
Abstract
Liver abscess in early infancy is uncommon, needs a high index of suspicion for diagnosis and carries a high mortality. It presents most frequently by a fulminant course, generalised sepsis and multiple metastatic abscesses. An underlying predisposing factor is usually attributed in nearly all cases reported to date. These include prematurity, low birth weight, umbilical catheterisation (UC), administration of hypertonic dextrose or total parenteral nutrition via UC, exchange transfusion, blood culture proven sepsis, necrotising enterocolitis, antecedent abdominal surgery, birth asphyxia, omphalitis and underlying immunodeficiency. We present three cases of early infantile liver abscesses without any identifiable predisposing factor despite extensive work-up to search for such. Early recognition and management led to a favourable outcome in all our patients.
Materials and methods
A retrospective case-record review was carried out for all infants admitted and diagnosed with liver abscess between January and September 2019 at our tertiary care teaching hospital in Northern India. Written informed consent was obtained from the parents of enrolled patients at follow-up outpatient visits. Clinical, laboratory and radiological details were noted with evaluation of potential risk factors, treatment administered and outcomes attained.
Results
Comparison of the clinical, laboratory, radiological, treatment and outcome details of the three neonates with liver abscess.
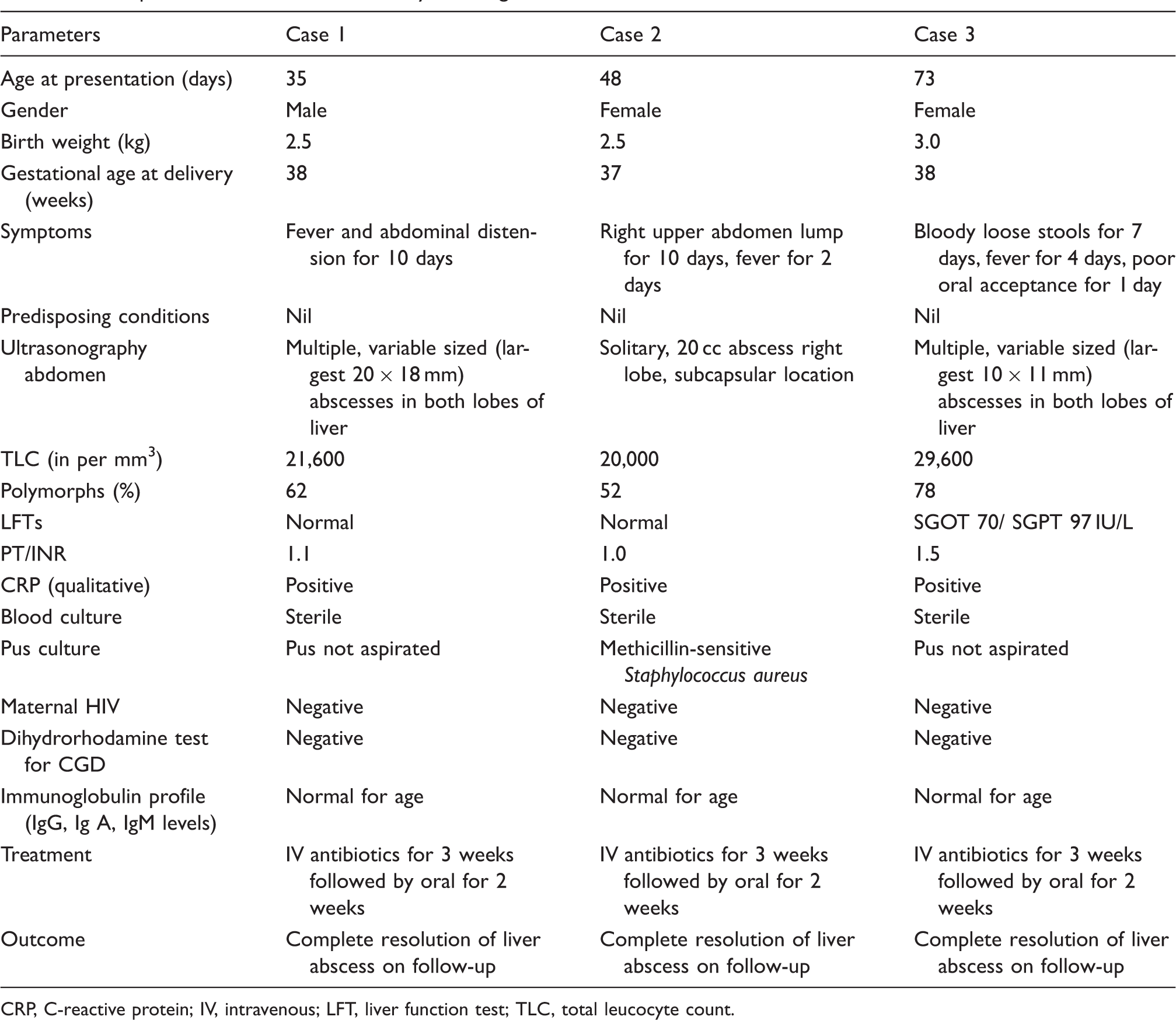
CRP, C-reactive protein; IV, intravenous; LFT, liver function test; TLC, total leucocyte count.
Case 1
A 37-day-old male infant presented with fever (up to 38.2℃) and abdomen distension of 10 days’ duration. On examination, he was active, alert, haemodynamically stable with an isolated hepatomegaly (the liver being palpable 4 cm below the costal margin with a span of 7.5 cm) and no other abnormal systemic findings. Ultrasonography revealed multiple abscesses in both hepatic lobes. Therapy with intravenous ceftriaxone and vancomycin was commenced, with defervescence after three days and decrease in abscess size seen on serial ultrasound scans.
Case 2
A 50-day-old female infant presented with a mass in the right upper abdomen of 10 days’ duration with fever (up to 38.6℃) for 48 h. On examination, she was playful, active and haemodynamically stable; abdominal examination revealed right hypochondrial tenderness with a visible mass 4 × 6 cm in size, presumed to be attached to the liver. Ultrasonography revealed a superficially situated solitary 20-mL subcapsular right lobe liver abscess. Image-guided percutaneous needle drainage was carried out; culture of pus obtained subsequently grew Methicillin-sensitive Staphylococcus aureus. Intravenous ceftriaxone and vancomycin were started as before, with reduction of fever within 48 h and a decrease in the size of the abscess on serial ultrasound scans.
Case 3
A female infant aged 2.5 months presented with bloody loose stools of seven days’ duration, decreased appetite and fever (up to 38.3℃) for four days. On examination, she was irritable and pale but haemodynamically stable with hepatomegaly palpable 6 cm below the costal margin, with a span of 8 cm. There was no splenomegaly and no other abnormal systemic findings were found. Ultrasonography revealed multiple liver abscesses involving both lobes. The same antibiotic regime was commenced, with a reduction of fever and loose stools within four days. Serial ultrasound scans monitored the resolution of the abscess.
Fever was thus present in all our cases, while hepatomegaly was found in two of the three cases. All patients had a leucocytosis of >20,000/mm 3 and a positive C-reactive protein (CRP) test. Liver function abnormality was present in only one of our cases; however, ultrasound was diagnostic in all.
All three of our patients responded to treatment and were well at the 12-months follow-up.
In view of the unusually early age of presentation without identifiable risk factors, investigations of maternal HIV serology, dihydrorhodamine assay for chronic granulomatous disease and immunoglobulin profiles (IgG, IgA, IgM) were carried out on all patients, but proved negative.
Discussion
Neonatal and early infantile hepatic abscess (first presentation at age <100 days) without any underlying risk factor has been reported in fewer than five infants to date.1–3 However, these cases1–3 had no search for underlying immunodeficiency undertaken, particularly CGD and HIV, both of which are known causes.4,5 Our case series highlights the possibility of the development of liver abscess in early infancy in term, exclusively breast-fed babies with normal birth weight, without any perinatal complications, nor risk factors for sepsis, nor underlying immunodeficiency. The infective organism can reach the liver via the portal circulation (umbilical vein, splenic vein, mesenteric vein), systemic circulation (hepatic artery) or via direct invasion from surrounding structures. 6,7 One case of transmission from infected breast milk has been described. 8 In our series, we believe the infection is likely to be blood-borne with occult bacteraemia as the cause.
Clinical presentation and lab investigations of early infantile (aged <100 days) liver abscess.
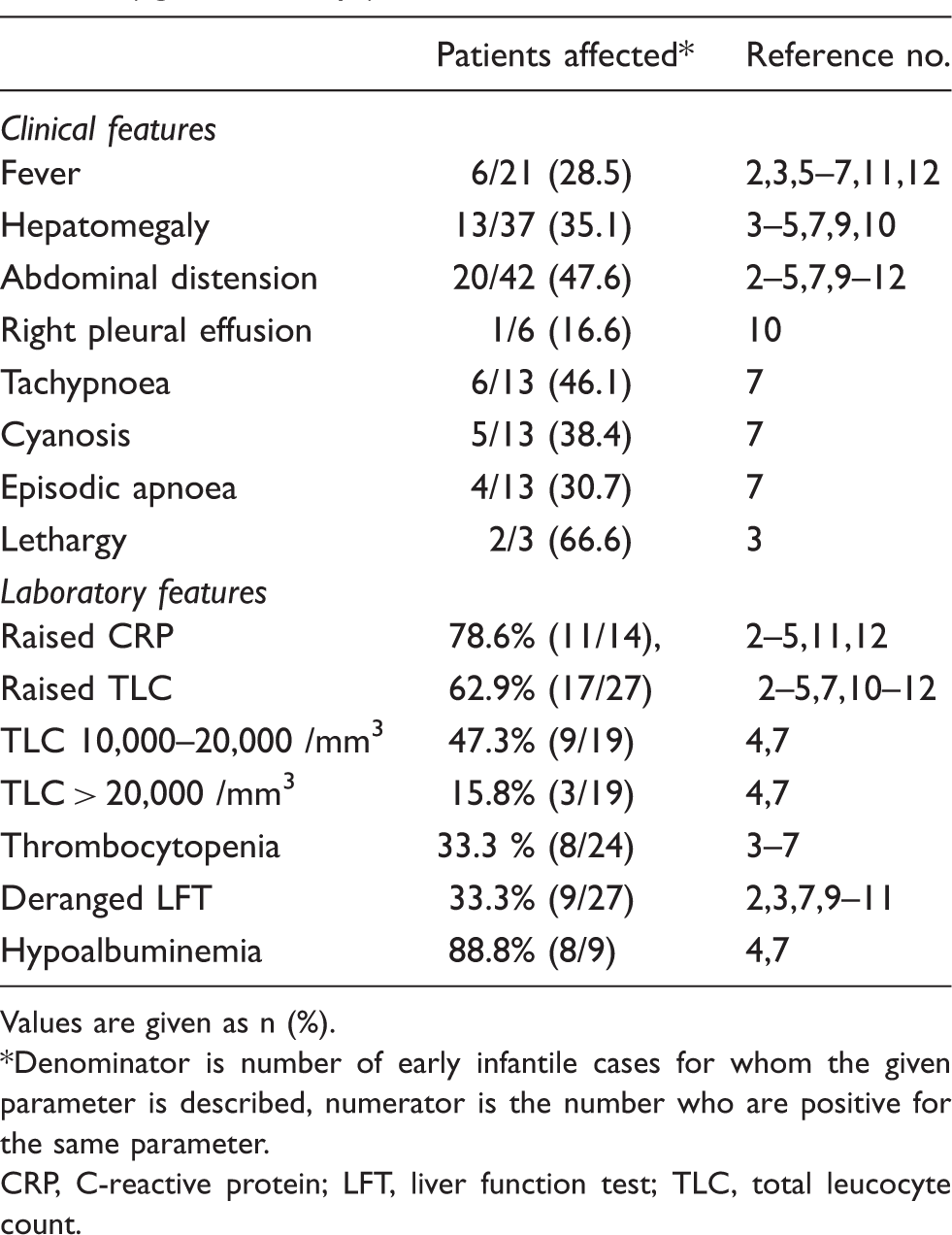
Values are given as n (%).
Denominator is number of early infantile cases for whom the given parameter is described, numerator is the number who are positive for the same parameter.
CRP, C-reactive protein; LFT, liver function test; TLC, total leucocyte count.
Liver abscesses in infancy are usually multiple and involve both lobes of the liver as was seen in two of our cases. 7,9 –11 The most common bacteria found are Staphylococcus aureus, Streptococcus pyogenes and E. coli, 2 although any organism can potentially be responsible in this age group. 9 Treatment includes injectable antibiotics for 3–6 weeks covering both Gram-positive and Gram-negative species as well as anaerobic organisms. 4 Multiple abscesses are usually treated conservatively with antibiotics, while image-guided percutaneous needle aspiration or catheter drainage is recommended in solitary abscess, particularly if large. 12
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.