
Abstract
One of the rare complications of cholelithiasis is gallstone ileus which occurs in <5% of patients. Among them, <3% develop Bouveret’s syndrome: gastric outlet obstruction by a large gallstone in the pylorus or duodenum. One large review of 128 patients showed it to present at a mean age of 74.1 ± 11.1 years with a mean gallstone size of 4.6 ± 1.5 cm, with nausea or vomiting in 86%, abdominal pain in 71% and haematemesis in 15%. The diagnosis is usually clear on oesophagogastroduodenoscopy or abdominal contrast-enhanced computed tomography. We present a case with massive upper gastrointestinal bleeding, due to erosion of a cystic artery pseudoaneurysm.
Case report
A 63-year-old man, with a previous coronary artery bypass graft and diabetes mellitus taking low-dose aspirin, presented with a three-day history of right hypochondrial pain and haematemesis requiring transfusion of 6 units of blood. An OGD had shown a small fistulous opening in the first part of the duodenum (D1) with a mild ooze of fresh blood appearing at the papillary orifice. A CT angiogram had shown a cystic artery pseudoaneurysm 4 × 4 mm in size which was coiled. Two days later, he developed post-prandial vomiting. A second OGD now showed a large stone completely obstructing the D1 with a fistulous communication to the gallbladder. Endoscopic retrieval of the stone was impossible on account of its size.
At this stage, the patient’s vital signs were stable and routine laboratory investigation were normal. A second abdominal CT scan revealed a large stone in the D1 with a fistulous communication between the D1 and the gallbladder, a dilated stomach, pneumobilia and previously placed coil was visualised (Figure 1a and 1b). OGD in our unit showed a large stone in the D1 with fistulous tract and visible stone in the gallbladder (Figure 1c, black arrow). Urgent surgical intervention was advised. Intraoperatively there was perforation of gallbladder fundus and a fistulous communication between it and D1 (i.e. endoscopic findings were confirmed). On duodenotomy, two large gallstones 5 × 3 × 3 cm and 2 × 2 × 2 cm in size (Figure 1d–f) were found and removed. Subtotal cholecystectomy was performed along with primary repair of the fistula site. The postoperative course was uneventful and the patient was discharged after one week.
(a, b) Coronal computed tomography image with a large stone in the D1 and a fistula between the D1 and the gallbladder, hugely dilated stomach and pneumobilia (a, black arrow). Coil artifact is also seen in the gallbladder fossa (b, black arrow). (c) Endoscopy image showing impacted stone in the D1 with large fistula and another stone seen through the opening. (d, e) Intraoperative image of stones being removed from the duodenotomy. (f) Measure of the stone size.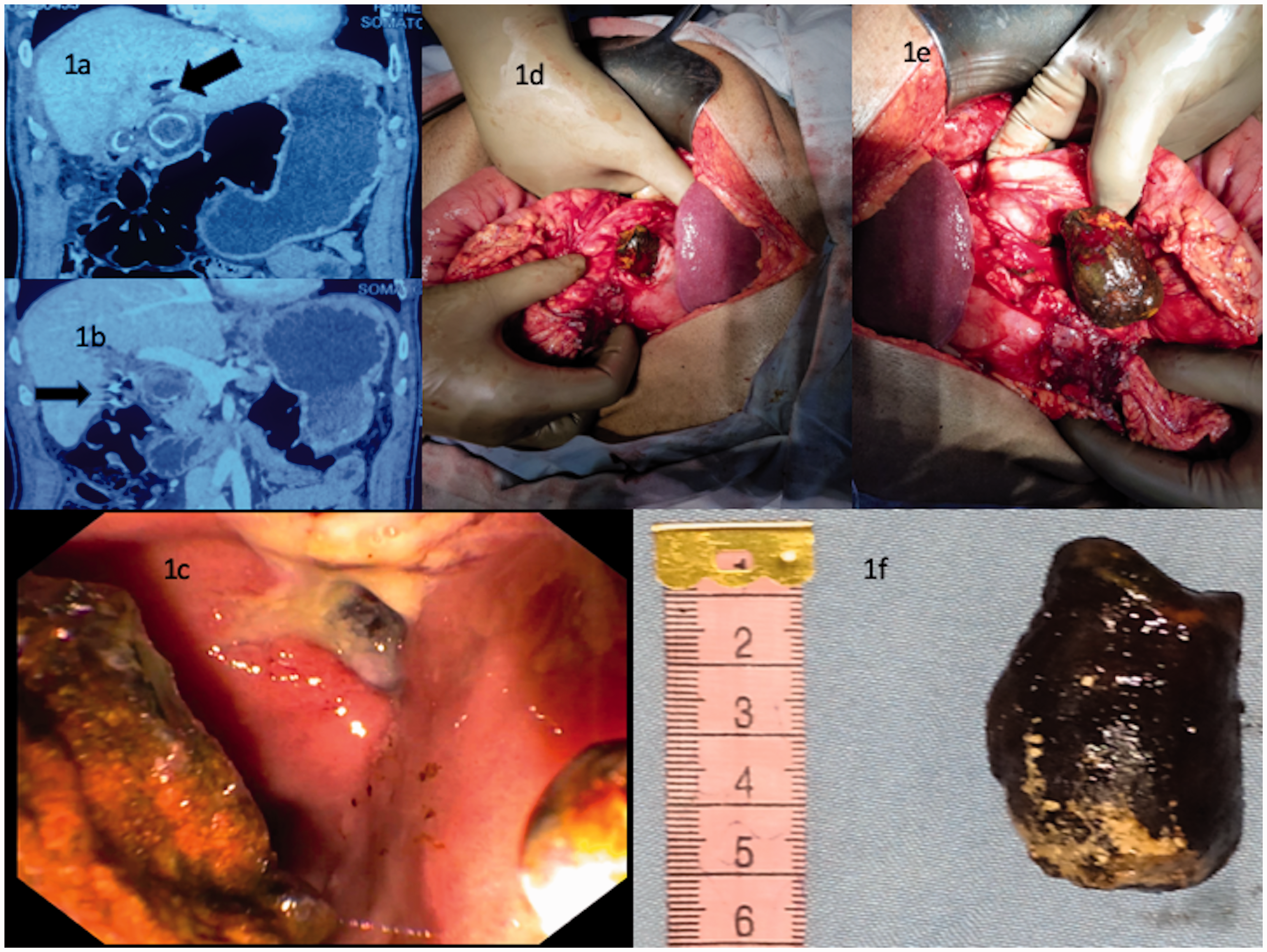
Discussion
Massive hematemesis requiring multiple blood transfusion in Bouveret’s syndrome is usually from a gastric or duodenal ulcer, either through pressure necrosis or peptic effects1,2 but very rarely from the cystic artery. 3 Due to its rarity, the exact frequency of cystic artery pseudoaneurysm is unclear. Fujimoto et al. 4 reviewed the largest number of cases of cystic artery pseudoaneurysm with acute cholecystitis: 43/50 (86%) cases had ruptured before diagnosis. Our case of bleeding from a cystic artery pseudoaneurysm may be unique. Clearly, this needs dealing with first, if possible, by intravascular coil insertion. Endoscopic removal of the stone is usually successful if it is of medium size and mobile; lithotripsy may be helpful to assist in removal. There remains the risk of stone impaction in the oesophagus on retrieval or its fragmentation causing obstruction in the distal ileum. Large, multiple or impacted stones need surgical intervention, 5 as does a large fistula.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.