
Abstract
Iron deficiency, the commonest cause of anaemia in children, is a global public health problem. Worldwide, almost 50% of children <5 years of age are anaemic. Platelet count in iron deficiency anaemia is mostly normal or high; thrombocytopenia is rare. We describe two children with iron deficiency anaemia and severe thrombocytopenia who recovered with iron supplementation alone.
Case 1
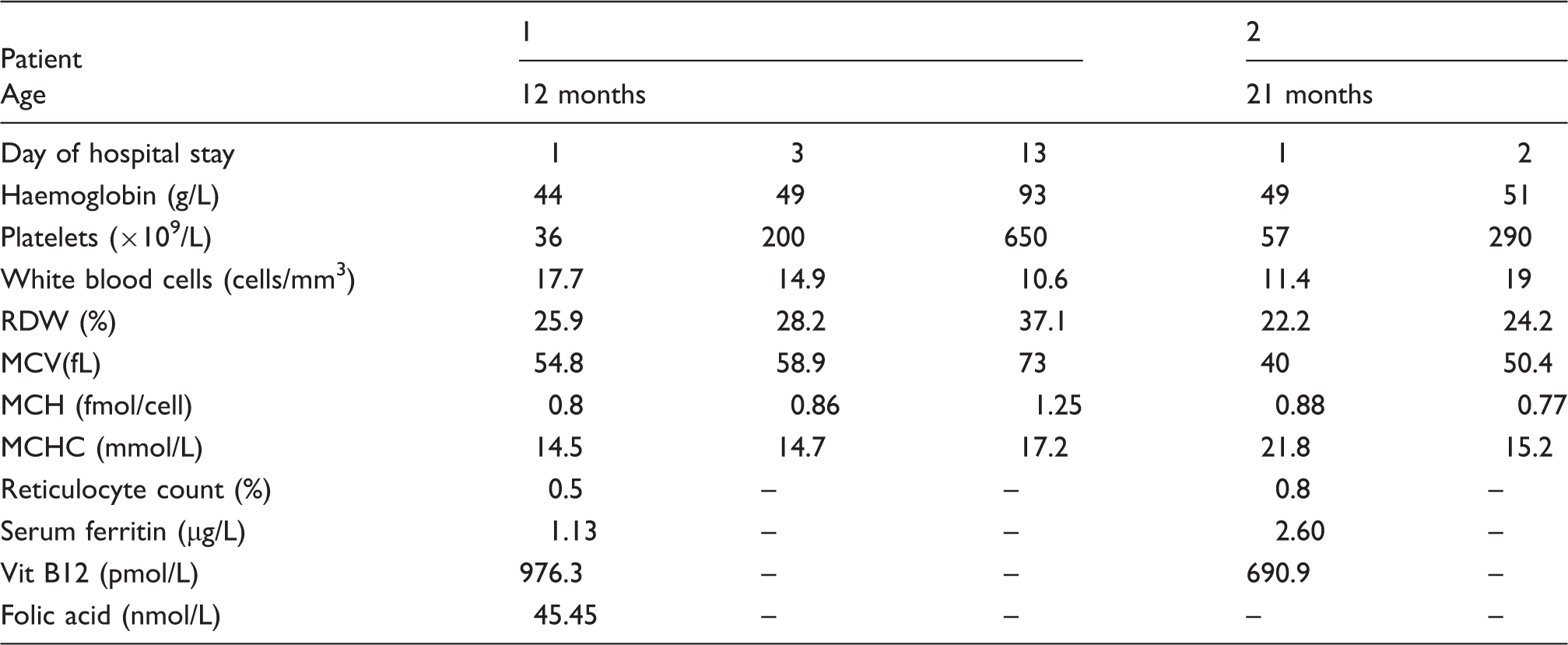
Haematological parameters and response to treatment.
Case 2
A 21-month-old boy was referred with poor appetite and fever of one week’s duration. Born at term, he was fed breast milk and formula milk till six months of age and was subsequently on a predominant cow milk-based diet (150–170 mL cow milk/day). Examination, except for sever pallor, was unremarkable. The full blood count showed microcytic, hypochromic anaemia suggestive of iron deficiency but again, thrombocytopenia was present (Table 1). Other investigations and management were similar to Case 1. The platelet count was normal by day 3 and haemoglobin by day 10 of treatment.
Neither children described above had high grade fever, bleeding, lymphadenopathy or hepatosplenomegaly. Hence, bone marrow aspiration and biopsy were deferred.
Discussion
Diagnosis of iron deficiency anaemia (IDA) is made by clinical evaluation and assessment of the haemoglobin and serum ferritin level. 1 Platelet count in IDA is usually normal or high.2,3 Thrombocytopenia is rare.4–7 In such a scenario, diseases involving two cell lines such as vitamin B12 deficiency, folic acid deficiency, haematological malignancy, aplastic anaemia and Evan’s syndrome need to be considered.
Thrombocytopenia with IDA was initially described in the 1960s but severe thrombocytopenia was rare and associated with severe IDA.4,5 Bone marrow aspirates show erythroid hyperplasia and decreased number of megakaryocytes which normalised in 7–10 days after iron therapy. 5 Increase in the platelet count following iron therapy is brisk, occasionally as dramatic as tripling of the initial value within 24 h treatment, as seen in both our children (Table 1).5–7
An interesting study in adults showed that patients with thrombocytopenia with IDA, compared to those with immune thrombocytopenia, had relatively higher platelet counts and lower mean platelet volume. 8 The cause of thrombocytopenia in IDA is unclear. One mechanism proposed is increased red cell production at the cost of reduced platelet production due to stem cells common to both lineages competing for the available iron. The other mechanism proposed is a dysfunctional iron-dependent cellular process in the later phase of thrombopoiesis. 6
Despite IDA being widespread in low-resource countries, severe thrombocytopenia with IDA has surprisingly not, to our knowledge, been reported before.
In children with severe IDA, a comprehensive clinical evaluation and careful analysis of the basic laboratory tests are essential to look for red flags. A trial of iron therapy may avoid extensive investigations such as bone marrow evaluation and potentially harmful therapy including platelet transfusion or steroids, thereby reducing discomfort and cost. Rising platelet count seems to be an early and reliable marker of response to iron therapy. Underlying mechanisms responsible need further study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.