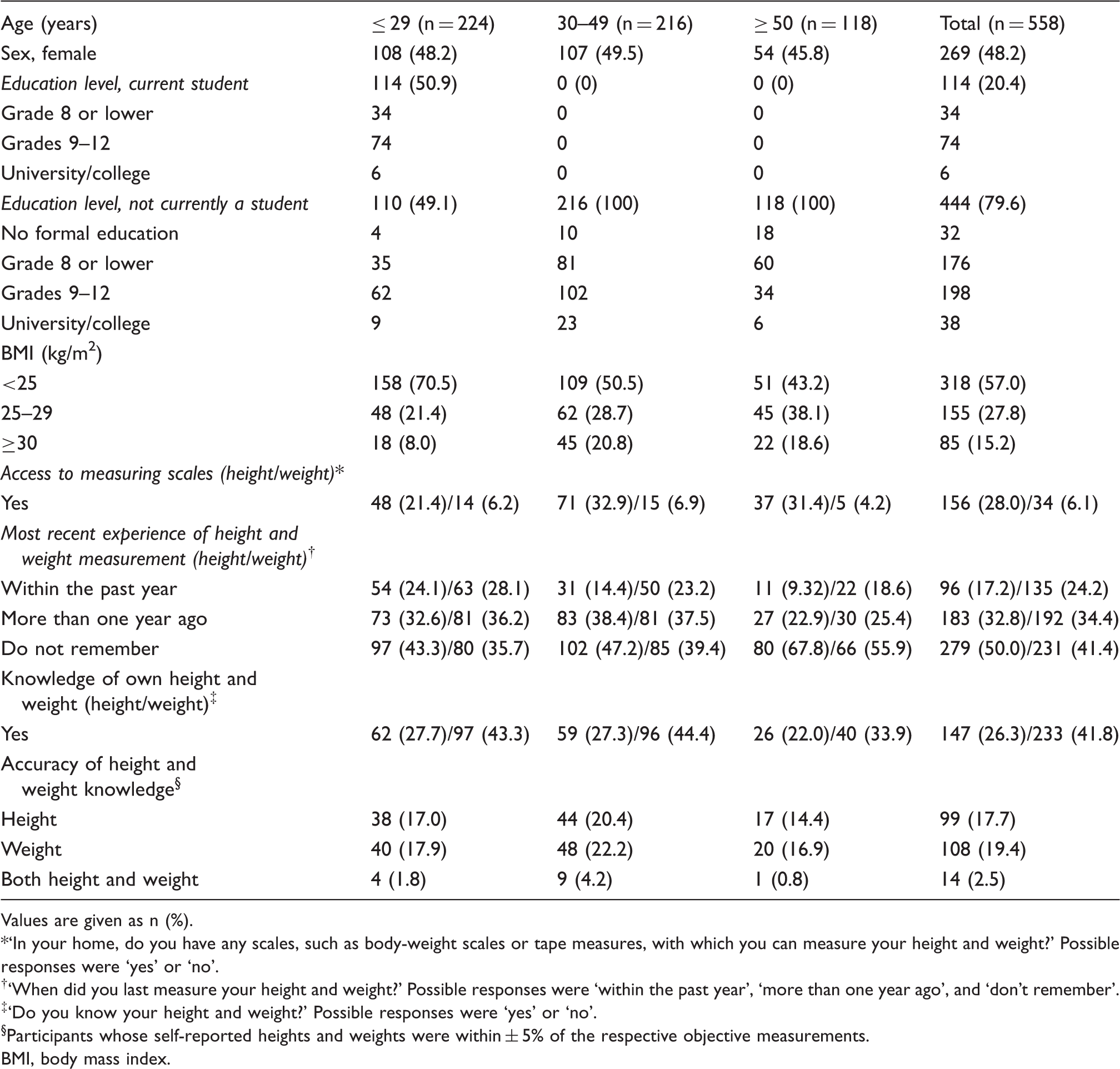
Values are given as n (%).
‘In your home, do you have any scales, such as body-weight scales or tape measures, with which you can measure your height and weight?’ Possible responses were ‘yes’ or ‘no’.
‘When did you last measure your height and weight?’ Possible responses were ‘within the past year’, ‘more than one year ago’, and ‘don't remember’.
‘Do you know your height and weight?’ Possible responses were ‘yes’ or ‘no’.
Participants whose self-reported heights and weights were within ± 5% of the respective objective measurements.
BMI, body mass index.
Personal knowledge regarding height and weight was confirmed if self-reported figures were within ±5% of our respective objective measurements.
For descriptive purposes, we calculated the numbers, percentages, means and standard deviations (SDs) of data by age groups.
Results
Of the 565 participants initially recruited, seven were excluded from final analysis due to missing data (n = 3) and refusal to participate (n = 4). The average ± SD age, height, weight and BMI were 34.8 ± 14.0 years, 162 ± 7.63 cm, 66.6 ± 13.8 kg and 25.1 ± 4.8 kg/m2, respectively. Table 1 shows the results of our descriptive analysis.
Discussion
Our findings indicate that at least 70% of participants did not possess means to measure their own height or weight, and approximately 80% had not measured their height or weight within the past year (Table 1). Moreover, approximately 60% did not know their own height or weight, and almost all participants (97.5%) did not have accurate knowledge (Table 1). Similar data trends were observed for all age groups (Table 1). These findings imply that community-dwelling people in WNBP currently have limited opportunities to measure their own height and weight and have a poor awareness of their respective measurements. Such information means that MRSs cannot really be feasible or effective.
The present study has several limitations. First, an analysis of the definite correlation between accessibility of height- and weight-measurement tools and the awareness of one's height and weight was outside its scope. Second, the generalisability of our findings may be in question, especially as a bias may have been introduced by excluding non-English speaking persons. Further studies with nationally representative samples of people are required in order to deepen our knowledge on the subject.
Footnotes
Acknowledgements
The authors thank everyone who took part in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.