
Abstract
Acute thoracic aortic dissection is an uncommon, although not rare, life-threatening condition. With protean signs and symptoms that often suggest more common cardiac or pulmonary conditions, it can be difficult to diagnose. Ultrasound has proven useful in making the correct diagnosis. This case demonstrates that training gained using standard ultrasound machines can be easily and successfully adapted to newer handheld ultrasound devices. The examination technique using the handheld device is illustrated with photos and a video.
Keywords
Introduction
Rapid diagnosis helps reduce mortality and physician-performed point-of-care ultrasound (POCUS) is the most rapid, cost-effective method of screening for this disorder.
Portable ultrasound machines have progressively become smaller while incorporating many functions found in larger units. A variety of these devices with diverse sizes, complexity and cost exists. At least one handheld device uses electronics to eliminate the need to change probes for different examinations and ultrasound depths. It has often been assumed that standard ultrasound skills transfer directly to handheld devices, but this has not been demonstrated. In this case, an emergency physician with ultrasound experience who had never used this or any handheld ultrasound device previously, was able to diagnose an acute thoracic aortic dissection in an emergency patient with non-specific complaints but a suggestive chest radiograph.
We provide a review of the diverse symptomatology and physical findings associated with acute aortic dissection (AAD) and describe the handheld ultrasound device and the technique to visualise this pathology.
Case report
A 75-year-old man of East Indian descent presented to the Georgetown Guyana Public Hospital emergency department complaining of one week of chest and abdominal pain, for which he was taking paracetamol. He had no significant past medical history, had stopped smoking more than five years previously and drank alcohol occasionally. His initial vital signs were equal pulses regular at 94 bpm, a blood pressure of 145/100 mmHg, temperature of 35.7°C, SpO2 99% (on room air) and unlaboured respirations at 22 per minute. His Glasgow Coma Scale score was 15/15. Suspecting an acute coronary syndrome, he was given 325 mg aspirin to chew.
His physical examination demonstrated only mild periumbilical and suprapubic tenderness. Auscultation of the heart and lungs were normal. Suspecting an acute coronary syndrome but needing evaluation for abdominal pain, he received 500 mL normal saline and 50 mg ranitidine orally. Laboratory tests, ECG (non-specific ST-T changes) and a chest radiograph (Figure 1) were ordered. Shortly thereafter, the patient reported feeling better.
Posteroanterior chest radiograph showing an enlarged cardiac silhouette with a large, well-defined opacity involving the superior mediastinum and left perihilar region (⋆). The thoracic aorta is dilated, and the trachea is displaced toward the right. While the lungs are clear, there is a homogenous opacification in the left subpulmonic area suggesting effusion (⋄).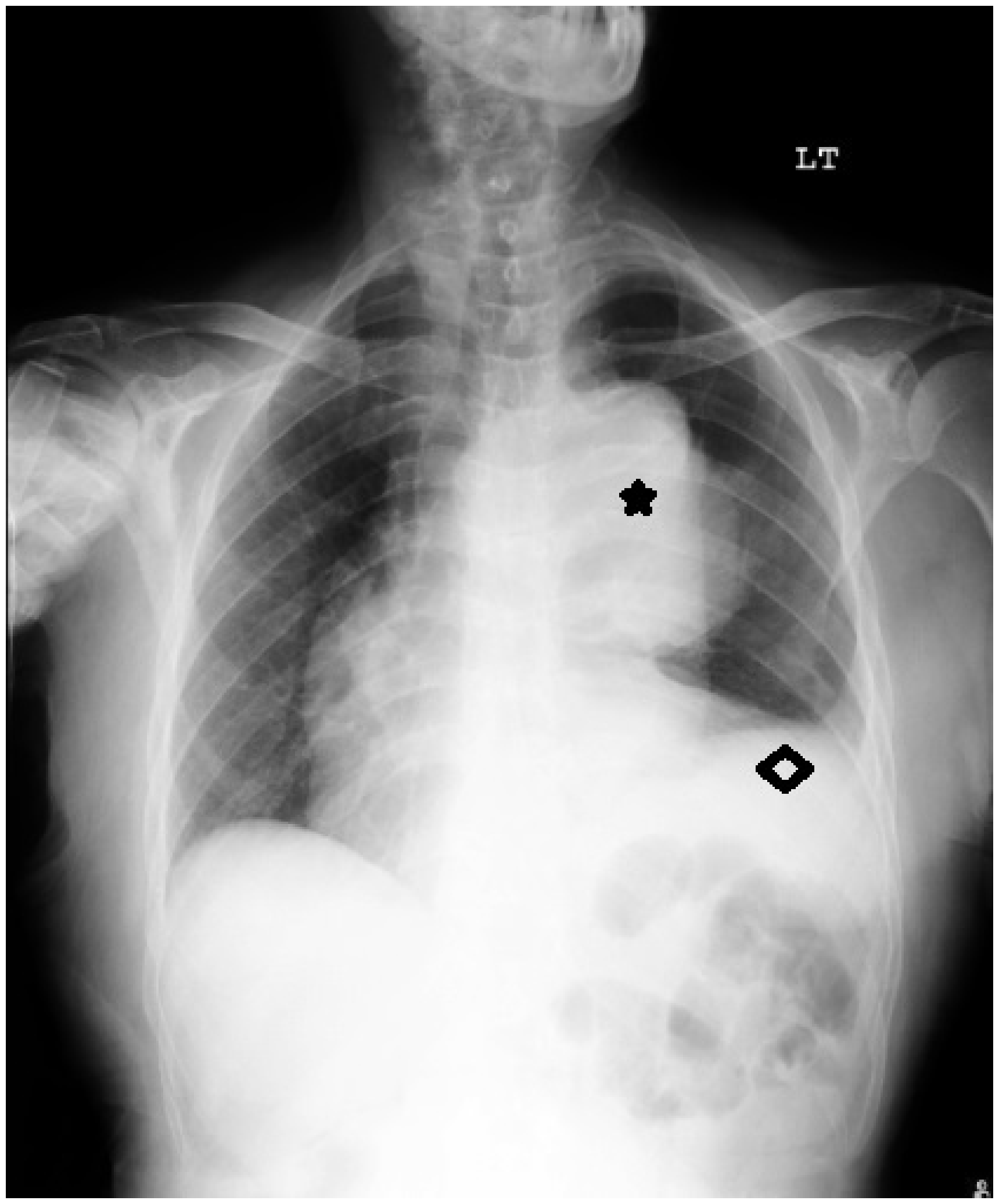
His laboratory results, including troponin I, were normal, except for a slightly elevated urea of 15 mmol/L and creatinine of 230 umol/L. D-dimer testing was not available.
Concerned by appearances on the chest radiograph, the physician performed a bedside transthoracic and abdominal ultrasound examination to define the mediastinal mass better. She had never previously used the recently donated handheld probe (Butterfly IQ®, Guilford, CT, USA) to detect AAD. Using the device’s cardiac setting, she examined the parasternal long axis view of the heart. This showed moderate left ventricular systolic function, a normal thoracic aortic outflow track and a small pericardial effusion. The descending thoracic aorta was of normal diameter. Further scanning of the anterior chest at the level of the second intercostal space demonstrated an ascending thoracic aortic aneurysm measuring 9.5 cm with a dissecting intimal flap (Video; Figure 2). The abdominal aorta had normal measurements.
Thoracic aortic aneurysm with flap dissection (see video).
Since there is no ability in Guyana, a low-income country, to perform thoracic aortic surgery, the patient, duly diagnosed with a type A AAD, was admitted to our internal medicine service for standard non-surgical management. This treatment, designed to control the heart rate and blood pressure, included intravenous labetalol and a titrated nitroglycerin infusion. The target blood pressure was 140/90 mmHg. Nitroglycerin was used owing to the lack of nitroprusside and infusion pumps.
Nonetheless, our patient died several hours later and an autopsy confirmed the ultrasound findings.
Discussion
Aortic dissection occurs when blood dissects between the intimal and adventitial layers of an artery. The disorder is uncommon, with an annual age- and sex-adjusted incidence reported as 3.5 per 100,000 persons. (Aortic rupture, a different entity, has the same incidence. 1 ) The disorder is life-threatening, with approximately 20% of patients dying before reaching hospital.
AADs are usually classified using the Stanford system, with any dissection involving the ascending aorta being type A and all others type B. Type A dissections have the highest mortality and are generally treated surgically; type B is most often treated medically. 2 Both require aggressive treatment of blood pressure and heart rate to decrease shear stress on the aorta wall. 3 For every hour delay in type A AAD diagnosis and treatment, the mortality rate is 1%– 3%/h during the first 24 h, 30% at one week, 80% at two weeks and 90% at one year. The hospital mortality rate for treated patients is approximately 30%. 4 Overall type B in-hospital mortality is 13%. 2
Diagnosing AAD can be challenging, since the presenting signs and symptoms often mimic other more common disorders. While patients with AAD classically present with sudden severe, sharp or tearing chest pain radiating to the upper back,5,6 6%–15% of patients may present with minimal symptoms, as did our patient. These less symptomatic patients have a higher-than-normal mortality, usually owing to delayed diagnosis and surgery.6–8 This includes almost one-third of patients aged >70 years, in which typical dissection presentations are less common. 8 the presentation of patients may also be confusing when they have had or seem to have an associated myocardial infarction, cerebrovascular accident, renal, spinal cord, or bowel ischemia or infarction. 9
The large International Registry of Acute Aortic Dissection (IRAD) database found a median time from emergency hospital admission to diagnosis of 4.3 h. While critically ill patients (e.g. those with hypotension, tamponade, pulse deficits/limb ischemia or altered mental status) are diagnosed earlier, studies show that longer delays more commonly occur in women, those presenting with atypical, gradual-onset or painless symptoms,6,10 patients with prior cardiac surgery 11 or those seen at a non-tertiary care hospital. 12
High risk conditions, pain features, and exam features to identify AAD. 10
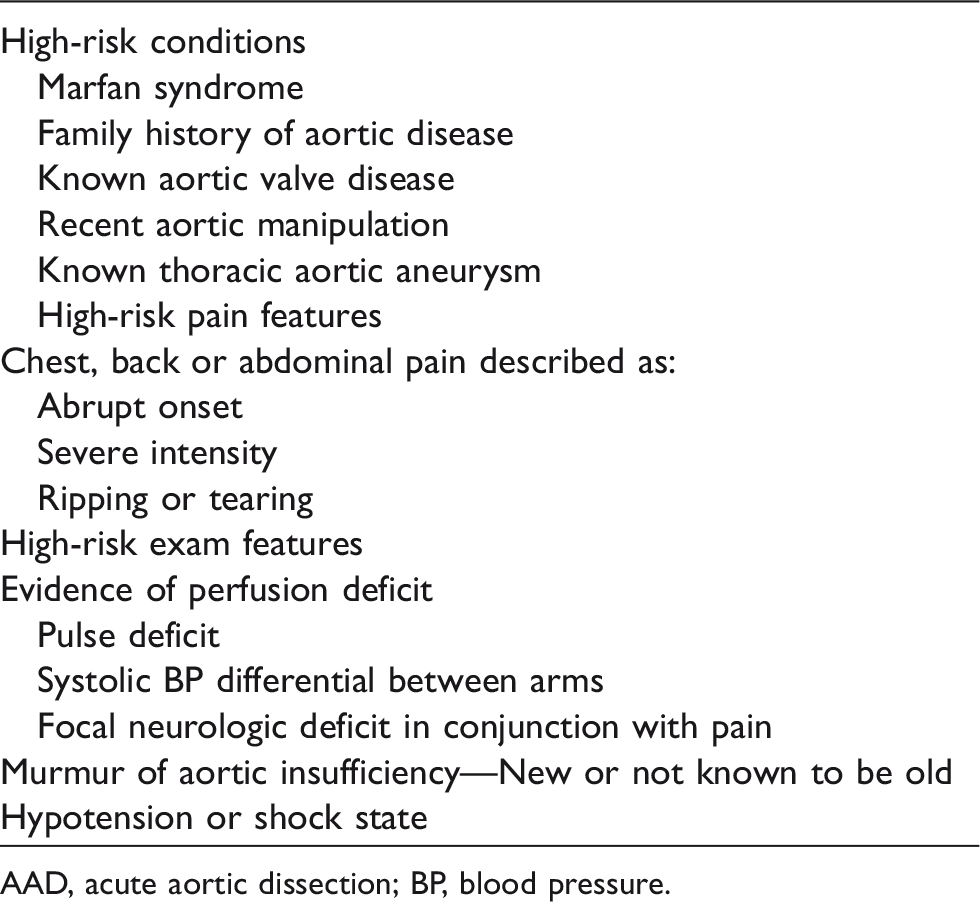
AAD, acute aortic dissection; BP, blood pressure.
With a suspicion of AAD, immediate imaging is necessary. Physicians often use the chest radiograph to screen patients for an AAD, although a normal study is relatively common in these patients.5,16,17 While a chest radiograph was not initially included in the AAD-RS criteria, subsequent validation analysis concluded that it was necessary to identify AAD in some patients that the scoring system rated as low risk. As in the patient we described, non-specific signs and symptoms steered the clinician away from considering an AAD until the chest radiograph was obtained. Yet, as opposed to POCUS that has a sensitivity for identifying AAD-associated abnormalities of 88%–99%, the radiographic sensitivity is low: left-sided pleural effusion (19%); pericardial effusion/tamponade/enlarged cardiac silhouette (26%); wide mediastinum (49%–67%); and intramural haematoma thrombus (49%–63%). In addition, unlike POCUS, simple radiography cannot identify an intimal flap or wall motion abnormality. 9
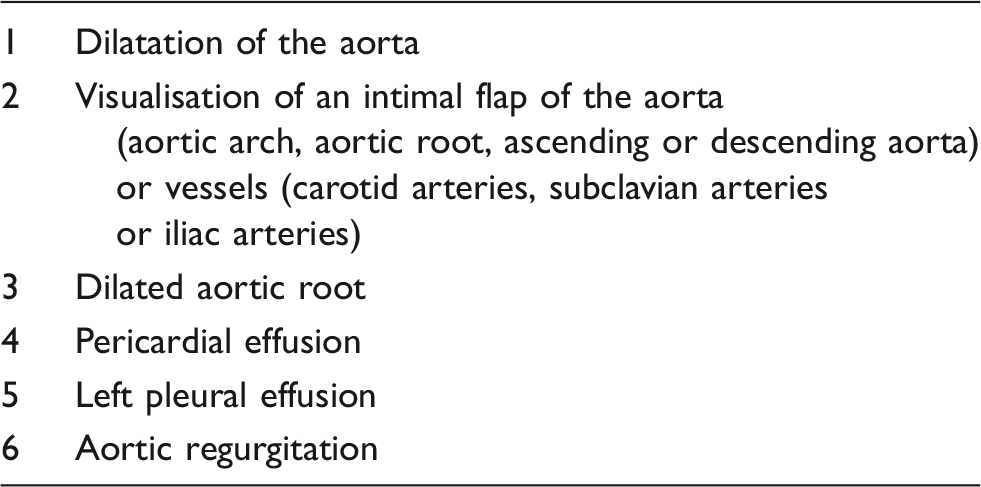
Acute aortic dissection findings on ultrasound.
However, other than POCUS, the substantial logistics involved in transporting a potentially unstable patient, summoning specialised personnel, preparation and study interpretation limit their usefulness and may significantly delay diagnosis and treatment.2,5,18
Several cases of emergency-diagnosed ADD using ultrasound have been reported, although none reported using a handheld device.3,19,20 A recently released handheld ultrasound (Butterfly iQ®, Guilford, CT, USA) was used in this case. Within a single handheld unit, it contains multiple presets emulating various transducers, functions in B-, M-, and colour Doppler modes. The device’s single probe, with a range of 1–5 MHZ, emulates a linear, curved or phased probe. 21 The device also supports encrypted wireless data transmission to iOS devices.
There are inherent limitations to any of the available handheld devices and POCUS. Not only are the prices for these devices often prohibitive for practitioners and institutions in lower-income countries, but unlike larger machines, they can easily be damaged, misplaced or purloined. Some only function with iOS devices, and the smartphone, tablet or laptop that receives their signal is a separate cost. POCUS at any site, but particularly with rarely used examinations, is limited by sonographer skill and experience, sonographic artifacts, and patient-centred challenges such as body habitus, bowel gas and overall cooperation.19,22 In addition, portions of the thoracic aorta cannot be visualised by POCUS and evaluation of intimal flap extension into smaller arteries is limited. However, physicians who have access to these devices can quickly diagnose and document life-threatening conditions, including ADD.
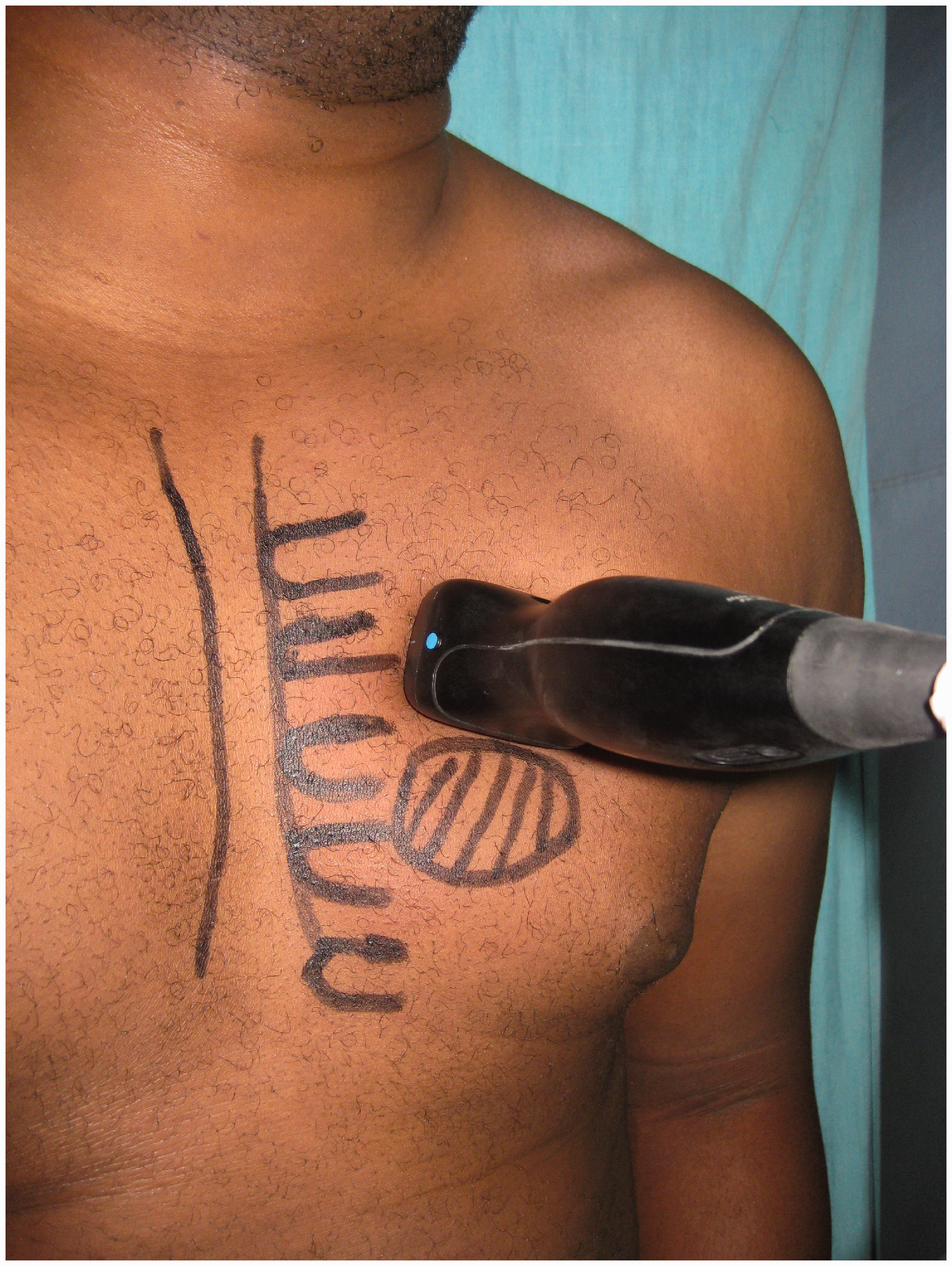
Ultrasound to diagnose an AAD is straightforward using standard cardiac views. Figure 3 shows the positions for the probe in the long parasternal cardiac view (diagonal stripes) and to view the aortic arch in the second intercostal space (cross-hatched). Figure 4 shows the handheld ultrasound in position to image the aortic arch.
Positions for the probe in the long parasternal cardiac view (diagonal stripes) and to view the aortic arch in the second intercostal space (cross-hatched). Handheld ultrasound in position to image the aortic arch.
Nearly all patients (∼90%) diagnosed with a type A AAD are managed surgically. Most patients receiving medical treatment for type A AAD either refuse surgery or have unacceptable surgical risks. 23 Medical management includes heart rate and blood pressure control. With surgery, patients on international registers have a mortality rate of approximately 22%. Medical management results in a 57% mortality rate, a rate that has not changed over the past 25 years. 8
Conclusion
Any device that reliably can diagnose a life-threatening condition easily benefits patients. POCUS, including with handheld devices, is easily performed, takes much less time and is more readily available in less-developed regions than are CT angiography, MRI or TEE. The technique to identify thoracic AAD is a slight modification of the standard cardiac examination.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.