
Abstract
Idiopathic systemic capillary leak syndrome (ISCLS) is a potentially fatal disorder characterised by ‘attacks’ of varying intensity of hypovolemic shock in association with haemoconcentration and hypoalbuminaemia. It is a disease of exclusion, and the severity of attacks may mimic sepsis at presentation. We report a case of a lady with recurrent attacks of ISCLS with at least two life-threatening episodes, having been treated elsewhere as a case of steroid insufficiency. The diagnosis is often challenging, and treatment of an acute episode involves the judicious use of fluids and vasopressors, as required. Prophylaxis to prevent further attacks is of varied success.
Case report
A 44-year-old lady presented with complaints of episodic swelling of the body for three years’ duration. Each episode, occurring once in five to six days, began with body aches, nausea, fatigue (prodromal phase) and a feeling of sudden weight gain and puffiness of the face (leak phase) with a reduced urine output lasting for a maximum of 48 h, followed by diuresis and resolution of symptoms (recovery phase). On some occasions, the symptoms were severe enough to cause hypotension and breathlessness requiring intensive care. The severity of each episode was dependent on factors such as exposure to hot climates and strenuous activity. She was evaluated elsewhere and was treated with danazol and glucocorticoids considering the possibility of angioneurotic oedema or cortisone deficiency.
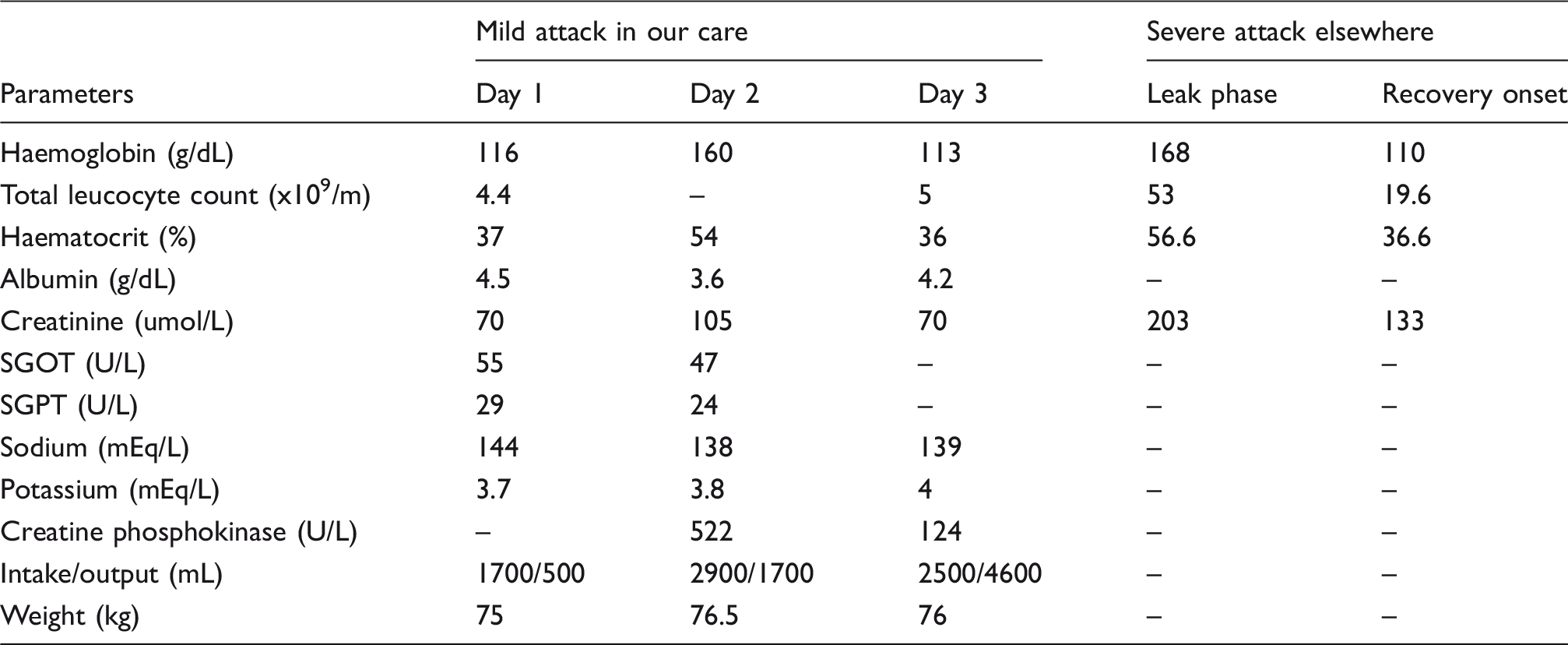
Lab parameters during the mild attack during hospital stay and limited data during an attack treated elsewhere.
Following literature review, we narrowed the diagnosis to ISCLS based on the following points:
Recurrent episodes of typical symptoms suggestive of the three phases of ISCLS Haemoconcentration and hypoalbuminaemia during the episode Presence of monoclonal gammopathy No evidence suggestive of infection, drug allergy, anaphylaxis or angioedema
She was started on prophylactic intravenous immunoglobulin (IVIG) (1.5 g/kg/month). Following this, the episodes of capillary leak decreased significantly with no severe episodes thereafter and only mild episodes when the immunoglobulin dose was delayed by more than four weeks. She has now received seven doses of immunoglobulin and is being followed up.
Discussion
ISCLS is a rare disorder characterised by episodes of hypotension, hypoalbuminemia and hemoconcentration due to leakage of plasma and proteins into the interstitial compartment. 1 The disease is more common in middle age without any gender predeliction. 2 Several hypotheses have been proposed such as the presence of paraproteins, endothelial cell apoptosis and increased interleukin 2 expression.3–5
Attacks of ISCLS typically demonstrate three phases: a prodromal, leak and recovery phase. The frequency and severity of attacks vary significantly. The prodromal phase is characterised by symptoms such as fatigue, nausea, myalgia and a sudden increase in body weight. This is followed by a leak phase within one to four days, which is characterised by the triad of hypotension, haemoconcentration and hypoalbuminaemia. A rapid drop in the white blood cell counts from 53 to 19/m9 was suggestive of a non-infective aetiology and could be attributed to haemoconcentration. However, we acknowledge that this initial value was recorded elsewhere and not at our centre.
The leak phase is usually followed by a recovery phase during which the extravasated fluid is recruited into the intravascular compartment, and the patient is at an increased risk for volume overload. 6 Our patient had approximately five to six attacks per month with an average of two severe attacks per year.
Various treatment modalities such as corticosteroids have been tried in acute settings without success. Theophylline plus terbutaline has been used with lack of good evidence. 7 We found a good response to IVIG and observed that the attacks resolved almost completely. The mechanism of action of IVIG in preventing ISCLS is unclear, but probably arises through its immunomodulatory effects. 8
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Remya Rajan https://orcid.org/0000-0003-4136-9843 Nitin Kapoor ![]()