
Abstract
Subacute combined degeneration of the spinal cord is a typical clinical syndrome due to vitamin B12 deficiency, characterised by the involvement of the posterior column and corticospinal tracts. Occasionally, it may present with atypical features such as a sensory level and Lhermitte's sign, both traditionally considered to be a feature of compressive myelopathy. Spinal magnetic resonance imaging strongly augments the diagnosis by exhibiting changes in the posterior column in the form of a ‘dot’. We describe such a patient who responded to therapy.
Case report
A 37-year-old man, vegetarian by diet, reported a month's progressive ascending bilateral lower limb numbness and tingling below the fourth dorsal (D4) dermatome and Lhermitte's sign (an uncomfortable ‘electrical’ sensation that runs through the back and into the limbs, brought on by neck flexion). Examination revealed the onset of tingling on stimulation with touch or painful stimuli below the nipple level and diminished vibration sense below the T4 spinous process. The remaining neurological and systemic examination was normal. Routine blood tests revealed an anaemia (Hb = 94 g/L) with macrocytosis (mean corpuscular volume = 108 fL). The peripheral blood smear showed the presence of hypersegmented neutrophils. Spinal magnetic resonance imaging (MRI) exhibited dot-like hyperintensity involving the posterior columns on axial imaging with subtle posterior hyperintensity in the sagittal section (Figure 1). He had low B12 level (76 pg/mL; normal range = 180–914 pg/mL). Other investigations including renal, hepatic and thyroid function tests, vasculitis markers, HIV, HbsAg and anti-HCV serology were unremarkable. Visual evoked potential and nerve conduction studies were also normal. The patient was initiated on parenteral cyanocobalamin supplementation (1000 µg per week for eight weeks) followed by once per month. Serology for anti-parietal cell antibodies was positive. His sensory level dropped to the level of T10 after two weeks and resolved over the ensuing two months. However, mild positive residual sensory symptoms remained.
(a) T2-weighted MRI scan of the dorsal spine (sagittal section) shows subtle posterior cord signal change in the upper dorsal spinal cord. (b) MRI of the dorsal spine (axial section) shows the presence of paired dot-like hyperintensities in the posterior column suggestive of ‘dot’ sign. MRI, magnetic resonance imaging.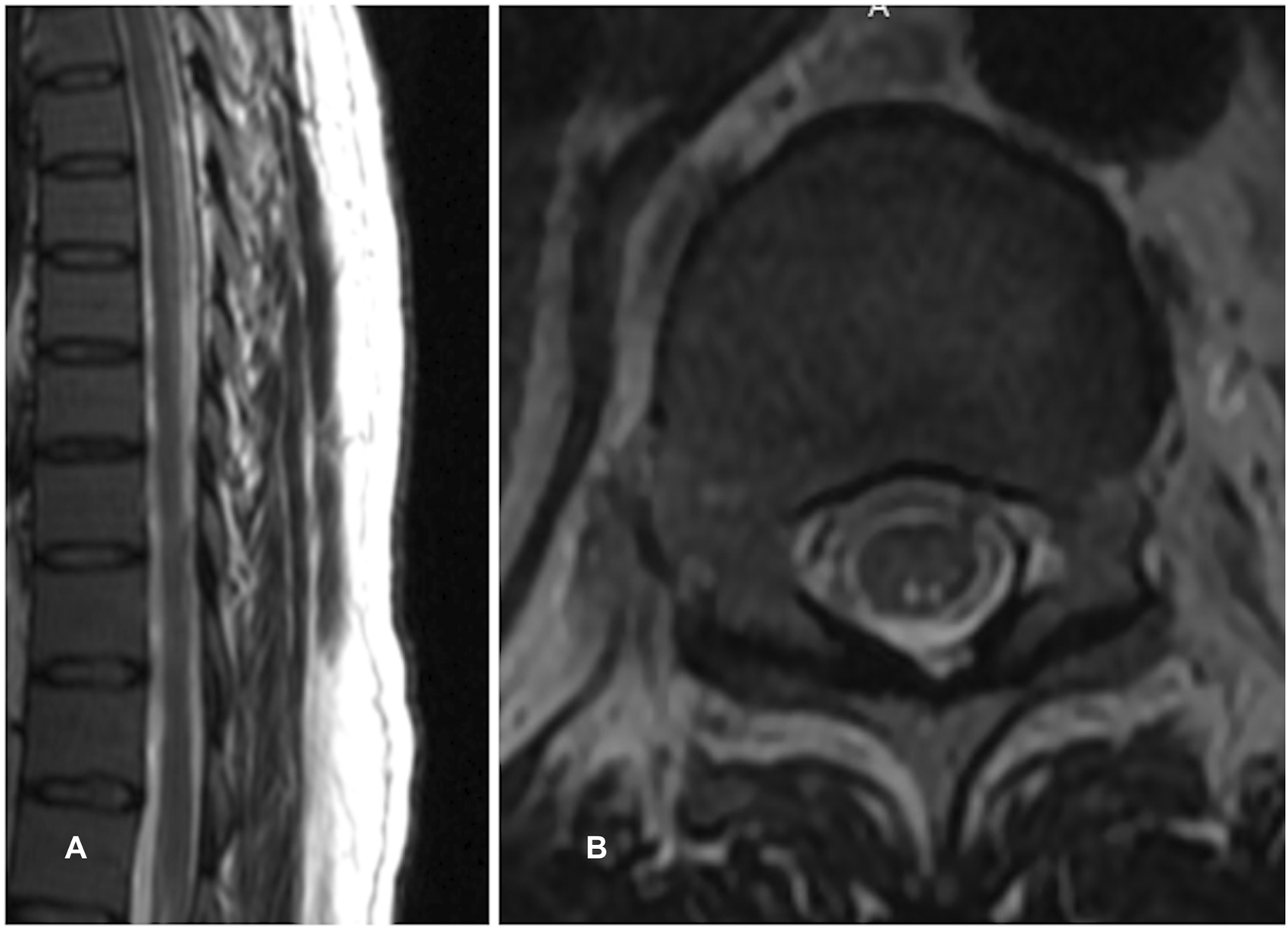
Discussion
SACD is a degenerative disorder affecting not only the white matter tracts in the spinal cord, but also the peripheral and, occasionally, the optic nerves. Usual clinical manifestations occur in the form of paraesthesia, spasticity, gait ataxia and peripheral neuropathy.
Our patient demonstrated a relatively uncommon clinical feature in the form of the presence of a sensory level. This may be an under-recognised feature. The presence of a sensory dermatomal level may impart prognostic value, with poorer recovery in those patients in whom it is present. 1
Another interesting feature was the presence of a reverse Lhermitte's sign (occurring on neck extension). Lhermitte's sign is reported in up to 21% of patients with SACD 2 and is usually an early feature.
Radiological features in SACD typically exhibit posterolateral signal change and are seen in 11%–37% of patients. 3 These may be the distinctive and prototypical ‘inverted V’ sign as well as the recently described ‘three-point’ sign.3 However, isolated posterior column hyperintensity in the form of ‘binocular sign’ and ‘dot’ sign on MRI have also been described, albeit less commonly. 4
It is important to note that SACD may present with atypical clinical features. In view of its mostly reversible nature, this possibility must be considered in all patients who present with sensory abnormalities in association with predominantly posterior column changes. A sensory level must be carefully explored in view of its potential prognostic implications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.