
Abstract
Coagulase-negative staphylococci (CoNS) are frequently isolated from wound infections. There are limited data examining the prevalence of methicillin-resistant CoNS (MRCoNS) among Egyptian patients after surgery. Thus, we studied 208 hospitalised patients, who had skin and soft tissue infections (SSTIs) due to various causes. Samples were cultured for isolation and identification of CoNS and isolates were screened for susceptibility against 23 different antimicrobials. Out of 241 Staphylococcal isolates, 114 (47.3%) were CoNS. The prevalence of MRCoNS among surgical site infection, diabetic foot, abscess, and burn patients was 13.4%, 11.5%, 15.6%, and 10.3%, respectively. The lowest resistance of the 27 identified MRCoNS isolates was to vancomycin, amikacin and gatifloxacin (7% each). We conclude that CoNS isolates are major pathogens associated with wound infections at our institution and MRCoNS probably poses a substantial threat for patients in Egypt, though most MRCoNS isolates demonstrated susceptibility to vancomycin.
Introduction
Since methicillin emergence and its wide clinical application, methicillin-resistant coagulase-negative staphylococci (MRCoNS) became dominant and an integral cause of nosocomial infections. This led to an increase in reported numbers of cases, as well as death rates both in hospital and community. 1 We previously reported that S. aureus was found in 61% of patients with surgical site infection (SSI), with methicillin resistant S. aureus (MRSA) prevalent in 14.9%. 2 There are limited data examining the prevalence of MRCoNS among Egyptian patients after surgery.
Subjects and methods
Patients enrolled were emergency cases admitted to the General Surgery Department of Minia University Hospital (MUH) for different surgical interventions, but suffering from SSTIs, defined according to the Center for Disease Control classification. A total of 208 subjects (143 (69%) males) of ages ranging from 2 months to 79 years, mean age (±SD) of 44.4 ± 15.8 years, were enrolled in our study between November 2007 and August 2010. They were all administered one of the available third generation cephalosporins (e.g. Ceftriaxone or Cefoperazone) 24 h before surgery. Our study protocol was approved by the College of Pharmacy Council, the Dean of the Faculty of Medicine and the Director of MUH and each subject consented prior to participation. All research procedures were carried out in accordance with the Helsinki Declaration. Parents of children included in the study approved their participation. Sterile swabs were used to collect the samples from hospitalised patients. Specimens were randomly selected from different infected skin and soft tissue sites and were collected prior to antibiotic administration as follows: (SSI; n = 82), diabetic foot (n = 52), abscess (n = 45) and burn infections (n = 29).
Collected swabs were cultured on mannitol salt agar (Becton Dickinson, USA) and nutrient agar (Oxoid, England), then incubated at 37℃ for 24 h and examined microscopically using Gram-stained smears. Cultures were characterised, and sub-cultured for the separation of mixed colonies on mannitol salt agar and blood agar. Catalase and coagulase, as well as other biochemical tests, were performed for identification of all the isolates following standard procedures. 3
Antimicrobial susceptibility testing was performed on Mueller-Hinton agar (Oxoid, England). The minimum inhibitory concentrations (MICs) were determined by agar dilution method according to Clinical Laboratory Standard Institute (CLSI) guidelines 4 to determine the sensitivity and resistance of the isolates to β-lactams and other antimicrobials.
Antimicrobial susceptibility testing for CoNS was performed by the disc diffusion method using oxacillin disks, 5 and confirmed by MIC testing. The following antimicrobial agents were tested: Ampicillin and Chloramphenicol (SEDICO, Egypt), Amoxicillin and Cefotaxime (EIPICO, Egypt), Oxacillin, Ampicillin/Sulbactam, Ciprofloxacin, Ofloxacin, Gatifloxacin, Levofloxacin, Clindamycin and Tetracycline (Sigma, USA), Cephalexin and Cefuroxime (Glaxo-Welcome, Egypt), Cefoperazone (Pfizer, Egypt), Cefepime and Amikacin (Bristol-Mayer’s Squibb, Egypt), Amoxycillin/Clavulanate (Beecham Pharmaceuticals, Egypt), Gentamicin (Memphis Company for Pharmaceutical and Chemical Industries, Egypt), Norfloxacin and Vancomycin (Lilly, USA), Erythromycin (WIN LAB, Harborough, England) and Rifampicin (El-Nasr, Egypt). The disc diffusion test was described 6 as giving an inhibition zone ≤10 mm indicating oxacillin-resistance, ≥13 mm indicating oxacillin-sensitivity and 11–12 mm indicating intermediate resistance.
Results
Prevalence of CoNS and MRCoNS species isolated from patients suffering from different wound infections at MUH.
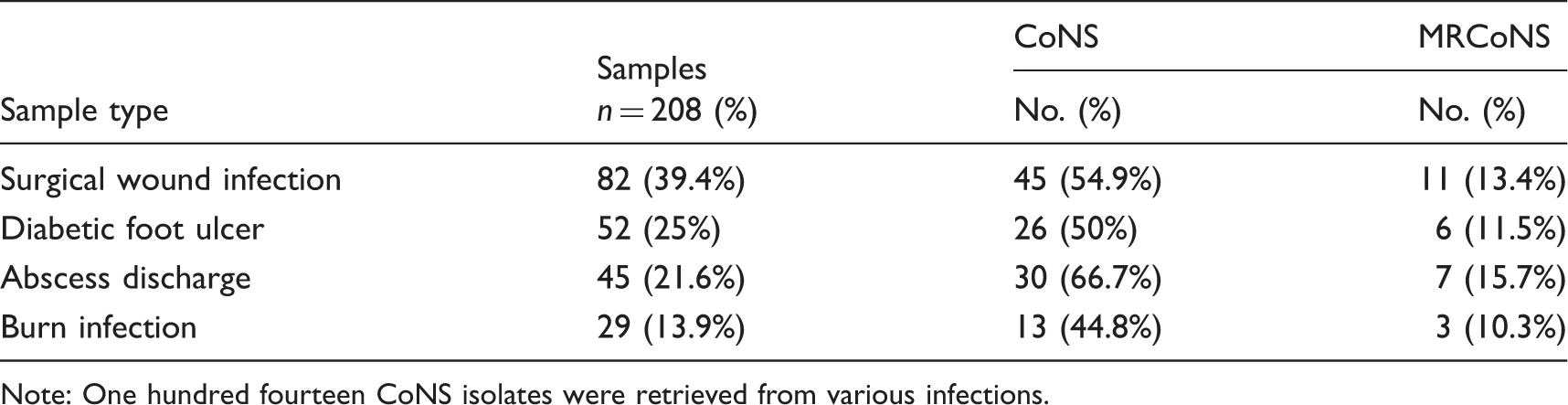
Note: One hundred fourteen CoNS isolates were retrieved from various infections.
Susceptibility of CoNS wound isolates to β-lactams and other antimicrobials.
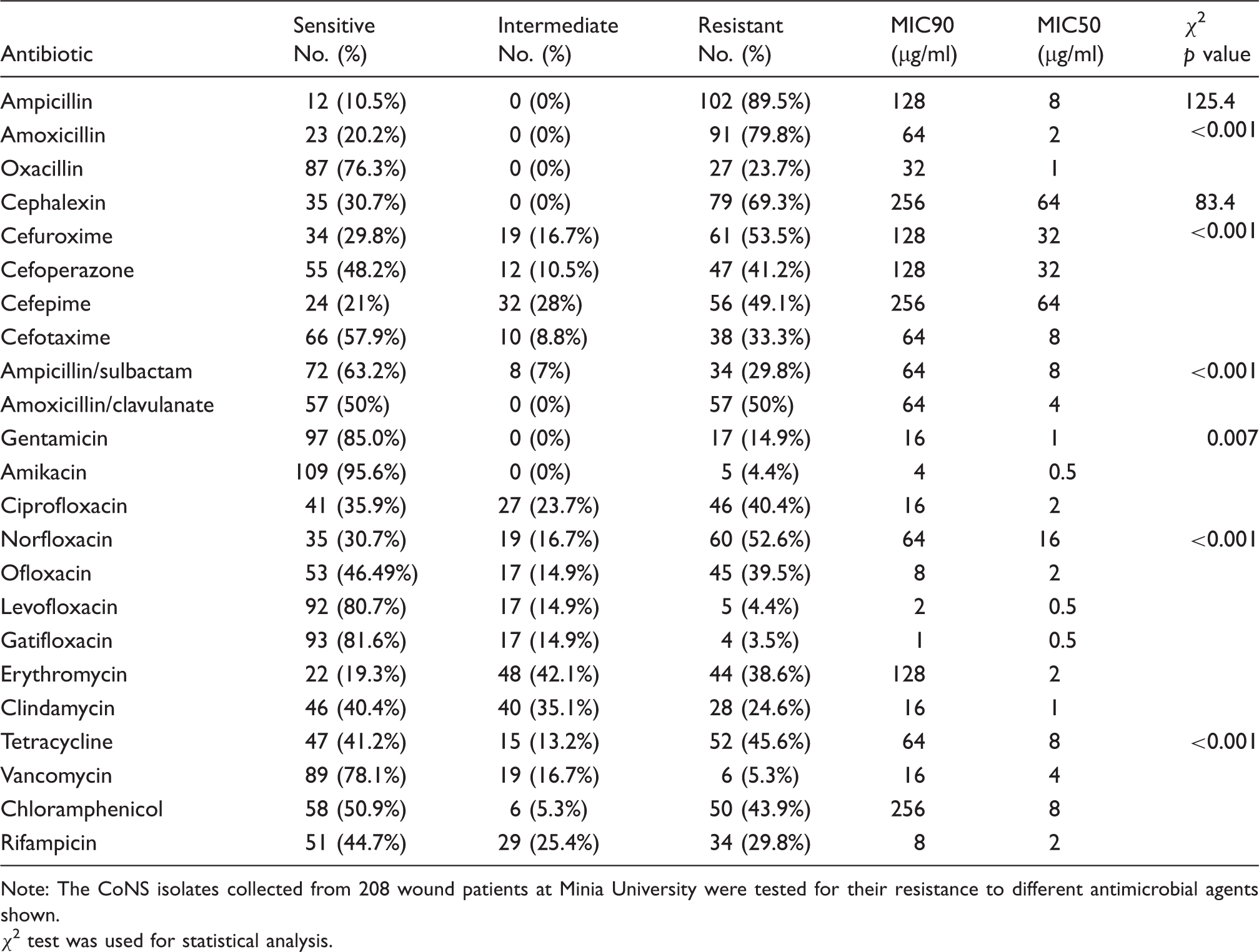
Note: The CoNS isolates collected from 208 wound patients at Minia University were tested for their resistance to different antimicrobial agents shown.
χ2 test was used for statistical analysis.
Susceptibility of MRCoNS isolates to antibiotic groups.
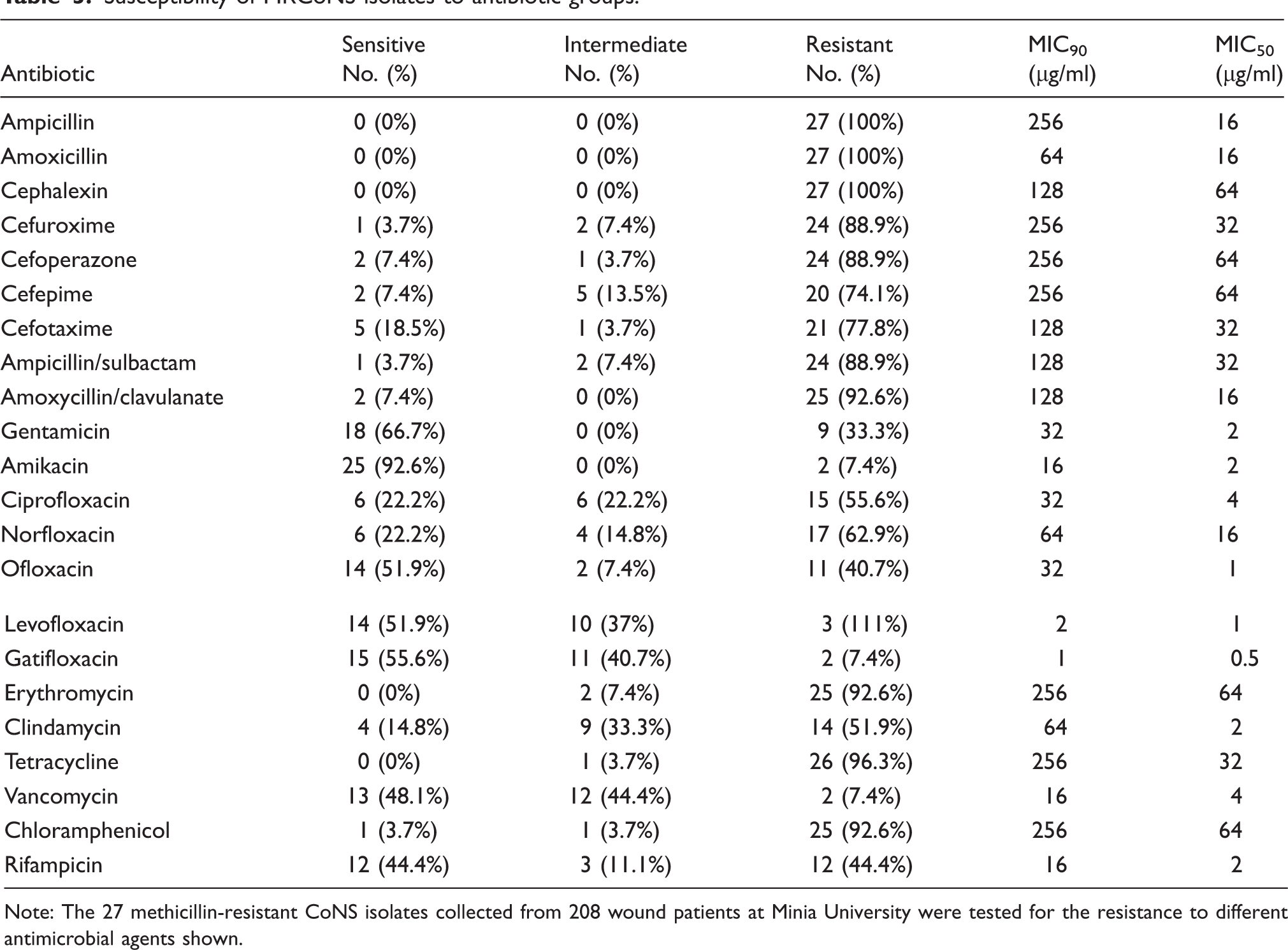
Note: The 27 methicillin-resistant CoNS isolates collected from 208 wound patients at Minia University were tested for the resistance to different antimicrobial agents shown.
Discussion
The prevalence of CoNS and MRCoNS was not substantially different in different types of infections, indicating no preferential association with a particular type of SSTI. CoNS was very common in line with findings of other studies.7–9 For a long time, CoNS were considered as commensals and were rarely reported to cause severe infections. However, probably as a result of the combined effect of increased use of intravascular devices and the increase in the number of hospitalised immunocompromised patients, CoNS has emerged as a major cause of nosocomial blood stream infections. 10 In addition, as Staphylococcus epidermidis makes up a significant part of normal bacterial flora of the human skin and mucous membranes, it is easily introduced as a contaminant during the surgical implantation of polymeric devices. 11 A high proportion of clinical CoNS isolates express the mecA gene, which is responsible for beta-lactam antibiotic resistance. This has implications for the choice of the antibiotic administered. 12
Whilst the vast majority (93%) of CoNS cases in our study were susceptible to vancomycin, the emergence of vancomycin resistance (although currently small) may be indicative of an emerging trend. Possible antibiotic abuse, and the appearance of genetic mutations warrant further research as to the cause. High resistance, however, to ampicillin, amoxicillin and cephalexin and moderate resistance to oxacillin, ampicillin/sulbactam, cefotaxime, cefoperazone cefepime, amoxycillin/clavulanic acid and cefuroxime have been well documented previously in numerous studies. However, most strains show susceptibility also to amikacin and gatifloxacin. Our conclusion is that MRCoNS warrants similar attention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from Minia University and personal funds.