
Abstract
One of the latest diagnoses that need to be considered when evaluating patients with persistent headache is spontaneous (postural) intracranial hypotension (SIH). The diagnosis can be clinched by magnetic resonance imaging (MRI) findings of subdural collections, meningeal enhancement and tonsillar descent. Cerebrospinal fluid leak has been postulated as the cause, and both medical and surgical treatment options have been documented. The treatment of choice is, however, an epidural blood patch. Here we discuss two cases of SIH treated successfully with epidural blood patch.
Keywords
Introduction
Spontaneous intracranial hypotension (SIH) is characterised by the classic triad of orthostatic headache, low cerebrospinal fluid (CSF) pressure and magnetic resonance imaging (MRI) findings of meningeal enhancement, subdural collections, enhancing pachymeninges and tonsillar descent.1,2 Its aetiology and pathophysiology still need to be fully evaluated.2,3 The commonest radiological findings are subdural fluid collections, enhancement of pachymeninges, engorgement of venous structures, pituitary hyperaemia and sagging of the brain. 3 An epidural blood patch (EBP) is considered the treatment of choice once conservative management fails.4,5 We describe two cases of SIH successfully treated in this way.
Ethical consideration
Our report was prepared in consideration with the Institutional Ethical Committee (IEC-NI/08/Dec/07/44) of Sri Ramachandra Institute of Higher Education and Research (SRIHER), Chennai, India, based on the Indian Council of Medical Research (ICMR) guidelines of biomedical research in human beings. Informed consent was obtained from the participants and their legal guardians with the option to withdraw from the publication study at any time.
Clinical presentation
Case 1
A 40-year-old woman, with no known co-morbidity, presented with complaints of sudden onset of intermittent headache, increasing on getting up from a sitting position for the past 20 days. She had associated vomiting with no blurring of vision and no seizures. There was no associated history of trauma or fever. Her general physical examination was within normal limits. Her blood pressure was 140/80 mmHg in the sitting position. Fundus examination of both the eyes revealed no papilledema. No localising neurological signs were noted.
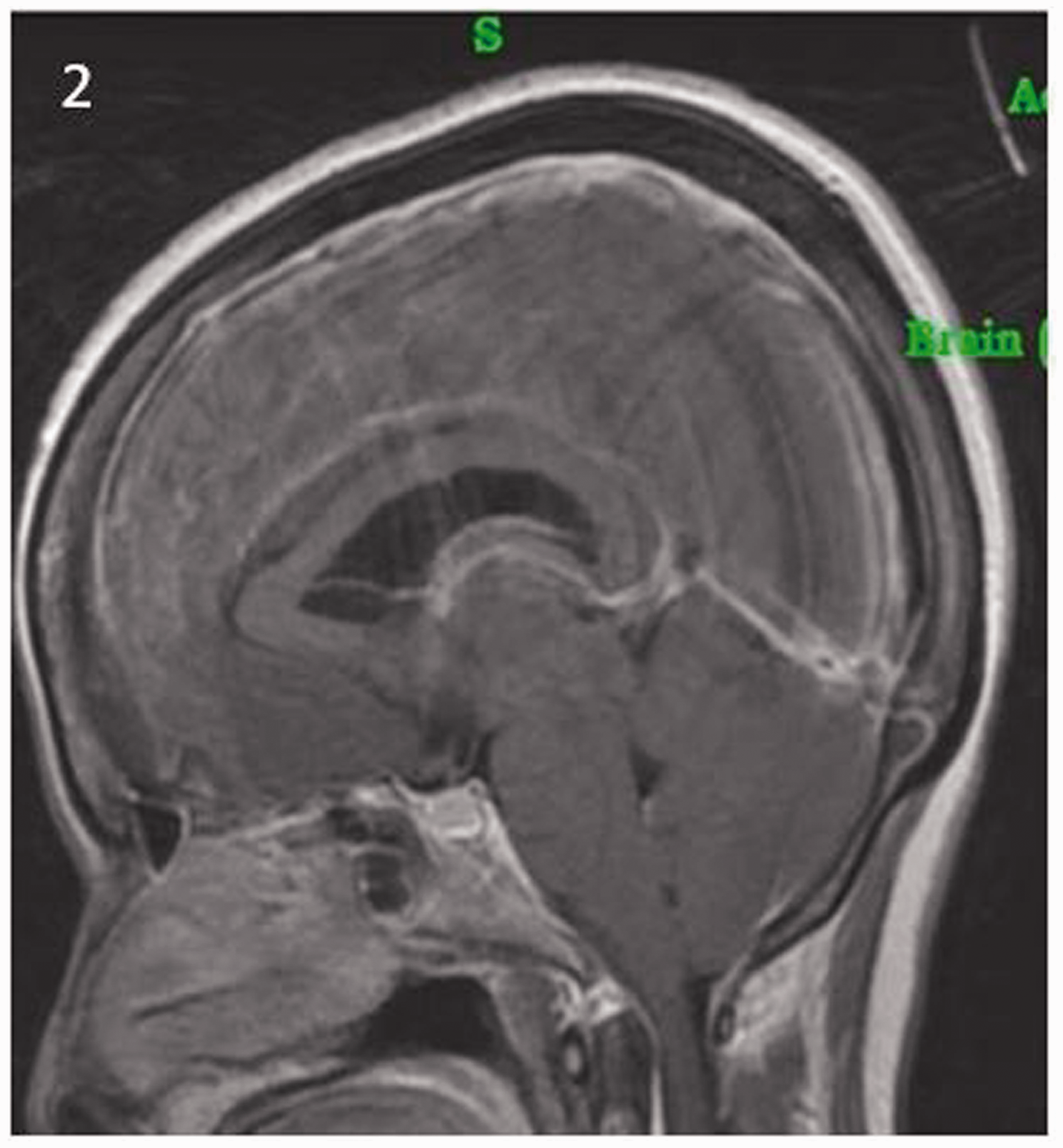
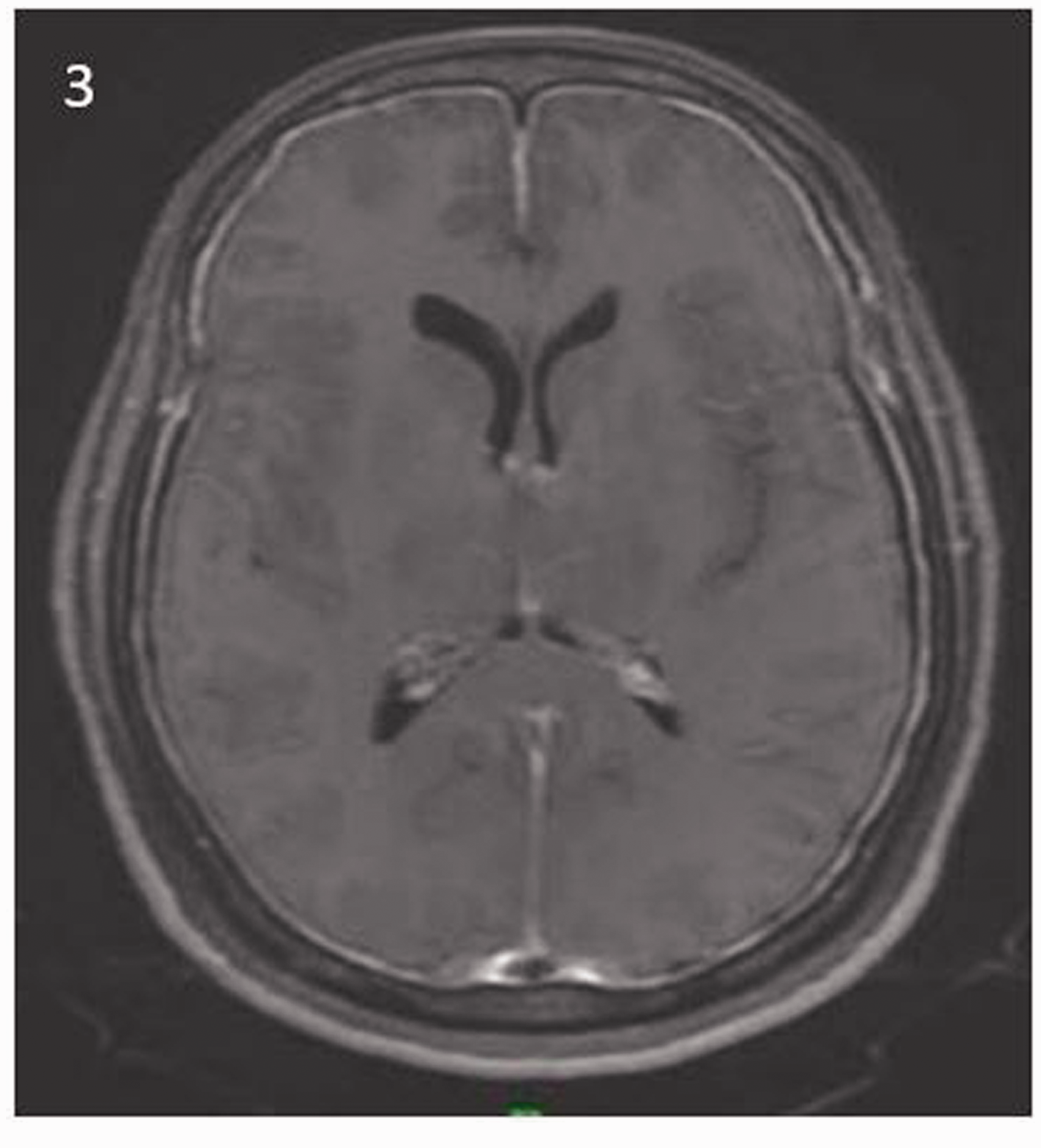
An MRI brain scan showed bilateral symmetrical subdural effusions over both cerebral hemispheres predominantly in the frontoparietal regions (Figure 1), effacement of perimesencephalic and prepontine cisterns, with an elongated and compressed midbrain (Figure 2), with tonsillar descent of 3.5 mm. Upon contrast administration, diffuse dural thickening and enhancement was noted (Figure 3). Based on these findings, a diagnosis of SIH was made. A ‘patch’ of 20 mL of autologous blood was placed in the L4-L5 epidural space under local anaesthesia.
MRI of the brain shows bilateral symmetrical subdural effusion over cerebral hemispheres. MRI of the brain showing tonsillar descent of about 3.5 mm. Diffuse dural thickening with contrast enhancement is noted.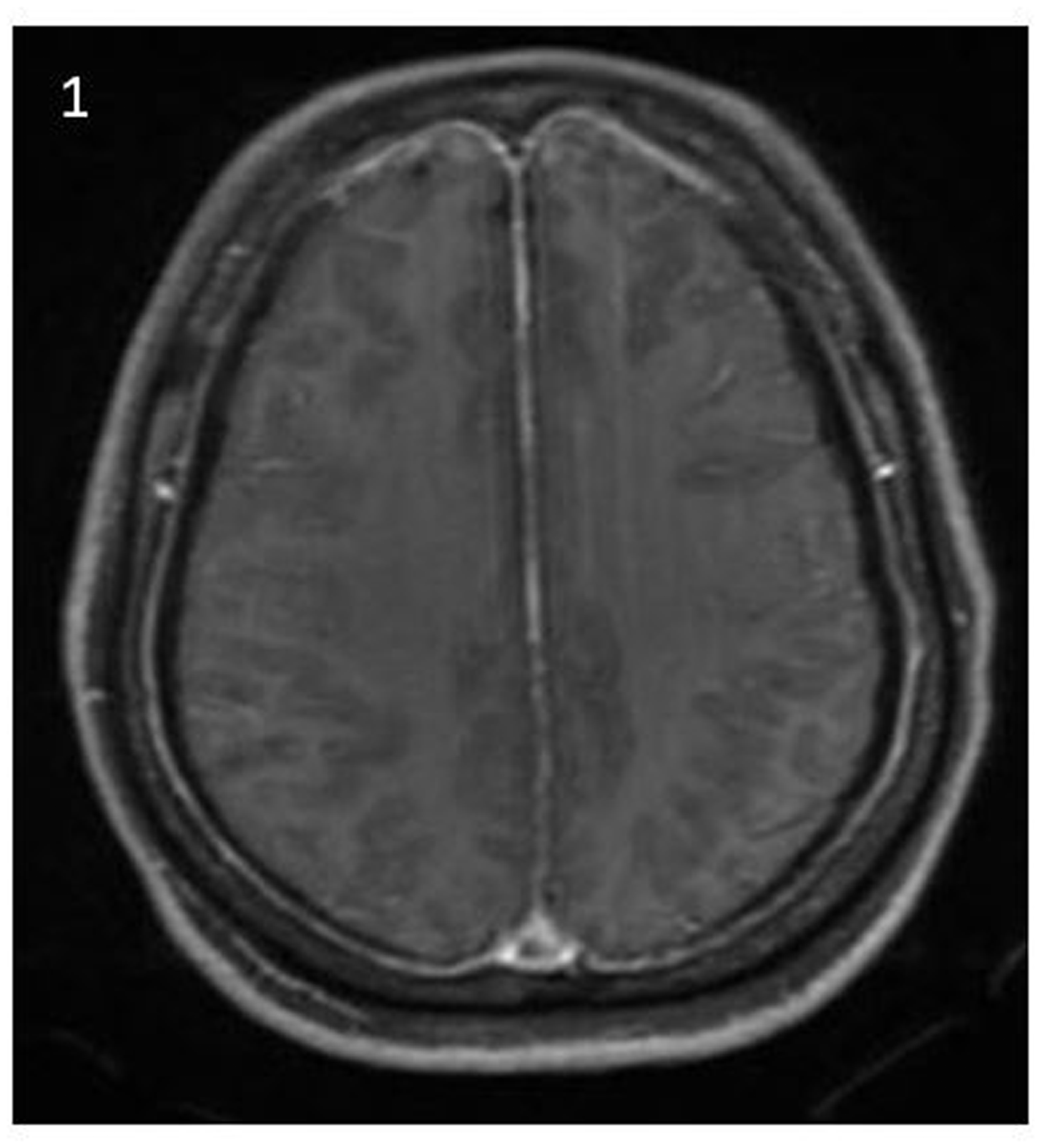
Two days after the procedure, the headache had disappeared and patient continues to be symptom-free after two years with follow-up scans showing total resolution of the subdural collection and sagging of the brain.
Case 2
A 35-year-old man with no co-morbidity presented with two months history of sudden onset, intermittent throbbing bilateral frontal headache, worse on standing upright. The headache was not associated with nausea, vomiting, blurring of vision or seizures. There was no history of recent trauma or fever. His general physical examination was within normal limits, with no focal neurological deficit. Blood pressure in the sitting position was 130/70 mmHg. Bilateral fundus examination showed no papilledema.
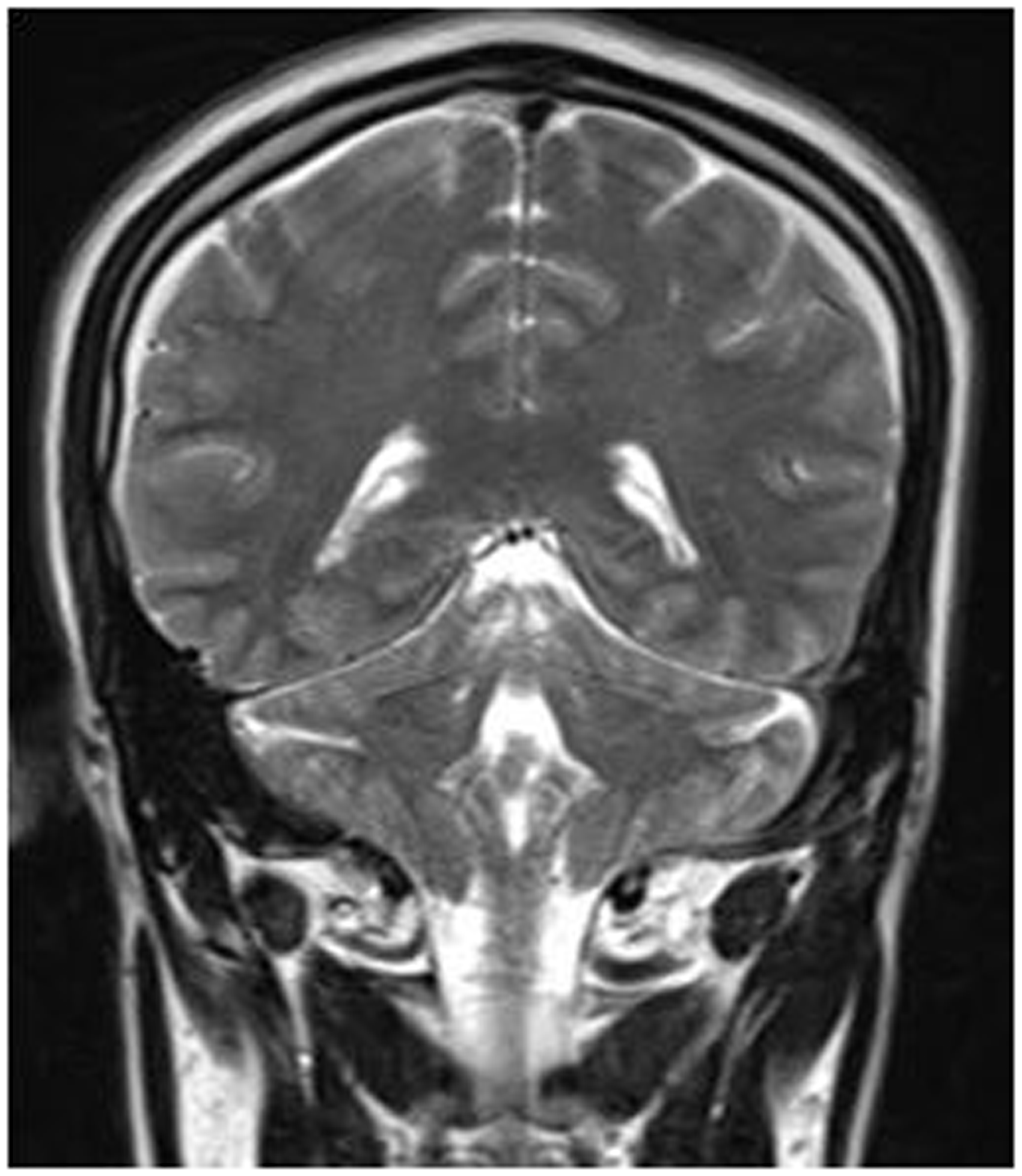
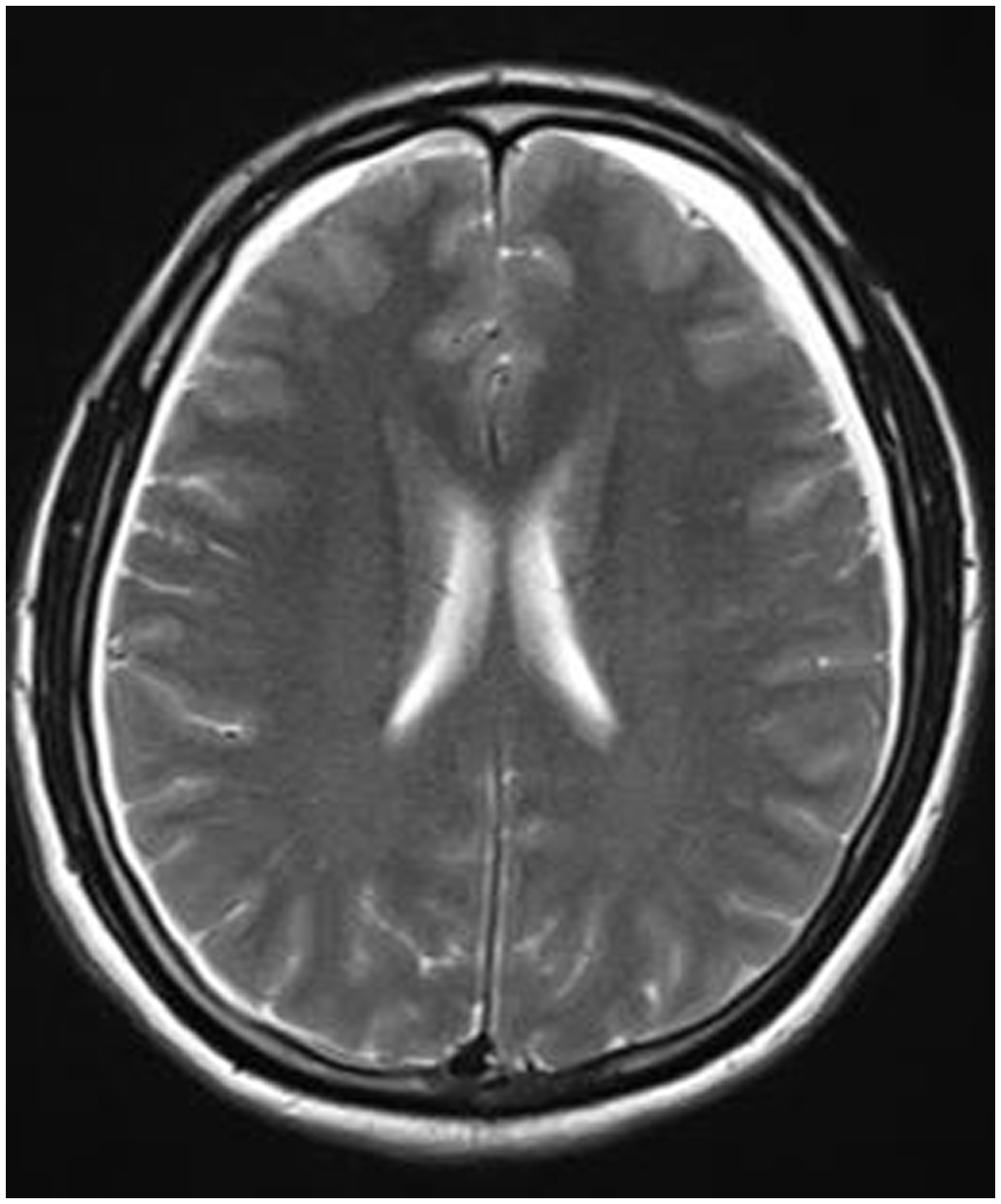
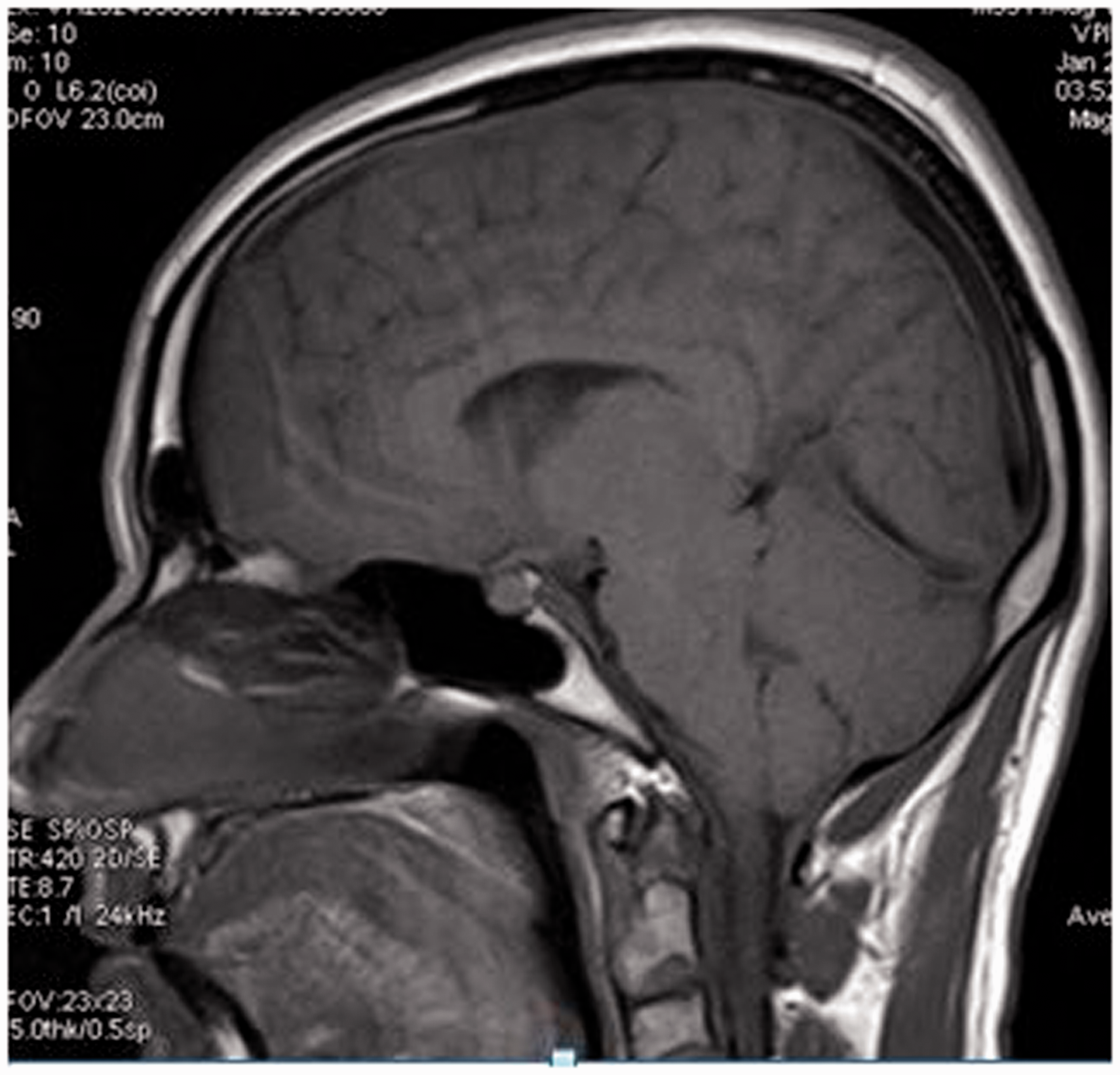
Cranial imaging showed bilateral frontoparietal subdural hygroma with diffuse cerebral oedema (Figures 4–6) and tonsillar descent of 10 mm below the foramen magnum (Figure 7). All routine blood investigations were normal.
T1 sagittal image showing subdural collection. T2-weighted coronal image shows bilateral subdural fluid collection. T2-weighted axial image shows bilateral subdural fluid collection. Sagittal image showing tonsillar ectopia of 10 mm below foramen magnum.
A diagnosis of SIH was made and the patient was treated in the same way as in Case 1. The headache disappeared and he could be discharged the very next day. No headache or any other fresh complaints were found at the one-year follow-up with resolution of the abnormal features present in the pre-procedural scan.
Discussion
Characteristic MRI findings of SIH make its diagnosis straightforward.6–9 Common presentation may be with associated dizziness, behavioural disturbance, vomiting and altered sensorium.10,11 A high index of suspicion of SIH is required in all patients with orthostatic symptoms, particularly in young and middle-aged patients with new-onset, persistent daily headaches. Typically, the symptoms occur immediately or within seconds to minutes of assuming an upright position and resolve within minutes after lying supine. 7 Nevertheless, a delayed response to postural change, after minutes or hours, may occur. SIH needs to be differentiated from the pathophysiologically similar post-lumbar puncture headache, as well as orthostatic headache due to postoperative CSF leakage or shunt over-drainage where there is an obvious trigger. 12
The estimated incidence of SIH is 5 per 100,000 inhabitants, 10 though the real figure might be significantly higher. Women are twice as likely to be affected than men. 13
Most CSF leaks occur at the thoracic or cervicothoracic junction. An underlying connective tissue disorder may play a role. Other potential contributing factors are minor trauma, degenerative disc disease and osseous spurs. Usually, the leaks themselves do not provoke any local symptoms. 14 Owing to the CSF leakage, a hypovolemia results in sagging of the brain and consequent tension in pain-sensitive structures such as veins and the duramater. In close to 70% of cases, the site of the leak is not evident, possibly because it may be transient, or the resolution thresholds of the scans are inadequate to identify small leaks and low intrathecal pressures. 15
No specific management guidelines have been established.14,15 Once the diagnosis has been made, a blind or targeted lumbar EBP is the cornerstone of treatment. 8 This should be followed by 12–24 h of bed rest in a horizontal or Trendelenburg position. 15 The mechanism by which the EBP works is not known. It probably forms a dural tamponade, thereby sealing the leak.
The injected blood has been shown to disseminate over several spinal levels, sometimes up to the cervical spine. The success rate of an EBP is in the range of 58%–77% and it can easily be repeated several times.14,15 Many patients benefit from repeated blood patches, which sometimes have a cumulative effect.1,15,16 Usually, the effect of EBP begins immediately after the procedure.
As a pragmatic approach, and depending on the severity of the symptoms, at least 1–3 EBPs should be applied in patients with persistent symptoms before further diagnostic testing to localise the precise site of leakage. An alternative treatment strategy to that of EBP is the injection of fibrin glue at the site of the leak.
Footnotes
Acknowledgements
The authors acknowledge the support and help provided by SRIHER, Chennai, India (IEC-NI/08/Dec/07/44).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.